


Many technologies used in dentistry are evolving and we must keep up with the progress. My interest in various laser and light therapies has recently led me to discovering new and emerging uses of BLUE light which I was not aware of, so I plunged into literature to learn more and what I found pleasantly surprised me. So, I would like to share my findings with the reader.
Past
Historically blue and UV curing lights have emerged at the same time as composites offering command cure versus chemically cured first composites of the 1960’s. Since then, the uses of light have evolved into four different categories by usage: 1. Curing lights, 2. Power bleaching lights, 3. Cleaning and disinfecting tools, 4. Surgical tools. Let us look a little closer at each category. A recent review published by Fornaini et. al.,1 screened over 500 studies about uses of blue/violet lasers and LEDs in dentistry, and 47 were included in their analysis. Most of the investigations focused on photo-polymerization of composites, followed by tissue decontamination, photo-bio-modulation (PBM) and oral surgery, with very few on periodontics, orthodontics, bleaching and endodontics.
Curing lights have evolved from halogen lamps to plasma arc lamps (Sapphire) to blue LED’s (Valo) to finally blue diode 445nm laser called “Monet” by AMD lasers, the same company that gave us “Picasso” 810nm diode surgical laser. The trend is to offer deeper cure in shorter time and without any thermal side-effects on the pulp. Of course, shorter cure time goes hand-in-hand with lower pulpal temperature increase. The Monet diode laser yields comparable results to halogen lamps and LEDs in terms of curing depth and temperature elevation in 1 second vs 20-40 seconds.
Adjunctive use of blue light in vital bleaching started around 25 years ago with first Zoom mercury metal halide lamps 350-400nm in wavelength, followed by plasma arc lamps (Sapphire) and Blue LED’s (Zoom 4). Activation of hydrogen peroxide breakdown and heating of the bleaching gel improved the time needed for in-office bleaching, if not the efficacy of the treatment. Increase in pulpal temperature and post-operative sensitivity remain a concern for long term light application.
Present
Lasers have come in offering to reduce treatment time and post-operative sensitivity while offering better color improvement. Different colorants are added to the bleaching gels to help focus the light energy on the gel and not allowing it to penetrate through the tooth structure towards the pulp. Affinity for pigment and hemoglobin keeps the laser energy within the gel, thus increasing temperature of hydrogen peroxide and speeding up its breakdown into ROS (reactive oxygen species), which in turn break down colored molecules within hydroxyapatite (Fig. 1).
Fig. 1A

