
Abstract
Chronic, severely localized periodontal infections at the site(s) of planned tooth extraction commonly give rise to a layer of granulomatous and epithelialized tissue encompassing the apex of the tooth root. Despite its typical disposal, this epithelialized granulomatous tissue can be effectively employed for primary closure, capitalizing on the biological mechanisms of wound healing. Introducing a pioneering approach termed the Leon’s Everted Gingival Pouch (LEGP) technique, the authors advocate for the comprehensive utilization of the epithelialized granulomatous tissue to facilitate the containment of bone graft material, manage soft tissue, and achieve primary closure in a single surgical procedure. The LEGP technique offers a viable alternative for tooth extraction, socket preservation, or immediate implant placement, obviating the necessity of periosteal release. This article expounds upon the intricacies of the LEGP technique and elucidates its application through the presentation of two compelling case reports.
Key words
Leon’s Everted Gingival Pouch (LEGP) technique, Gingival Revitalization, vertical tooth mobility, Leon Chen classification for vertical tooth mobility, Leon’s Vertical Mobility, Vertical Mobility Index (VMI), inverted gingival pouch, everted gingival pouch
The attainment of primary stability, primary closure, tissue regeneration, and optimal wound healing is pivotal in ensuring the predictable osseointegration of dental implants.1 However, a significant number of patients seeking implant treatment are periodontally compromised, often characterized by teeth in a hopeless state that cannot be preserved due to a lack of bone-root contact, inadequate bone volume for implant placement, and/or severe local infection at the extraction site. Additionally, these patients may present soft tissue deficiencies, a thin gingival tissue biotype, or insufficient soft tissue, impeding the achievement of reliable primary closure and posing further challenges to long-term implant survival and the attainment of ideal esthetics.2,3
Traditionally, it has been recommended to thoroughly eliminate the granulomatous tissue that forms during the infection process in the socket as part of the debridement procedure following tooth extraction. In cases where there is severe vertical bone resorption, guided bone regeneration becomes essential to augment the bone height. This involves the placement of bone graft material and a collagen membrane in conjunction with either a laterally positioned flap or a coronally advanced flap, aiming to achieve optimal primary closure.3,4 Furthermore, a range of surgical techniques, such as free gingival grafts and pedicle flap techniques, are employed to correct or eliminate anatomic, developmental, or traumatic irregularities in gingival morphology.5-9 Subsequently, in order to attain successful primary closure, the implementation of soft tissue release flaps, connective tissue grafts, barrier membranes, and soft tissue replacement matrix techniques has been advocated.10
These historically time-consuming, expensive, and unattractive methods employed to reconstruct lost tissue after complete tissue removal from the extracted socket have yielded controversial clinical outcomes.2 Specifically, various factors (e.g., incision techniques, flap design, elevation, flap mobility, flap stability, and suturing) exert an influence on the clinical efficacy of augmentation and regeneration procedures.4,11 It is crucial for the flap to be capable of complete elevation and closure to facilitate bone regeneration, while also remaining immobile and undisturbed to ensure proper wound healing.12,13
However, the process of wound healing in periodontal tissue is intricate, encompassing inflammation, formation of granulomatous tissue, neo-vascularization, re-epithelization, and matrix remodeling.12 In the customary sequence, the formation of a clot occurs within the injured tissues, followed by the development of granulomatous tissue due to the infiltration of inflammatory, fibroblast, and endothelial cells. Subsequently, there is migration of epithelial cells to cover exposed surfaces, culminating in the maturation of the healing tissue matrix.13
Hence, the establishment and maturation of granulomatous tissue arise through a sequence of intricate cellular and molecular mechanisms, involving the infiltration of macrophages, fibroblasts, and neovascularization in a coordinated manner within the wound space.14 Functioning as a complex reservoir of cytokines and growth factors, granulomatous tissue comprises newly formed capillaries, macrophages, fibroblasts, and a component of loose connective tissue.13,15 The cytokines and growth factors within this tissue exhibit chemo-attractive, mitogenic, and other regulatory properties, which contribute to its epithelialization.
