


An elite athlete presented with multiple areas of incipient interproximal caries. Through ongoing learning of behaviour modification techniques and evidence-based decision-making, incorporating the patient’s goals and preferences, the latest research, and clinician expertise were imperative.
Initially, my participant presented with a high caries risk assessment and an initial Plaque Index of 68%. Reducing his risk for the progression of cavities was very important to him, as he didn’t want expensive dental care. He would be interested in changing his oral self-care practices and discussing options for reducing sugar using small, quick changes.
The Transtheoretical Model was used throughout the project to determine and understand the changing process of the participant’s readiness for change. Motivational Interviewing techniques were also used to facilitate the patient’s oral health behavioural change using a collaborative partnership between patient and clinician.
The prevention of the progression of incipient dental caries required a multifaceted approach to include diet, oral hygiene, and individual risk factors to address both individual and social factors.
Exploring the social behaviour of consuming sugar-containing gum and sports drinks, and identifying alternatives worked towards developing more sustainable strategies.
Interventions focused on improving oral hygiene habits considered the broader social context influencing the adoption and sustainability of behaviours. Habit stacking provided a framework for my patient to implement complementary habits, ensuring that his oral health regimen is consistently executed.
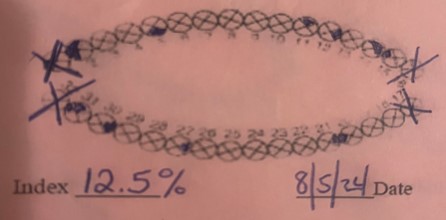
A post Plaque Index indicated a biofilm reduction of 24% and the presence of acid producing biofilms at 12.5%. This tool assisted my patient in the process of preventing caries and managing his oral health.
The use of motivational interviewing strategies throughout the process emphasized the importance of understanding one’s perspective to strengthen motivation, provide support, and create innovative techniques for sustained behavioural change.
Introduction
An 18-year-old male Division I hockey player presented with multiple areas of incipient interproximal caries after his first semester in college. In truth, my approach would have been to show the radiographs, discuss the progression of disease, and offer potential solutions. However, through ongoing learning of behaviour modification techniques and evidence-based decision-making, it is crucial to incorporate the patient’s goals and preferences, the latest research, as well as the clinician’s expertise, for long-term behaviour change. This opportunity to integrate behavioural change strategies, caries management, and social support, allows the experiential learning necessary to support all patients’ health outcomes.
This multifactorial disease process requires a multifaceted approach to change behaviours and outcomes. My order of approach also needed to change to understand how important maintaining his oral health was to the patient and assist with prioritizing his goals. This requires active listening, reflective practice, and the establishment of trust.
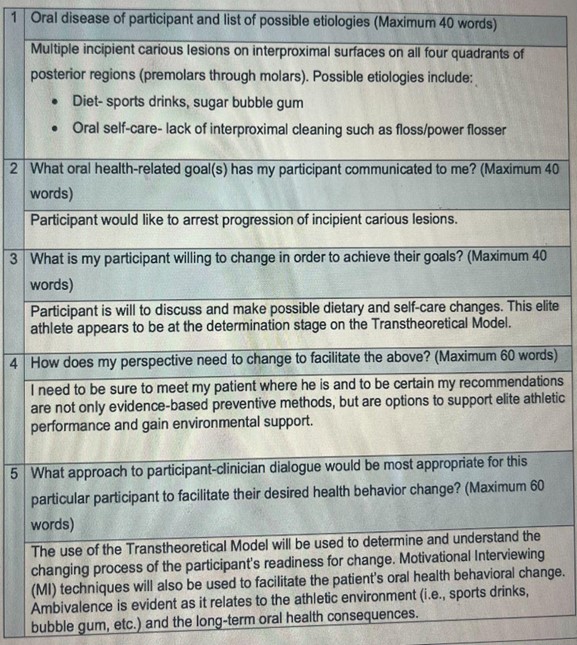
The use of the Transtheoretical Model will be used throughout the project to determine and understand the changing process of the participant’s readiness for change. Motivational Interviewing techniques will also be used to facilitate the patient’s oral health behavioural change. Additionally, addressing ambivalence is important as it relates to the athletic environment and the participant’s willingness to change.
The participant would like to arrest the progression of “early cavities” between his teeth and discuss health options to make possible dietary and self-care changes. This elite athlete appears to be at the determination stage on the Transtheoretical Model.
