


Impaction of second molars, whether maxillary or mandibular, is an uncommon but clinically significant anomaly in orthodontics, with a reported prevalence ranging from 0.03% to 2.3%, depending on the population studied.1 Unlike third molars, which are frequently impacted and often extracted prophylactically, impacted second molars are traditionally preserved to establish and maintain functional occlusion. Etiology of their impaction is not well understood, although common possibilities to explain these conditions have been ectopic position, obstacles in their eruption path, posterior dental crowding, and failures of eruption mechanism.2 Their impaction can lead to significant clinical challenges, including malocclusion, periodontal compromise, and the need for complex orthodontic or surgical interventions. Magnusson and Kjellberg emphasized the importance of early detection and individualized treatment planning, noting that delayed diagnosis often results in more invasive procedures and less favorable outcomes.3
While impaction of second molars is a relatively uncommon orthodontic issue, encountering cases with vertical growth patterns is not unusual. Non-surgical orthodontic management of hyperdivergent patients requires a careful, biomechanically sensitive approach to ensure adequate control in prevention of secondary effects. These patients often exhibit a clockwise mandibular rotation and open bite tendency, making vertical control a primary treatment objective.4 Different strategies exist to control the vertical dimension. Bonding of the molars, specifically the second molars, is often deliberately avoided in the early stages of treatment, or completely, to prevent further eruption and vertical development of the posterior dentition, which could exacerbate the hyperdivergent pattern. Instead, selective bonding or delayed molar engagement is used to reduce increase in lower facial height.5
This case report will focus on a non-surgical management of impacted second molars with a hyperdivergent growth pattern and open bite tendency, demonstrating the intricacies of vertical control while aligning the second molars into occlusion.
Diagnosis
A 13-year-old and 8-month-old girl presented with the chief complaint of “having a tooth stuck in [their] gums”, pointing at the region of tooth 1.3. Her medical history is non-contributory. Extra-oral examination shows a convex profile, orthognathic maxilla, and retrognathic but large mandible, rotated down and back, contributing to an increased anterior lower face height. The frontal view shows a maxillary midline deviated 2 mm to the right from the facial midline. Intra-oral examination shows a molar Class I malocclusion associated with unerupted teeth 1.3, 1.7, 2.7, 3.7 and 4.7, decreased overbite, decreased overjet, and an overall Bolton discrepancy with mandibular excess. The patient reported a history of nail-biting habit and of non-nutritive thumb sucking.
Fig. 1A

Fig. 1B

The patient’s panoramic radiograph shows distal crown angulation of 3.7 and 4.7. Developing third molars are shown with hyperplastic follicles. The mandibular third molars which have a mesial crown angulation are suspected to be obstacles in the eruption of path of 3.7 and 4.7. Tooth 1.3 appears crowded rather than impacted. The patient’s lateral cephalometric radiograph shows a development stage of CS4, which would indicate that peak mandibular growth has occurred less than a year since this stage.6 Further cephalometric measurements are listed in Table 1.
Fig. 2
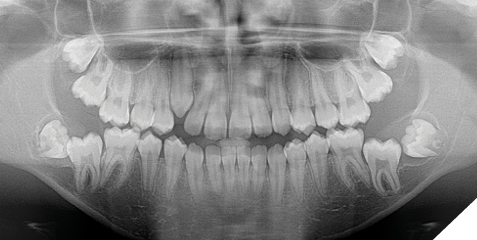
Fig. 3
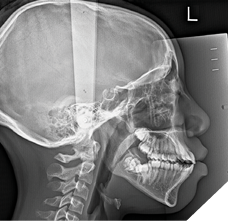
Table 1: Pre-treatment cephalometric measurements
| Measurement | Patient value | Norm | Unit |
| SNA | 79.9 | 82.0±3.5 | ° |
| SNB | 75.7 | 80.9±3.4 | ° |
| ANB | 4.1 | 1.6±1.5 | ° |
| Unit Length Difference (Co-Gn – Co-A) | 33.8 | 23.7±4.0 | mm |
| SN – GoGn | 43.6 | 32.9±5.2 | ° |
| FMA (MP – FH) | 29.3 | 24.3±4.5 | ° |
| U1 – PP | 124.6 | 110.0±5.0 | ° |
| L1 – MP | 95.8 | 95.0±5.0 | ° |
| Interincisal angle | 107.4 | 130±6.0 | ° |
Treatment objectives and plan
The treatment objectives were to make space for teeth 1.3, 1.7, 2.7, 3.7 and 4.7 and establish ideal overbite and overjet with a non-surgical approach. The initial plan consisted of having all third molars extracted, followed by insertion of full maxillary and mandibular fixed appliances. Re-assessment of bicuspid extractions was planned following space creation for 1.3 which was planned to be done with open coil springs on a continuous archwire. Extraction of bicuspids were anticipated for closing the overbite which was suspected to decrease with space creation for 1.3. However, they were not done simultaneously with the extraction of third molars since model analysis showed no lack of space across the entire arch due to the spacing and rotations of other teeth, rendering the extraction decision less certain.
Treatment progress
Five weeks following extraction of third molars, full maxillary and mandibular bonding with Twin Brackets (0.022” slot, MBT prescription) was undertaken at the initial visits with early insertion of an open coil spring between teeth 1.2 and 1.4 to create space for 1.3, and help in shifting the maxillary midline to the left. The wire sequence for both arches was as follows: 0.014” NiTi, 0.018” NiTi. An 0.018” SS was subsequently placed in the maxillary arch only to facilitate space opening for 1.3. At the end of this initial wire sequence, and following sufficient space creation for 1.3, a decision was made to extract all second bicuspids to help in vertical control and sagittal correction since the patient had significant dental protrusion, limited overbite and limited overjet at this stage. Extraction of second bicuspids was performed 3 months after the decision was made, and orthodontic adjustments resumed 2 weeks following these extractions.
Fig. 4

