
This is “The most elegant way to correct class II cases” and treat an impacted canine simultaneously.
I have personally met Dr. Luis Carriere and his father, Pepe (PHD in Orthodontics), at their Barcelona’s Clinic in September of 2016 to learn more about his unique approach and thinking of implementing invisalign at the same time with the brand new Clear Carriere Motion II. I love to “do everything first”, since I have been using invisalign simultaneously with other orthopeadic appliances like Herbst, Mara, Haas Palatal Expander, Pendulum Expander. I started doing hybrid systems to be more efficient, to save treatment time, but mainly to address the chief complaint of the patient, which is always the front teeth, not the class II or the width of their maxilla in the back.
We are trained to propose and treat the back of the mouth like class II, class III or transverse problems when the patient is coming for the front of the mouth and teeth that they see first. Because the techniques we used to propose were always like that, treat transverse, sagittal and then finally aligning teeth with braces.
Now we have treatment options that are much more efficient and very aesthetic-driven like clear aligners. When I am using invisalign, I have discovered that there are no longer 3 orders of movement like in fixed braces. There are no such things as leveling, uprighting and torquing teeth in a sequence with a specific evolution of wires at specific intervals. We can now program and design all orders of movement from day 1 with the software of aligner systems. Class II cases, even unilateral ones, can be addressed while we also treat alignment and, why not, an impacted tooth. In 2008, I also started making upper anterior attachments on the lingual side.
This female teenager was 15.5 years old when she consulted me. She was referred firstly for a lower impacted canine.
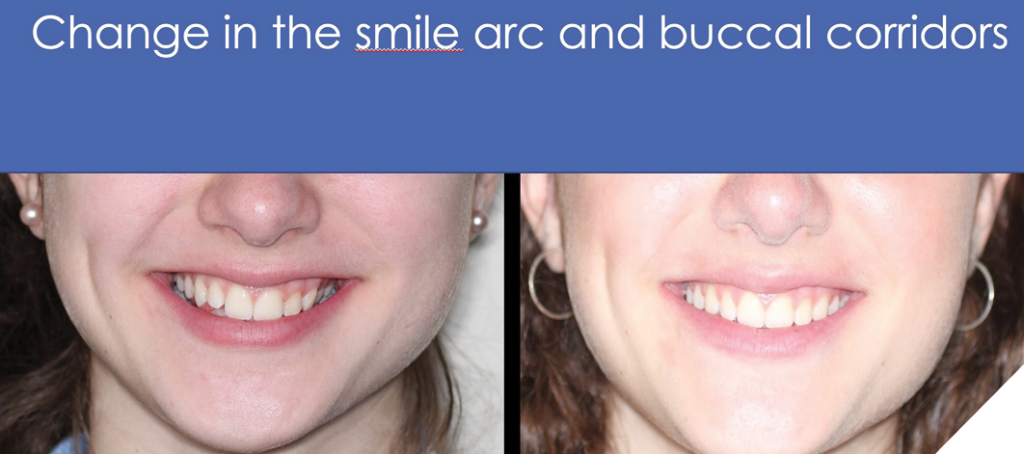
I started this case with Carriere Motion II on the right side to correct the asymmetry, the overbite, the midline, and the impacted 43. I wanted to help her as well for the asymmetry of her bite (class II subdivision), of the face and improve the buccal corridors.
All of that with no orthognathic surgery.
I have designed this approach that does everything in the beginning: aligning 6 front teeth on upper and treat all lower arch, correcting the class II, leveling Curve of Spee, addressing overjet and overbite, tipping, torquing, creating space and eventually making dental expansion. We can focus on everything right from day one. Another huge plus using this combination or hybrid treatment is that the patient will never wear the enamel of the teeth during parafunction since the tooth integrity will be protected during the orthodontic correction. No other system can stop or protect this adverse effect of grinding at night and tooth wear. In the same concept, I will use Vivera retainers with bite ramps, so the patient will stop the inevitable wear that comes from parafunction at night. A worn dentition comes with age and this wear can now be stopped when using the aligner system and Vivera retainers.
Also, I want to create an environment of treatment with the best aesthetic approach. I have been using invisalign since 2005 and when the Clear Carriere Motion arrived in 2016, I decided to use that in combination for my class II or class III’s. Not only choosing the Clear Carriere Motion with clear aligners, but also TREAT and CONTROL right from beginning, the upper front 6 anteriors, which is for the majority, the chief complaint. Also, we avoid the secondary effect of creating diastemas on the 6 upper anteriors when using the Carriere Motion on canines and let free the 4 incisors. Using invisalign from day one, I can also treat the lower arch from the beginning instead of holding the arch only with a retainer device (Essix). To push even more for aesthetic, I use the “short” Carriere and bond it on 1st upper pre-molar to the first molar instead of the canines, which used to be the most common way. When we bond the Carriere Motion on the first premolar, the class II elastics are even less visible and so are the eventual spacings created distal of canines instead of between the 6 upper anteriors. All the mechanics are then being pushed one tooth more in the back, which is a major plus for all patients searching for an aesthetic approach.