Meeting the patient where he is at and providing recommendations that are not only evidence-based preventive methods but also options to support elite athletic performance and environment is crucial.
With the use of the latest research, motivational techniques, and behaviour change models, it is the hope to create a plan that promotes long-term oral health and meets the unique needs of this elite athlete.
Behaviour change question:
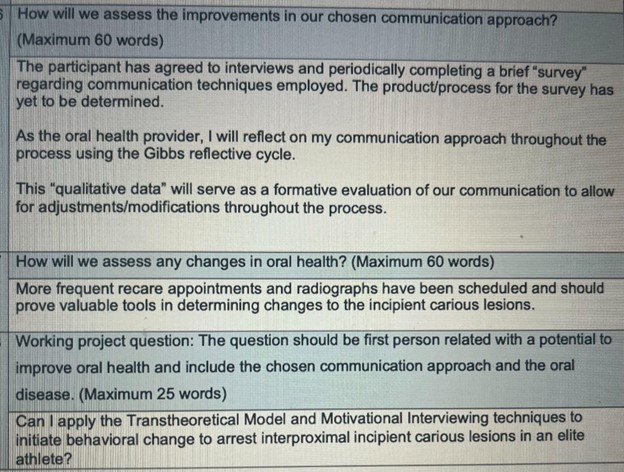
“If I apply the Transtheoretical Model and Motivational Interviewing techniques to institute behavioural change, how will this support the arrest of interproximal incipient carious lesions in an elite athlete?”
Current knowledge
Oral health is a critical component of overall health, particularly for individuals engaged in high-intensity physical activities. The prevention of the progression of incipient dental caries in a healthy, elite eighteen-year-old athlete requires a multifaceted approach that addresses both individual and social factors. Personalized, evidence-based prevention strategies and assessments aimed at reducing caries and improving oral health outcomes are crucial.1
The implementation of behavioural change techniques are essential in promoting healthy nutritional choices and improving oral self-care practices. Research has highlighted the potential of behavioural change models and motivational techniques to guide sustainable improvements.2 Interventions that target self-efficacy, such as those described by Bantel et al., (2023) can empower athletes to take an active role in their oral hygiene routines and make sustainable changes to their behaviours. Providing a comprehensive framework that combines the Transtheoretical Theory and motivational interviewing techniques may support the athlete’s journey towards improved oral health.
One systematic review examined the effectiveness of models for individual oral health promotion, noting the need to develop an effective chairside approach that addresses the underlying social determinants of oral disease.3 The review emphasized the potential of motivational interviewing to empower individuals in managing their oral health, moving beyond the traditional biomedical model that focused solely on knowledge and skills acquisition.3
Motivational interviewing recognizes that behaviour change requires a collaborative partnership between the patient and the clinician, where the patient’s expertise on their own circumstances is acknowledged and they are actively engaged in a non-judgmental dialogue to explore their own reasons for change. Thus assisting with identifying their personal values and goals.
Ambivalence can be a significant obstacle in implementing effective behavioural change techniques. To overcome this ambivalence, a comprehensive approach is required to address both the individual’s beliefs and the environmental factors that contribute to their behaviour. Health professionals can work with athletes to help them recognize and resolve their ambivalence, providing them with the necessary knowledge, skills, and support to make sustainable changes to their dietary habits and oral hygiene practices. Additionally, collaborating together in teaching proper oral hygiene techniques, including efficient brushing and flossing, can help to successfully prevent the development and progression of dental caries.1
The progression of incipient dental caries is a complex process influenced by various factors, including diet, oral hygiene, and individual risk factors. Preventive measures are crucial in limiting the risk of incipient dental caries and promoting overall oral health in elite athletes. A comprehensive, personalized approach to prevention is essential, incorporating both professionally applied and home-care interventions.1 Professionally applied preventive measures may include the application of fluoride varnishes and other remineralizing agents to strengthen tooth enamel and inhibit the progression of early caries lesions. Interventions focused on improving oral hygiene habits should consider the broader social context and socioeconomic factors that may influence the adoption and sustainability of these behaviours.4
Oral self-care measures, such as diligent oral hygiene practices, can also significantly contribute to the maintenance of healthy teeth. The current literature suggests that power flossers may play a crucial role in maintaining and improving the oral health of young individuals. Specifically, evidence indicates that the use of power flossers can significantly reduce plaque accumulation and the incidence of caries, particularly in hard-to-reach areas of the mouth.4 Moreover, the convenience and ease of use associated with power flossers make them an attractive option for individuals who may struggle with traditional manual flossing techniques.5 Ultimately, the use of power flossers to arrest the progression of incipient caries should be considered as part of the personalized preventive strategies tailored to the unique needs of the individual.1
Social factors also play a significant role in oral health needs and outcomes. Exploring the social behaviour of chewing sugar-containing gum and identifying potential alternatives can work towards developing more effective and sustainable strategies for maintaining oral health. The role of social support cannot be underestimated in the context of oral health for elite young athletes. Gomes et al., (2019) have highlighted the significant impact of social support and health beliefs on the overall well-being of adolescents. By fostering a supportive environment that encourages healthy habits and provides access to dental care, coaches, parents, and healthcare professionals can contribute to the long-term oral health of athletes.