From this biological standpoint, the emergence of epithelialized granulomatous tissue is a manifestation of the intricate process of wound healing, demonstrating its capacity to resist local infections. It is justifiable to contemplate the comprehensive utilization of this epithelialized granulomatous tissue for achieving primary closure, rather than its removal. Building upon this foundation, L. Chen et al. introduced the groundbreaking Leon’s Everted Gingival Pouch (LEGP) technique in 2005,16 while first introducing in 2005, it was formally named as Inverted Ginginval Pouch (IGP). Leon’s Everted Gingival Pouch (LEGP) represents the inaugural approach for attaining primary closure that incorporates the incorporation of typically disregarded diseased epithelialized granulomatous tissue.16-18
Utility of granulomatous tissue
As the progression of periodontitis or other local infections ensues, a layer of granulomatous tissue forms, subsequently accompanied by the development of an epithelial lining that enwraps this tissue at the apex of the tooth root (i.e., the base of the affected socket following extraction).12-14 In accordance with the principles of the LEGP technique, this epithelialized granulomatous tissue can be delicately separated from the underlying bony layer within the socket immediately after extraction, and can be considered as a complete thickness entity.16-18 Consequently, the socket can be thoroughly debrided and cleansed, subsequently allowing the previously elevated epithelialized granulomatous tissue to serve as a housing medium for the bone graft material, acting as a barrier membrane for guided bone regeneration, and/or facilitating the incorporation of soft tissue grafts to manage the surrounding soft tissues.16-18
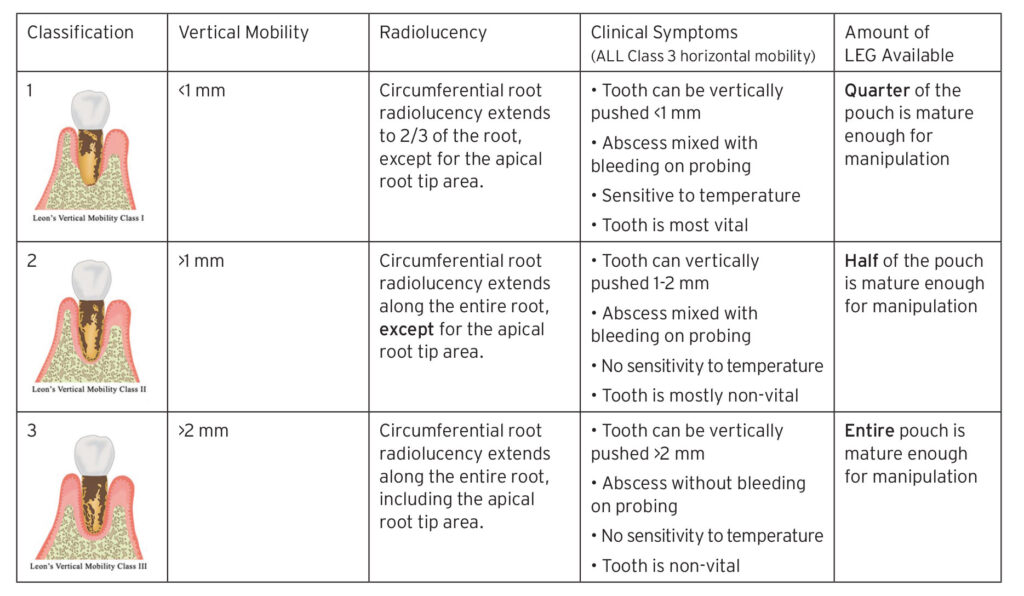
The preservation of the structural integrity of the granulomatous tissue and keratinized epithelium within the socket constitutes the foremost determinant in assessing the feasibility of implementing the LEGP technique. The appropriateness of employing the LEGP technique can be ascertained by evaluating the patient’s clinical symptoms and tooth mobility, as per Leon’s Vertical Mobility Classification (Table 1). In instances where the thickness of the epithelialized granulomatous tissue measures ≥ 2 mm and remains undamaged (e.g., falling under Leon’s Vertical Mobility Class III), the execution of the LEGP technique is deemed warranted.16-18
Therefore, following tooth extraction, it is crucial to conduct an assessment of the bone structure and examine the surrounding tissue. Another critical factor to consider is the presence or absence of bleeding following the extraction.10 If bleeding is absent, it indicates that the apical portion of the socket is entirely covered and encapsulated by epithelial tissue,10 thereby making the LEGP technique the preferred method of choice.