Fig. 1B

Mobius et.al. compared bleaching efficiency of 445nm blue diode laser and infrared (IR) diode laser 940nm with surgical versus bleaching handpiece, 970nm diode laser with surgical handpiece and bleaching alone without laser activation. The results showed that laser activated bleaching was more effective than conventional bleaching and 445nm blue laser performed the best giving the highest change in VITA shade color followed by 940nm laser using bleaching wand.2
Infrared (IR) diode lasers have been utilized in soft tissue surgery since the 1980s, yet most practitioners still don’t fully understand the benefits of laser surgery over scalpel or electro-surgery. For this to change, lasers must become a part of undergraduate curriculum and laser training should be mandatory, and not optional, for the doctors considering using this technology to its fullest benefit. Blue surgical diode laser first entered the dental market as Sirona BlueLase in 2016 as one of the first multi-wavelength lasers offering disinfection (blue), cutting (IR) and PBM (red). But since then, research confirmed that blue wavelength is not only good for disinfection (being a close neighbor to UV ultraviolet spectrum) but is also superior in cutting due to highest affinity to pigment and hemoglobin. A randomized control study by F. Sobouti et. al.3 compared frenectomy done with 445nm blue diode with IR 980nm diode and scalpel. Diode laser frenectomy in general resulted in lower intra- and post-operative complications compared to the scalpel, and 445 nm laser was significantly superior to 980nm. Just to list some of the benefits: best temperature control with best quality of incision, better efficiency, scant signs of inflammation, no bleeding and high compliance from patients and great capacity for coagulation, coupled with very low penetration depth and minimal thermal side-effects.
Blue light as a disinfecting agent is not too far-fetched since the bactericidal and anti-viral effects of UV light are well known. Photons of UV light carry higher energy and are able to destroy bacteria by breaking chemical bonds which keep cell membranes intact. Blue light photons are of lower energy but are also less dangerous to use on patients and for us as operators. Blue light wavelengths can interact with endogenous photosensitizing molecules like Porphyrins and Flavins. The absorption of blue energy photons will bring about excited triplet state and subsequent transfer of this energy to stable molecular oxygen will lead to dissociation into two singlet oxygens (ROS), thus damaging bacterial cell membrane leading to leakage and cell death.4 Scientific literature in the past 10 years is full of investigations supporting the use of blue light in the treatment of MRSA and E.coli infections in the hospitals,5 healing skin burns,6 and anti-viral properties against HSV-1.7 Photo-dynamic therapy using blue light with various photo-sensitizers have been shown effective in reduction of both periodontal pathogens and anti-caries therapy against S.mutans and L. salivarius.8-14 Companies like MRM, Multi Radiance Medical (Solon, Ohio) are leading the way in evidence based non-surgical applications of light therapy by incorporating red, IR and blue LED’s, along with super-pulsed IR diode low level laser to offer simple to use portable devices to help clinicians treat common dental conditions like cold sores, chancre sores (Fig. 2), oral mucositis, post-surgical surface wound disinfection and pain management (Fig. 3A, 3B), dry socket (Fig. 4), burning mouth syndrome (Fig. 5) and healing defects like BRONJ (bis-phosphonate related osteo-radio-necrosis of the jaw) (Fig. 6).
Fig. 2