Dietary modifications, such as reducing the consumption of sugary and acidic foods and beverages, can further support the prevention of incipient dental caries.6 Since chewing bubble gum is a common social occurrence, an alternative to sugar containing bubble gum is important. One promising approach to preventing the progression of incipient caries is the use of xylitol chewing gum. Xylitol has been shown to have antimicrobial properties and the ability to disrupt the formation of dental biofilms.7 Chewing gum containing xylitol can help increase saliva flow, which in turn enhances the natural cleansing and remineralization processes in the oral cavity. Additionally, the physical act of chewing gum can have a beneficial mechanical effect on biofilm removal and overall oral hygiene.7
While the evidence for the oral health benefits of chewing gum additives can be challenging, it is a promising strategy for preventing the progression of incipient caries.8 Regular chewing of xylitol-containing gum can help maintain good oral health and support the overall performance and well-being of athletes.
Additionally, the selection of appropriate beverages for athletes is a crucial consideration, balancing the need for effective rehydration, energy replenishment, the preservation of overall health, and acceptable taste. One area of particular concern is the high sucrose content found in many sports drinks. Recent research has highlighted the detrimental effects of sugar-based sports drinks on oral health, with studies reporting a high prevalence of dental caries and erosion associated with their increased consumption, especially among adolescents and athletes.9
This health promotion project will be conducted in the dental practice setting, as well as through phone interviews. During these sessions, I will utilize motivational interviewing techniques to assess the athlete’s current stage of readiness for change, explore their barriers and facilitators to maintaining good oral hygiene, and collaboratively develop a personalized plan to address the progression of incipient carious lesions.
Behaviour change techniques/models which were implemented and tested
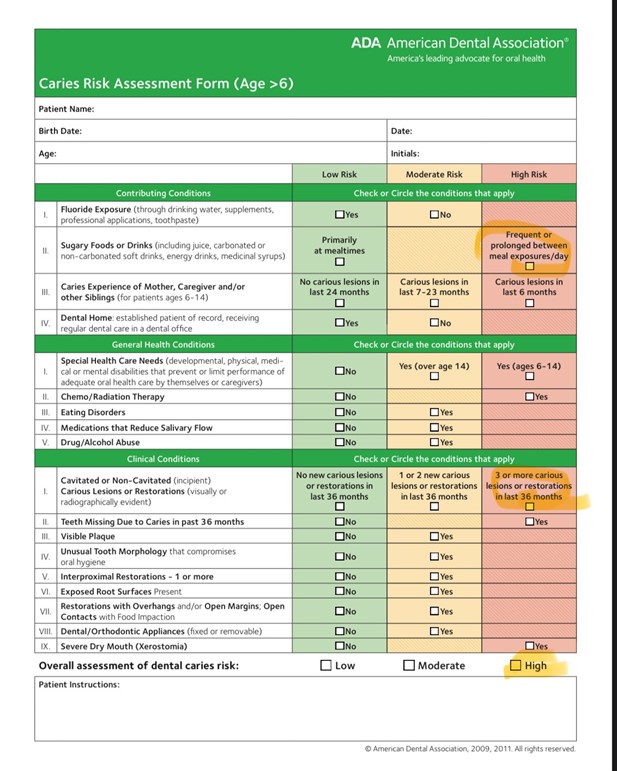
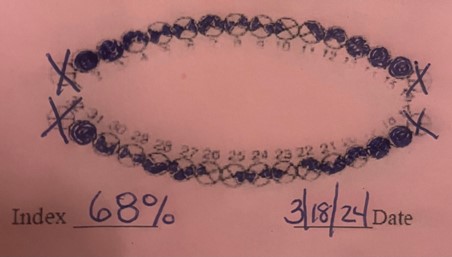
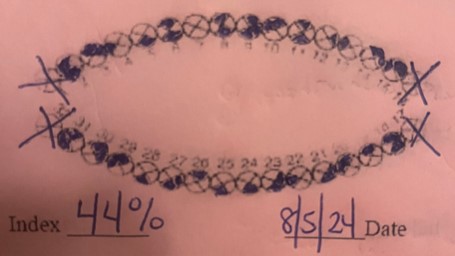
My participant presented at our initial visit for radiographs and prophylaxis. This eighteen-year-old has a negative medical history with no known allergies and is taking no medications. His caries risk assessment (Appendix 4) was high and his initial Plaque Index was 68% (Appendix 5).