Everted Gingival Pouch (LEGP) technique
The utilization of the LEGP technique can offer advantages to a variety of patients, encompassing individuals with conditions such as gingival recession, tooth mobility, alveolar bone loss, and localized gingival infection, to name a few. This technique facilitates infection control, flap design, bone augmentation, soft tissue management, and simultaneous implant placement, streamlining these procedures into a single surgical intervention at the time of tooth extraction.16-18 By adopting this minimally invasive approach, the need for multiple regeneration surgeries, which have traditionally been linked to tooth extraction, bone augmentation, soft tissue regeneration, and implant placement, can be eliminated.16-18
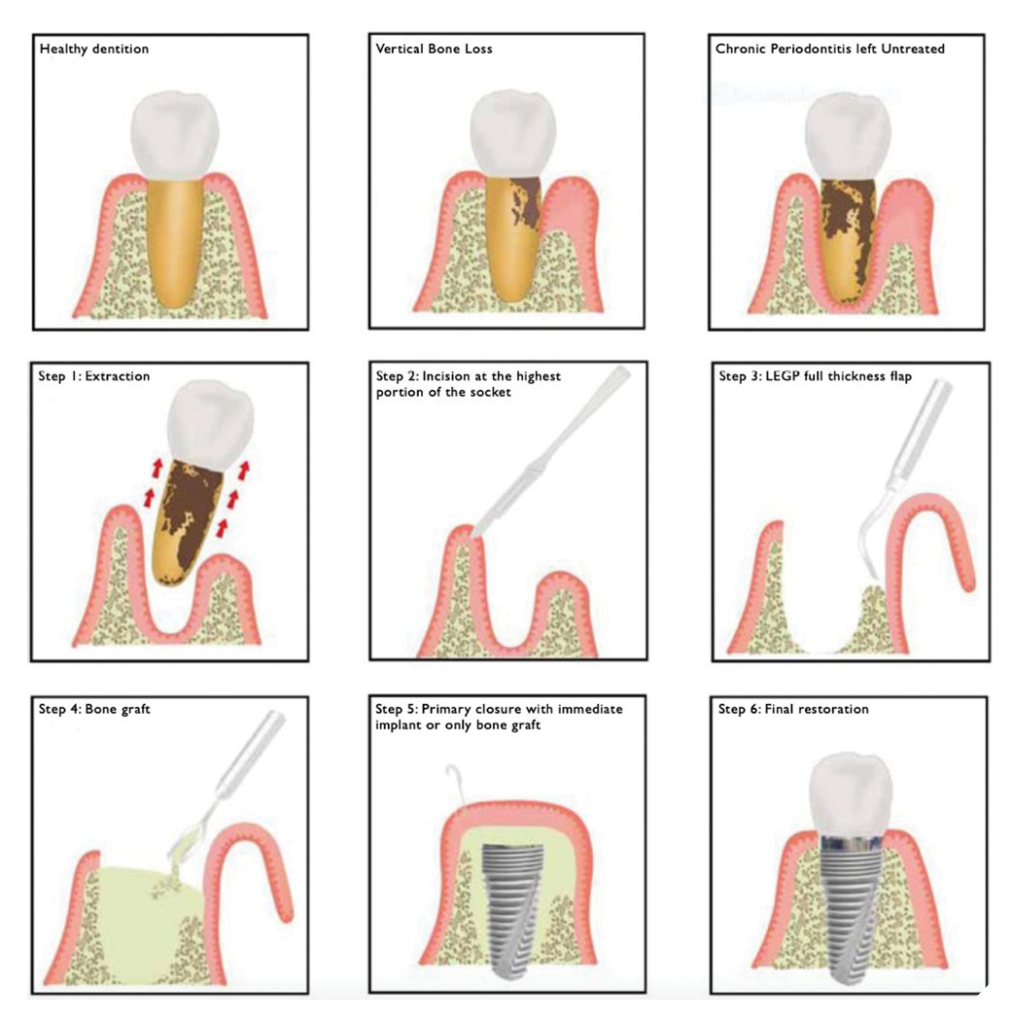
Protocol for the LEGP technique involves the following (Fig. 1):
- Extraction of the tooth with a poor prognosis (e.g., severe bone resorption; attachment loss).
- Making an incision at the crest of the alveolar ridge (ideally on the most prominent bony wall).
- Releasing a full-thickness flap of epithelialized granulomatous tissue from the incision on one side of the alveolar crest, across the base of the socket, to the opposing side of the crest.
- Packing the socket with bone graft material (Bio-Oss®, Geistlich Pharma North America, Inc.) in accordance with the principles of guided bone regeneration (GBR).