After the extractions, the wire sequence for both arches was as follows: 0.016”x0.022” NiTi, 0.016”x0.022” SS. Space closure started segmentally at the extraction sites, from the first bicuspid to the first molar with elastomeric chains, on a continuous wire. Tooth 1.3 spontaneously erupted into the maxillary arch 12 months into treatment. Tooth 1.3 was eventually engaged into a continuous maxillary archwire, stepping back down to a 0.014” NiTi. At this stage, all second molars had simultaneously erupted into their respective arches. However, the eruption of the second molars showed that the maxillary second molars were in lingual crossbite to the second mandibular molars.
Fig. 5

Space closure continued with conventional sliding mechanics, and at times, was aided with gable bends to counter crown tipping. Bracket repositions were done at 19 months, stepping down to a 0.018” NiTi wire in both arches. Second molars were bonded at this point but not yet engaged to the archwires. The patient was also instructed to wear intermaxillary elastics for vertical control, going bilaterally from U3-L3-L4s with 3/16”, 4.5 oz rubber bands. At 22 months, the patient had progressed to 0.016”x0.022” SS wires to resume space closure and 0.016” NiTi wires were overlayed on top and were engaged to the second molars bilaterally.
Fig. 6

The overlay wires progressed to 0.018” SS wires at which point tip back bends in the first order were placed in the mandibular overlay archwire, immediately distal to the first mandibular buspids as seen in Figure 7. This was done in order to create arch constriction at the level of the second mandibular molars.7 These activations were left for 2 months until it corrected the lingual crossbite of all second molars. Continuous archwires in both arches to the second molars were inserted following this correction. In addition to the same intermaxillary elastic pattern previously prescribed, a pattern going from the U6-U7-L7-L6 bilaterally was added to bring the second molars into occlusal contact. Detailing and finishing followed to complete the case’s objectives.
Fig. 7
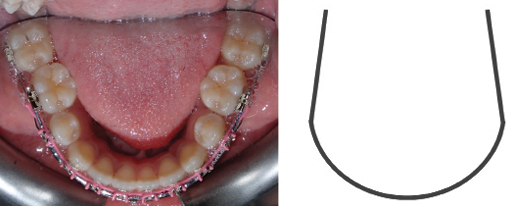
Fig. 8

Treatment results
Several treatment objectives were met successfully, and treatment time lasted a total of 29 months in an academic graduate orthodontic clinical setting. This included a few months of wait time for extractions and decreased appointment availabilities. Teeth 1.3, 1.7. 2.7, 3.7 and 4.7 came into proper occlusal positions. A positive overjet of 2mm was achieved, and an overbite of 5% was achieved, although an overbite of 20% would have been more ideal. The patient’s profile shows mild lip retraction and a reduction in facial convexity which may be attributed to residual mandibular growth. Both maxillary and mandibular dental midlines finished coincident with the facial midline. The post-treatment lateral cephalometric radiograph shows significant reduction in incisor proclination as well as a mild increase in lower anterior face height. For retention, the patient was given full coverage Essix retainers for both maxillary and mandibular teeth, in addition to bonded maxillary 2-2 and mandibular 3-3 fixed retainers. Use of full coverage would be to create a posterior bite block effect to maintain the open bite closure achieved for the patient.
Fig. 9A