With his permission, I asked him questions about possible health behaviour change (Appendix 3). He stated that reducing his risk for the progression of cavities was very important to him, as he doesn’t want expensive dental care. He indicated that he would be interested in changing his oral self-care practices and discussing options for reducing sugar. He would be interested in small, quick changes that would not change his life socially. He would like to find easier ways of doing things that would not be time-consuming or expensive. This elite athlete appears to be at the determination stage on the Transtheoretical Model.
He would like to be given some different, healthier options for bubblegum, but does not want to give it up. He will also discuss drinking options, although he plans to drink sports drinks if offered by his coach.
He would like to make changes that don’t require him to think about constantly or make major lifestyle adjustments. For example, since he is already showering, he said he may as well use the power flosser in the shower. He already has a power flosser, but rarely uses it at the bathroom sink.
He likes the idea of working together to find/sample drink and bubblegum choices. He is also open to sharing resources such as a video or app, but does not want me to check-up on him. He definitely doesn’t want me to ask questions like, “did you floss today?” He likes the idea of working together and having control of his options without judgment.
At a subsequent visit, we discussed adding fluoride gel to his oral health routine. He was initially hesitant, but upon further discussion, I learned that he doesn’t like the feel of fluoride varnish. I explained the properties and options for a prescription gel to replace his toothpaste; he was extremely aggreable as it has an acceptable taste and texture.
He has replaced his bubblegum with one of the xylitol options given. He likes the flavor and stretchiness and has introduced the gum to a couple of his teammates.
He has replaced sports drinks with water during practice and has a banana afterwards for muscle recovery and athletic performance. He continues to drink sports drinks after a game, but is trying to be more mindful of drinking it quickly.
Using the power flosser in the shower is becoming more consistent. He states that he does it eight out of ten times. He misses occasionally because he is running late, but is trying to give himself an extra couple of minutes to not be rushed. This elite athlete appears to now be at the action stage on the Transtheoretical Model.
Another plaque index was completed twelve weeks after the initial appointment. There was a biofilm reduction of 24% (Appendix 6) with the greatest decrease of plaque on the interproximal surfaces. With the initial plaque index, I used a two-tone disclosing solution as a visual method to discuss with the patient areas of concern and the difference between older and newer biofilm present. The post-index involved the use of a three-tone disclosing solution to also identify pathological, acid-producing biofilms. The presence of acid-producing biofilms was 12.5% (Appendix 7). This visual tool assisted my patient with not only an awareness of his current oral self-care status, but also actively engaged him in the process of preventing caries and managing his oral health effectively.
Overall, my patient is feeling very positive and proud of his new routine. He appreciates his sense of control, that we focus on what’s going well, and that he never feels judged.
New knowledge
The use of motivational interviewing strategies throughout the process emphasized the importance of understanding the athlete’s perspective and involved using active listening, open-ended questions, and reflective responses to strengthen his motivation for change. This approach not only respected the athlete’s autonomy but also built rapport, making him more engaged in the change process; ultimately leading to more effective and personalized strategies for overcoming barriers to change. Fostering a sense of partnership between us with a non-judgmental awareness of his thoughts and feelings was essential for addressing underlying ambivalence to modify behaviour.
Sending short videos of elite athletes displaying healthy behaviours was helpful. This use of the social cognitive theory to promote self-efficacy appeared to impact his motivation, goal-setting, and persistence. Vicarious experiences, such as observing an Olympian eat a banana for muscle recovery, served as a powerful source of self-efficacy information.
Habit stacking provided a structured framework for my patient to implement a series of complementary habits, ensuring that his oral health regimen is consistently executed without overwhelming his already demanding schedule. For example, using the power flosser in the shower. By leveraging habit stacking, my patient was able to streamline his oral health practices to enhance his overall performance and well-being.