- Performing precise drilling to prepare and subsequently insert an immediate dental implant or exclusively implement GBR, both utilizing the previously elevated mature granulomatous tissue to achieve primary closure.
- Final restoration.
Fig. 1
The following case illustrations demonstrate the implementation of the LEGP technique in patients classified under Leon’s Vertical Mobility Class III. Instead of disregarding the diseased epithelialized granulomatous tissue, the authors fully utilized this tissue to achieve periodontal infection control, regeneration of the soft tissue (such as augmentation of keratinized tissue width and thickness), bone augmentation, enhanced esthetics, and heightened clinical efficiency.
Case presentation #1
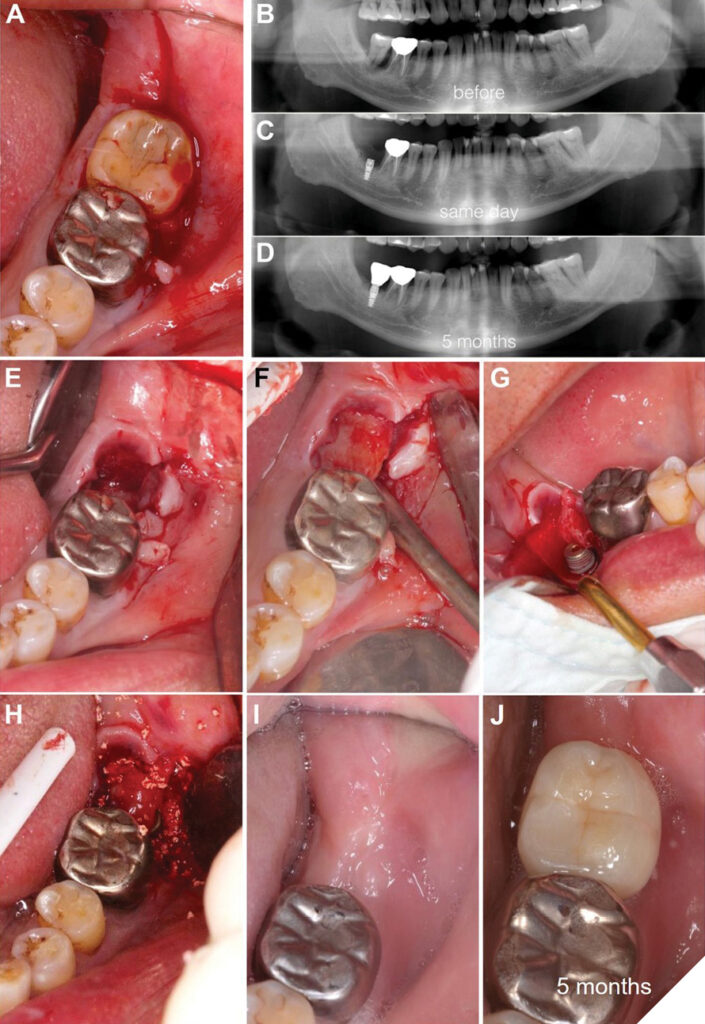
A 66-year-old male patient exhibited severe bleeding upon probing and vertical mobility exceeding 2 mm (i.e., categorized as Leon’s Vertical Mobility Class III) in relation to tooth #31 (Fig.2A). During the clinical evaluation, an abscess was observed, and the patient reported no sensitivity to temperature in the affected tooth. To validate these observations and evaluate the extent of tissue compromise, a preoperative panoramic radiograph was obtained (Fig. 2B). Subsequently, it was determined that implant therapy incorporating the LEGP technique was a viable option for this particular patient.
A gentle and non-traumatic extraction of tooth #31 was conducted employing forceps with minimal force applied (Fig. 2E), followed by a full thickness flap of the granulomatous tissue (referred to as the Leon’s Everted Gingival Pouch Flap [LEGP Flap]) from the socket at tooth #31 (Fig. 2F). This process involved the meticulous elevation of the mature epithelialized granulomatous tissue into a full thickness flap, utilizing a periosteal elevator.
The socket was subsequently curetted, debrided, and sounded to assess the exposed bone surface. Anorganic bovine bone grafting material (Bio-Oss®, Geistlich Pharma North America, Inc.) was meticulously placed into the socket to augment osseointegration and ensure long-term stability.
Following that, a tapered implant (NobleActive®, Nobel Biocare™) was immediately inserted (Fig. 2G), and primary stability was achieved near the apical portion of the implant, carefully avoiding proximity to the mandibular cortical nerve canal. Precise implant positioning was verified using a panoramic radiograph (Fig. 2C).