Fig. 9B

Fig. 10
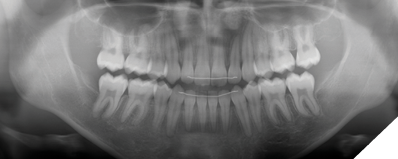
Fig. 11

Discussion
Management of open bite tendencies and impacted second molars can be done in a multitude of ways. In this present case, goals were achieved in a timely manner, considering the several factors that may extend treatment time in a university setting. In hindsight, efficiency of treatment may have been improved with extractions of the second bicuspids done at the same time as the third molars. The initial conservative approach to wait did not have significant benefits, considering the different factors that would point towards the need for bicuspid extractions: open bite tendency, posterior crowding, and decreased interincisal angle.
There were several challenges with this case. The second molars erupting in lingual crossbite posed a problem as its correction with fixed appliances may inadvertently lead to the extrusion of the posterior teeth, working against the vertical correction. Had the second molars erupted in conventional transverse position, consideration of not bonding the second molars would be contemplated as they may erupt naturally into occlusion. The case highlighted the fine line of correcting the lingual crossbite and re-directing eruption forces of the second molars towards occlusal contact without excessive extrusion leading to worsening of the open bite tendency. To correct the lingual crossbite of the second molars, the safest approach to reduce secondary effects was to use of a stiffer base archwire to preserve control over the remaining dentition and using it as an anchor to create a more determinate force system to constrict the second mandibular molars lingually.
In managing the open bite tendency, several methods are usually suggested as they are shown to be predictable, including posterior intrusion mechanics with TADs8 and clear aligner therapy.9 However, many methods of managing an open bite use posterior intrusion which can lead to mandibular counterclockwise rotation.10 In this present case, this is undesirable due to the increased unit length difference and underlying skeletal Class III tendency. The objective became to increase the overbite by anterior extrusion and reduction in incisor proclination to yield relative incisor extrusion.
Conclusion
Management of impacted second molars may pose a challenge when vertical control is also of great importance. Focus should be placed on using predictable treatment planning and careful biomechanics to prevent undesirable secondary effects. The present case shows a clinical example of ensuring minimal side effects following conservative treatment decisions. 
Oral Health welcomes this original article.
References
- Bondemark L, Tsiopa J. Prevalence of ectopic eruption, impaction, retention and agenesis of the permanent second molar. Angle Orthod. 2007;77(5):773-778.
- Raghoebar GM, Boering G, Vissink A, Stegenga B. Eruption disturbances of permanent molars: a review. J Oral Pathol Med. 1991;20(4):159-166.
- Kusnoto B, Schneider BJ. Control of the vertical dimension. Semin Orthod. 2000;6(1):33–42.
- Magnusson C, Kjellberg H. Impaction and retention of second molars: diagnosis, treatment and outcome. A retrospective follow-up study. Angle Orthod. 2009;79(3):422-427.
- Hering K, Ruf S, Pancherz H. Orthodontic treatment of openbite and deepbite high-angle malocclusions. Angle Orthod. 1999;69(5):470-477.
- Baccetti T, Franchi L, McNamara JA. The Cervical Vertebral Maturation (CVM) Method for the Assessment of Optimal Treatment Timing in Dentofacial Orthopedics. Semin Orthod. 2005;11(3):119–29.
- Rebellato J. Two-couple orthodontic appliance systems: activations in the transverse dimension. Semin Orthod. 1995;1(1):37-43.
- Scheffler NR, Proffit WR, Phillips C. Outcomes and stability in patients with anterior open bite and long anterior face height treated with temporary anchorage devices and a maxillary intrusion splint. Am J Orthod Dentofacial Orthop. 2014;146(5):594-602.
- Harris K, Ojima K, Dan C, et al. Evaluation of open bite closure using clear aligners: a retrospective study. Prog Orthod. 2020;21(1):23.
- Deguchi T, Kurosaka H, Oikawa H, et al. Comparison of orthodontic treatment outcomes in adults with skeletal open bite between conventional edgewise treatment and implant-anchored orthodontics. Am J Orthod Dentofacial Orthop. 2011;139(4 Suppl):S60-S68.
About the author

Dr. Thien Vuong earned his dental degree from McGill University and completed a general practice residency at the Montreal Children’s Hospital. He recently completed his M.Sc. and specialty training in orthodontics and dentofacial orthopedics at the University of Toronto. Following the completion of his program, he started practicing in Montreal.