Fig. 3A

Fig. 3B

Fig. 4
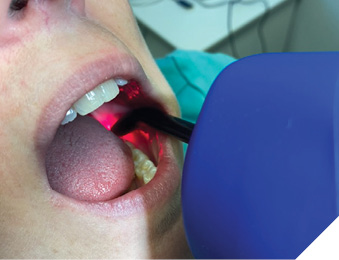
Fig. 5

Fig. 6

Future
Pretty soon we might have a scientifically proven protocol which uses curcumin mouthwash followed by a couple of minutes of blue LED activation as a prophylaxis against caries in children, orthodontic patients, and seniors with reduced salivary flow. If this is proven to have equal anti-bacterial efficacy to our conventional go-to prescription of chlorhexidine, but without all the nasty side-effects such as staining, taste alteration, fibroblast inhibition and antibiotic resistance, I believe everyone would jump on board this “Blue Light Train”.
How about treating and preventing peri-implantitis from inside the implant? As zirconia implants are gaining popularity over the titanium ones, L. Zhang et. al.14 are proposing a way to insert a tiny wireless blue LED inside the zirconia implant and irradicating pathogens such as P.intermedia and P.gingivalis within 10 minutes using a uniform 3-D blue glow from within the implant.
Conclusion
I believe the future of dentistry is bright. Bright BLUE to be specific! 
Oral Health welcomes this original article.
References
- C.Fornaini, R. Fekrazad, J.P. Rocca, S. Zhang, E. Merigo. Use of Blue and Blue-Violet Lasers in Dentistry: a Narrative Review. J Lasers Med Sci 2021;12:e31.
- D. Mobium, A. Braun, R. Franzen. Evaluation of tooth color change after a bleaching process with different lasers. Odontology, 2024;112, 872-883.
- Sobouti et al. Maxillary labial frenectomy: a randomized, controlled comparative study of two blue (445 nm) and infrared (980 nm) diode lasers versus surgical scalpel. BMC Oral Health (2024) 24:843. doi.org/10.1186/s12903-024-04364-w
- K.Rupel et al. Blue laser light inhibits biofilm formation in vitro and in vivo by inducing oxidative stress. npj Biofilms and Microbiomes (2019) 5:29; doi.org/10.1038/s41522-019-0102-9
- Amodeo, D.; Manzi, P.; De Palma, I.; Puccio, A.; Nante, N.; Barcaccia, M.; Marini, D.; Pietrella, D. Efficacy of Violet-Blue (405 nm) LED Lamps for Disinfection of High-Environmental-Contact Surfaces in Healthcare Facilities: Leading to the Inactivation of Microorganisms and Reduction of MRSA Contamination. Pathogens 2023;12,1338. doi.org/10.3390/pathogens12111338
- J.A.F.Neto, T.M.S. Simões, T.K.B. de Oliveira, J.S. Pereira, C.F.W. Nonaka, M.H.C,V. Catão. Effects of photobiomodulation with blue Light Emitting Diode (LED) on the healing of skin burns. Lasers in Med Sci (2023) 38:275. doi.org/10.1007/s10103-023-03929-5
- Zupin L. Antiviral properties of blue laser in an in vitro model of HSV-1 infection. Microbiol Immunol 2018;62:477-479. doi:10.1111/1348-0421.12600
- Hirose M, Yoshida Y, Horii K, Hasegawa Y, Shibuya Y, Efficacy of
- antimicrobial photodynamic therapy with Rose Bengal and blue light against cariogenic bacteria, Archives of Oral Biology (2020), doi.org/10.1016/j.archoralbio.2020.105024
- D.P. V. Leite, F. R. Paolillo, T. N. Parmesano, C.R. Fontana, V.S. Bagnato. Effects of Photodynamic Therapy with Blue Light and Curcumin as Mouth Rinse for Oral Disinfection: A Randomized Controlled Trial. Photomedicine and Laser Surgery. 2014; v32(11), 627–632. doi: 10.1089/pho.2014.3805
- N.C. Araujo, R.F. de Menezes, V.S.M. Carneiro, A.P. Santos-Neto, C.R. Fontana, V.S. Bagnato, C.M. Harvey, M.E.M. Gerbi. Photodynamic Inactivation of Cariogenic Pathogens Using Curcumin as Photosensitizer. Photomedicine and Laser Surgery 2017;35(5),259–263.doi: 10.1089/pho.2016.4156
- B.H.D. Panariello, E.A.M. Cavichioli, S.F. Sochacki, L.G.G.Junior, S. Duarte. Blue light & chlorhexidine therapies on Streptococcus mutans biofilm and its regrowth on an in vitro orthodontic model. AJO-DO 2020. doi.org/10.1016/j.ajodo.2020.06.050
- De Lucca, A.J.; Carter-Wientjes, C.; Williams, K.A.; and Bhatnagar, D., Blue light (470 nm) effectively inhibits bacterial and fungal growth. Letters in Applied Microbiology 2012;55, 460–466. doi:10.1111/lam.12002
- G.F. Gomez, R.Huang, M. MacPherson, A.G. F. Zandona, R.L. Gregory. Photo Inactivation of Streptococcus mutans Biofilm by Violet-Blue light. Curr Microbiol. 2016. doi 10.1007/s00284-016-1075-z
- S. Böcher, J-S Wenzlera, W. Falk, A. Brauna. Comparison of different laser-based photochemical systems for periodontal treatment. Photodiagnosis and Photodynamic Therapy 27 (2019) 433–439. doi.org/10.1016/j.pdpdt.2019.06.009
- L. Zhang, Y. Li, L. Yuan, Q. Zhang, Y. Yan, F. Dong, J. Tang, Y. Wang. Advanced and Readily-Available Wireless-Powered Blue-Light-Implant for Non-Invasive Peri-Implant Disinfection. Adv. Sci. 2023,10,2203472. doi:10.1002/advs.202203472
About the author

Marina Polonsky, DDS, MSc, is a gold medal University of Toronto ’99 graduate, she maintains private general practice in Ottawa, Ontario with focus on multi-disciplinary treatment utilizing lasers of different wavelengths. She holds a Mastership from World Clinical Laser Institute (WCLI), Master of Science in Lasers in Dentistry from RWTH University in Aachen, Germany. She is the founder of the Canadian Dental Laser Institute (CDLI), the only study club affiliated with the Academy of Laser Dentistry. She serves on the Executive Committee for Oral Health and is the editor of the Laser Dentistry issue.