Beneath the granulomatous LEGP Flap (Fig. 2H), bone graft material (e.g., Bio-Oss®, Geistlich Pharma North America, Inc.) was meticulously positioned, facilitating primary closure. Since the LEGP Flap achieved passive primary closure, the placement of an artificial membrane was deemed unnecessary. To ensure uneventful wound healing and effective infection control, the patient was prescribed antibiotics (e.g., Augmentin 500 mg BID) to be taken twice daily for a duration of seven days.
During the 4-week follow-up appointment, the presence of esthetically pleasing and healthy keratinized gingival tissue was noted (Fig. 2I). After a healing period of five months (Fig. 2D), the implant was restored with a crown prosthesis (Fig. 2J).
Fig. 2A-J
Case presentation #2
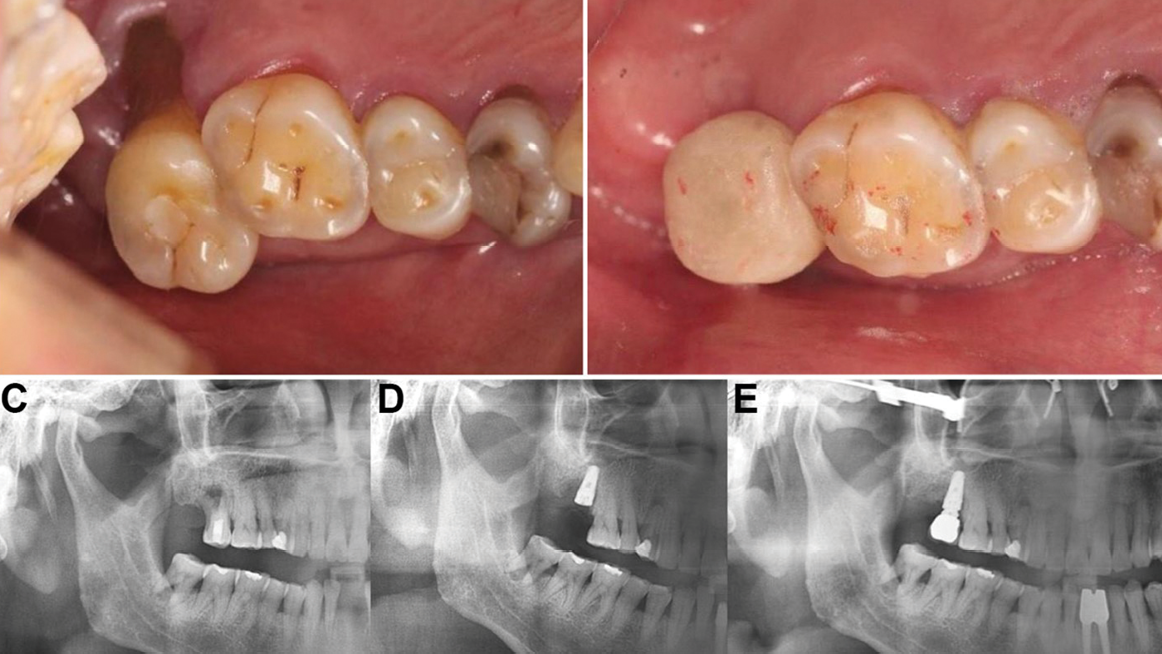
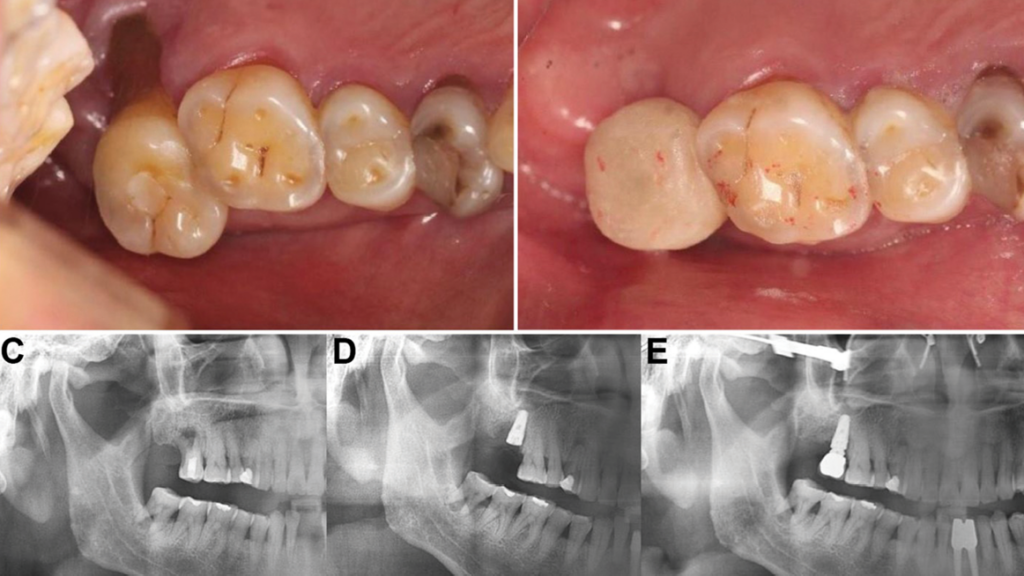
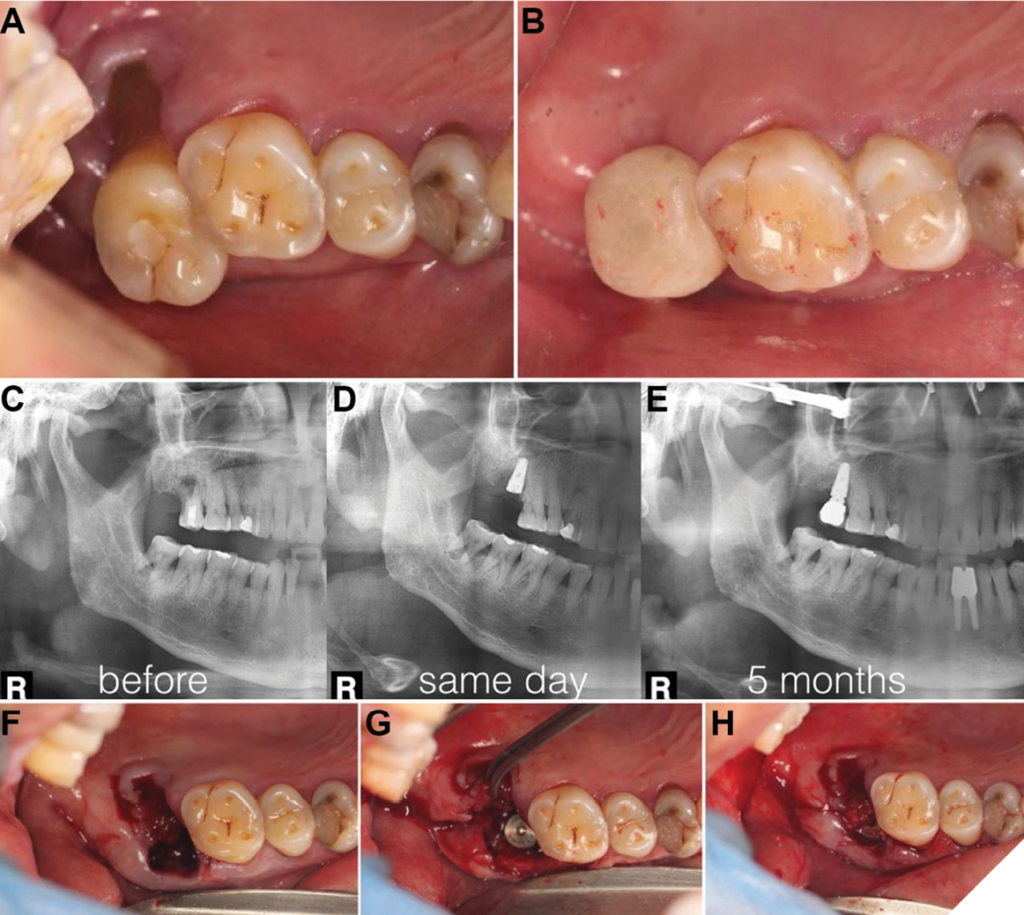
A 58-year-old male patient presented with severe palatal root recession and vertical mobility measuring ≥ 1 mm (i.e., classified as Leon’s Vertical Mobility Class II) at tooth #2 (Fig. 3A). Clinical examination revealed the presence of an abscess and bleeding upon probing, while the patient reported no sensitivity to temperature in relation to tooth #2. To confirm the clinical findings and evaluate the extent of compromised tissue involvement, a preoperative panoramic radiograph was obtained (Fig. 3C).