With the initial plaque index, I used a two-tone disclosing solution as a visual method to discuss with the patient areas of concern and the difference between older and newer biofilm present. The post-index involved the use of a three-tone disclosing solution to also identify pathological, acid producing biofilms. This visual tool assisted my patient with not only an awareness of his current oral self-care status, but also actively engaged him in the process of preventing caries and managing his oral health effectively.
Discussion
The results of my health behaviour change action research were very positive. The incorporation of motivational interviewing techniques served to create a more supportive environment that acknowledges the complexity of experiences and emotions surrounding behavioural change, which is critical for sustaining long-term commitment to healthy lifestyle behaviours. By prioritizing a collaborative approach that emphasizes empathy and understanding, I can effectively navigate the competing motivations patients may face, ultimately enhancing their readiness to succeed in adopting desired behaviour changes that align with their personal goals. By providing a variety of choices, I expanded my patient’s options allowing for a greater sense of control and autonomy.
By employing a mindful approach (i.e., reflective listening, empathy, compassion, patience) alongside motivational interviewing, I can help patients recognize and accept their emotional responses to challenges, which is essential for confronting ambivalence without pressure and fostering personal growth.
Moreover, this combination of motivational interviewing and mindfulness creates a supportive environment to encourage patients to openly explore their feelings and apprehensions, to ultimately facilitate more effective intervention strategies designed for their unique circumstances and challenges. By creating an atmosphere of trust and collaboration, I can significantly enhance a patient’s willingness to engage in behavioural change.
It is essential to meet a patient where they are at, not where I want them to be. Sending a motivational video sometimes elicited a “cool” and I needed to recognize that this may help to reinforce change as a short-term motivational strategy and not necessarily elicit change. This project has also underscored the importance to celebrate incremental achievements and to anticipate relapses as an opportunity to learn and grow. Social support plays a crucial role in the success of any preventive strategy. Involving family, coaches, and teammates in the implementation and reinforcement strategies can enhance an individual’s adherence and increase the likelihood of long-term success.
The application of disclosing solutions can significantly aid in visualizing plaque accumulation, allowing for a quantitative pre-procedure plaque index and post-plaque index assessment following the implementation of oral hygiene interventions. The plaque index employed was a dichotomous survey to determine the presence or absence of plaque. The distinctive colors provided by the two-tone and three-tone disclosing solutions serve as a guide for patients to understand the areas of new plaque accumulation and areas consistently missed. This visual assessment allows for improved engagement in oral self-care and the potential for improved oral health outcomes.
This project has reinforced for me the need to incorporate the best scientific evidence, my own clinical expertise, and my patients values, beliefs, and expectations. The need for a collaborative approach to guide a personalized preventive care plan is essential for sustainable change. Providing a variety of choices expanded my patient’s options allowing for more control and autonomy. Learning the implementation of ‘making every contact count’ allowed me to assist my patient in his behaviour change efforts and support his general well-being.
Providing ongoing support and innovative motivational techniques are essential for sustained behavioural change guiding patients from action to maintenance. It is imperative to meet patients where they are within the stages of change to encourage self-efficacy and optimize performance.
Appendices
Appendix 1: Health Behavior Change Proposal
Appendix 2: Health Promotion Project Consent Form
Dear Ben,
This year, I am studying with O’Hehir University to earn a Bachelor of Science degree in Oral Health Promotion. An important part of my studies is completing a project which will help my patients to improve their oral health through a new approach, called health behavioral change. I would be most appreciative if you would choose to participate.
My data collection methods will include oral hygiene indices and questionnaires (verbal and written). I guarantee confidentiality of information and promise that no names will be made public. Participation is simple and easy.
If you choose not to participate you are free to do so with no consequences. If you choose to participate, and wish to be kept informed about the progress of the project, I can keep you informed via email or telephone. If you consent, please sign your permission below at your earliest convenience.
I, ____________________________________________consent to participate in the project described above. I understand that at any time I may withdraw my consent.
Signature:_____________________________________ Date: ______________
Please include your contact information if you want to be updated during the project.
Thank you in advance for your consideration.
Maureen Strauss
Appendix 3: Health Behavior Change Questions
1. On a scale of 1 - 10 (10 being the highest), how important is it to you, to reduce your risk for the progression of cavities? Why?
2. How do you feel about changing your oral health care practices and reducing sugar intake?
3. If you decided to change, what might your options be?
4. What potential challenges or barriers do you anticipate as you change this behavior, and how might you overcome these challenges?