It was determined that tooth #2 could be atraumatically extracted using forceps without exerting force (Fig. 3F), revealing intact and mature granulomatous gingival tissue beneath the palatal root, which rendered it suitable for the LEGP technique. Utilizing a periosteal elevator, a full thickness flap of the granulomatous tissue, known as the LEGP Flap, was carefully elevated.
The socket was thoroughly debrided, and sounding of the exposed bone surface was performed to ensure complete removal of the granulomatous tissue. Subsequently, anorganic bovine bone grafting material (Bio-Oss®, Geistlich Pharma North America, Inc.) was placed into the socket. A specially designed, dental implant with threaded and cutting features (HexaPlus™, OsseoFuse® International Inc.) was then inserted, utilizing the vertical and horizontal step-locking threads of the implant to achieve reliable primary stability (Fig. 3G).19
Additional bone graft material (e.g., Bio-Oss®, Geistlich Pharma North America, Inc.) was placed in the socket. Subsequently, passive primary closure was achieved using the granulomatous LEGP Flap (Fig. 3H). The implementation of the LEGP technique allowed for implant placement and closure without the need for any buccal gingival releasing incisions, vertical incisions, or artificial membranes. The accuracy of implant positioning was verified through a panoramic radiograph (Fig. 3D).
To ensure unhindered wound healing and effective infection control, the patient was prescribed antibiotics (e.g., Augmentin 500 mg BID) administered twice daily, for a duration of seven days. Following a healing period of five months, the implant was restored with a crown (Fig. 3B). Radiographic examination confirmed complete integration of the implant (Fig. 3E).
Fig. 3A-H
Discussion
It is noteworthy that, in accordance with the provided classification, the feasibility of employing the LEGP technique for Leon’s Vertical Mobility Class I patients is limited due to insufficient soft tissue (i.e., granulomatous tissue partially covering the socket after tooth extraction and bone sounding) and an inability to raise a complete flap for primary closure (Table 1). Moreover, comprehensive clinical and histological studies are imperative to validate the routine application of the LEGP technique in cases where dental implant patients are afflicted by chronic infections, which undoubtedly pose a threat to bone regeneration.
Table 1: Leon’s Vertical Mobility Classification
However, recent research conducted over the past decade investigating immediate implant placement in infected sites has revealed promising outcomes in terms of esthetics, osseo-/soft-tissue integration, and other clinical parameters, thus indicating the potential success of such treatment approaches.20-23 These studies align with the principles of the LEGP protocol, suggesting that meticulous debridement and cleansing procedures of the sockets play a crucial role in achieving favorable and predictable results. Furthermore, recent investigations specifically focusing on the LEGP technique have corroborated a remarkable 99% implant survival rate when utilizing preserved diseased soft tissue for primary closure.24
Conclusion
The introduction of new implant therapy techniques aimed at addressing deficiencies in both bone and soft tissue, such as the Leon’s Everted Gingival Pouch (LEGP) technique, holds significant advantages for both dental practitioners and patients when dealing with challenging periodontal conditions and localized infections. While further clinical studies are warranted to validate the positive outcomes associated with the LEGP technique, it represents a groundbreaking approach that maximizes the utilization of typically discarded granulomatous tissue to achieve efficient and safe primary closure, serving as an alternative to the traditional requirement of multiple surgical interventions for periodontal infection control, soft tissue regeneration, and bone augmentation in implant cases. The cases presented in this article have demonstrated enduring and predictable results with favorable clinical outcomes. Together with previous research findings, these results strongly indicate that the LEGP technique may be a suitable treatment option for patients afflicted with periodontal diseases and in need of implant therapy. 
Oral Health welcomes this original article.
References
- Lioubavina Hack N, Lang NP, Karring T. Significance of primary stability for osseointegration of dental implants. Clinical Oral Implants Research. 2006;17:244-50.
- Baelum V, Ellegaard B. Implant survival in periodontally compromised patients. JPeriodontol. 2004;75:1404-12.
- Mengel R, Flores-De-Jacoby L. Implants in patients treated for generalized aggressive and chronic periodontitis: a 3-year prospective longitudinal study. J Periodontol. 2005;76:534-43.
- Cairo F, Pagliaro U, Nieri M. Treatment of gingival recession with coronally advanced flap procedures: a systematic review. J Clin Periodontol. 2008;35:136-62.
- Chen L, Cha J. A three-point translation technique for root coverage with 4-year follow-up.Dent Today. 2002;21(10):112-115.
- Chen L, Cha J, Guiha R, Bouwsma J. Root coverage with enamel matrix derivatives.Compend Continu Dent Ed. 2002;23(9):797-802.
- Allen EP, Miller Jr PD. Coronal positioning of existing gingiva: short term results in the treatment of shallow marginal tissue recession. J Periodontol. 1989;60:316-9.
- Miller Jr PD. Root coverage with the free gingival graft: factors associated with incomplete coverage. J Periodontol. 1987;58:674-81.
- Bernimoulin JP, Luscher B, Muhlemann H. Coronally repositioned periodontal flap. J Clinical Periodontol. 1975;2:1-13.
- Hammerle CH, Araujo MG, Simion M. Evidence‐based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res. 2012;23:80-2.
- Kassab MM, Badawi H, Dentino AR. Treatment of gingival recession. Dent Clin North Am.2010;54:129-40.
- Murakami S, Takayama S, Ikezawa K, et al. Regeneration of periodontal tissues by basic fibroblast growth factor. J Perio Research. 1999;34:425-30.
- Aukhil I. Biology of wound healing. Periodontol 2000. 2000;22:44-50.
- Sporn M, Roberts AB. Peptide growth factors and inflammation, tissue repair, and cancer. J Clin Investig. 1986;78.2:329
- Martin P. Wound Healing–Aiming for perfect skin regeneration. Science. 1997;276:75-81.
- Chen L. Implant Complication Management. ICOI Winter Symposium Miami. 2005 Jan 13-15.
- Chen L, Zhang X, Huang T-F, Cheng W-S, Chen S-F, Cha J. Gingival revitalization by Inverted Gingival Pouch (IGP) technique. J Implant & Advanced Clin Dent. 2017;9:12-25.
- Shehabeldin et al. Intrasocket reactive tissue: The state of current knowledge. Int J Oral Implantol. 2023:16(2):95-103.
- Chen L, Chen N, Chen A, Chen A, Chen N, Chen N. “A One-Drill System for Predictable Osteotomy and Immediate Implant Placement”. EC Dental Science 22.1 (2023) 114-128.
- Jung RE, Zaugg B, Philipp AO, et al. A prospective, controlled clinical trial evaluating the clinical, radiological, and aesthetic outcome after 5 years of immediately placed implants in sockets exhibiting periapical pathology. Clin Oral Implants Res. 2013 Aug;24(8):839-46.
- Crespi R, Capparè P, Gherlone E. Fresh-socket implants in periapical infected sites in humans. J Periodontol. 2010 Mar;81(3):378-83.
- Marconcini S, Barone A, Gelpi F, Briguglio F, Covani U. Immediate implant placement in infected sites: a case series. J Periodontol. 2013 Feb;84(2):196-202.
- Montoya-Salazar V, Castillo-Oyagüe R, Torres-Sánchez C et al. Outcome of single immediate implants placed in post-extraction infected and non-infected sites, restored with cemented crowns: a 3-year prospective study. J Dent. 2014 Jun;42(6):645-52.
- Liu Y, Chen Y, Chu C et al. A prospective cohort study of immediate implant placement into posterior compromised sockets with or without primary wound closure of reactive soft tissue. Clin Implant Dent Relat Res. 2019 Nov 22. doi: 10.1111/cid.12845.
About the Authors

Aleq Chen is the Executive Assistant at the Dental Implant Institute in Las Vegas and OsseoFuse Onedrill Dental Implant System. He is actively involved in dental conferences and is currently designing algorithmic software for immediate implant procedures.

Nasdaq Chen is the CFO of The Dental Implant Institute in Las Vegas and OsseoFuse Onedrill Dental Implant System. He is actively engaged in developing algorithmic software for immediate implants.

Niq Chen is the CTO of The Dental Implant Institute in Las Vegas and a graduate of Universidad Europea de Madrid. He is currently enrolled in a postdoctoral program in periodontics at Columbia University College of Dental Medicine.

Nina Chen is currently a resident at the New York University College of Dentistry, furthering her education in periodontics and implant dentistry.

Audree Chen is currently a resident in the Prosthodontics Program at Tufts University, where she is also pursuing a joint Master of Science degree.