5. How can I help you succeed?
Appendix 4: Caries Risk Assessment (CAMBRA)
Appendix 5: Pre-assessment
Appendix 6: Post-assessment
Appendix 7: Post-assessment for acid producing biofilms
References
- Lakhani, S. R., Noble, F., Rodd, H., & Cobourne, M. T. (2023). Management of children with poor prognosis first permanent molars: an interdisciplinary approach is the key. British Dental Journal, 234(10), 731–736. https://doi.org/10.1038/s41415-023-5816-7
- Ramseier, C., & Suvan, J. E. (2011). Health Behaviour Change in the Dental Practice. John Wiley & Sons.
- Yevlahova, D., & Satur, J. (2009). Models for individual oral health promotion and their effectiveness: A systematic review. Australian Dental Journal, 54(3), 190–197. https://doi.org/10.1111/j.1834-7819.2009.01118.x
- Martin, M., Pugach, O., Avenetti, D., Lee, H., Salazar, S., Rosales, G., & Songthangtham, N. (2020). Oral Health Behaviours in Very Young Children in Low-Income Urban Areas in Chicago, Illinois, 2018–2019. Preventing Chronic Disease, 17(200213). https://doi.org/10.5888/pcd17.200213
- Vernon, L. T., Paes, A., & Seacat, J. D. (2017). In defense of flossing: Part II-can we agree it’s premature to claim flossing is ineffective to help prevent periodontal diseases? The Journal of Evidence-Based Dental Practice, 17(3), 149–158. https://doi.org/10.1016/j.jebdp.2017.06.003
- Segura, A., Boulter, S., Clark, M., Gereige, R., Krol, D., Mouradian, W., Quinonez, R., Ramoz-Gomez, F., Slayton, R., & Keels, M. A. (2014). Maintaining and improving the oral health of young children. Pediatrics, 134(6), 1224–1229. https://doi.org/10.1542/peds.2014-2984
- Hayashi, Y., Ohara, N., Ganno, T., Ishizaki, H., & Yanagiguchi, K. (2007). Chitosan-containing gum chewing accelerates antibacterial effect with an increase in salivary secretion. Journal of Dentistry, 35(11), 871–874. https://doi.org/10.1016/j.jdent.2007.08.004
- Maslii, Y., Garmanchuk, L., Ruban, O., Dovbynchuk T., Herbina, N., Kasparaviciene, G., & Bernatoniene, G. (2023). The Study of the Cytotoxicity, Proliferative and Microbiological Activity of the Medicated Chewing Gum with Ascorbic Acid and Lysozyme Hydrochloride Using Different Culture of Cells. Pharmaceutics, 15(7), 1894–1894. https://doi.org/10.3390/pharmaceutics150718
- Khan, K., Qadir, A., Trakman, G., Aziz, T., Khattak, M. I., Nabi, G., Alharbi, M., Alshammari, A., & Shahzad, M. (2022). Sports and Energy Drink Consumption, Oral Health Problems and Performance Impact among Elite Athletes. Nutrients, 14(23), 5089. https://doi.org/10.3390/nu14235089
- Bantel, D., Chmielewski, W. X., Elmar Brähler, Yve Stöbel-Richter, Zenger, M., & Berth, H. (2023). Variables associated with oral health-related self-efficacy – results of a cross-sectional study. BMC Oral Health, 23(1). https://doi.org/10.1186/s12903-023-03656-x
- Gomes, A. C., Rebelo, M. A. B., de Queiroz, A. C., de Queiroz Herkrath, A. P. C., Herkrath, F. J., Rebelo Vieira, J. M., Pereira, J. V., & Vettore, M. V. (2019). Socioeconomic status, social support, oral health beliefs, psychosocial factors, health behaviours and health-related quality of life in adolescents. Quality of Life Research, 29(1), 141–151. https://doi.org/10.1007/s11136-019-02279-6
About the author

Maureen Strauss has served as a professor at Middlesex Community College since 2005 and brings decades of clinical experience as a practicing dental hygienist. She earned her Bachelor’s degree from O’Hehir University and a Master’s degree from Boston University. Maureen provides educational leadership in Community Health, Clinical Dental Hygiene Practice, and Pain Management, and actively contributes to academic curriculum development. A former president of the Massachusetts Dental Hygienists’ Association (ADHA), she has been recognized with multiple awards for excellence in teaching and clinical practice.