The treatment is highly efficient because we are doing everything from the beginning: tip-torque-align, treat the vertical and the horizontal. Bonding the Motion on upper 1st premolars will open the bite in a much more efficient way comparing to bond it on the canines. Simply because the secondary effect of the extrusion that comes with the Cl II elastics will be profitable with a tooth that has an occlusal table which the canine doesn’t have. The bite opening is even more profitable when we place the class II elastics on the lower second molar. Extruding a canine just won’t open the bite. I will exceptionally choose to bond it on canines when the case is class II with an open bite tendency.
With this design, the case acceptance is higher, treatment time plus number of appointments, much lower. Not to mention, almost no emergency appointment compared to conventional fixed systems. In my practice, I focus on the efficacy of systems, the flow of patient, profitability, and the pride of offering the best aesthetic combination treatment amongst all the traditional systems.
Patients are just amazed to see those fast results especially because we are treating their chief complaint from day one. They see their front teeth perfectly aligned in the first 6 months and the majority of them are finished within 12-16 months. Being able of treating everything first right from day one is a tremendous change in my practice and this nice momentum will occur because motivation is at its peak. We simply get the best patient collaboration in the beginning of treatment because they are simply highly motivated.
Fig. 1
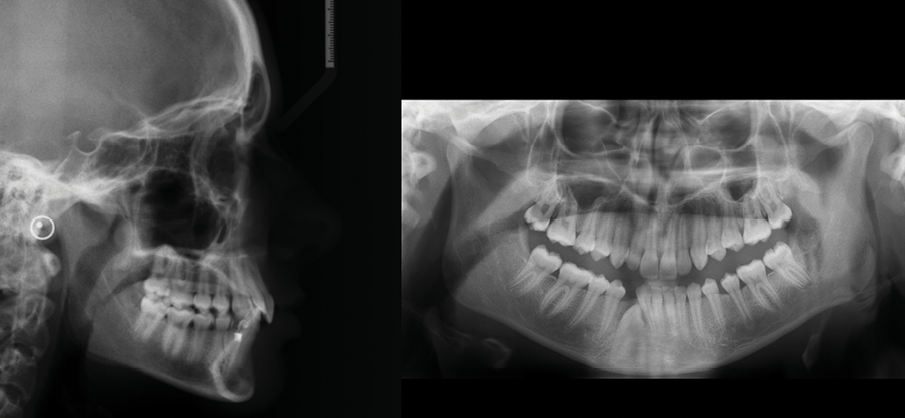
Fig. 2

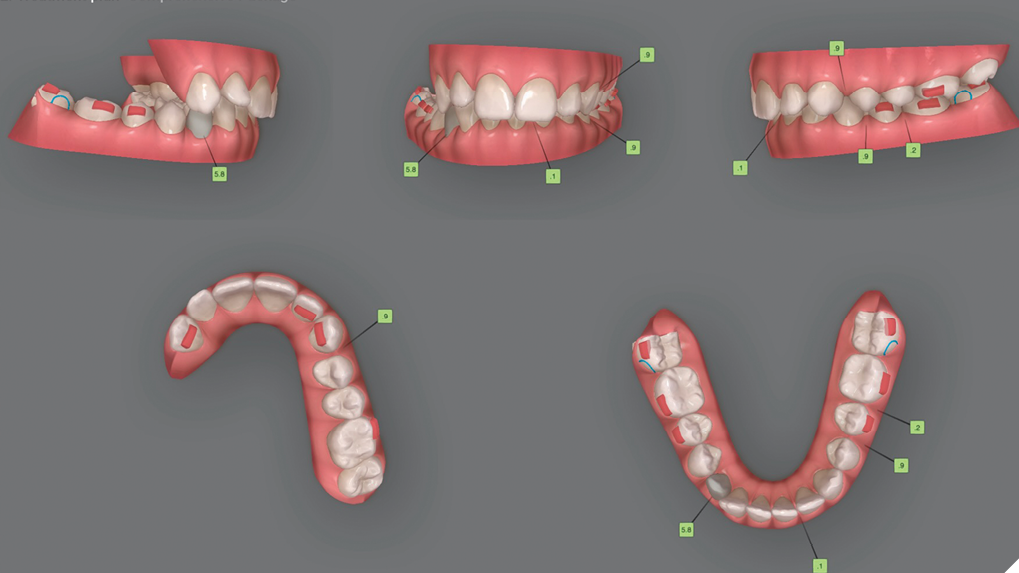
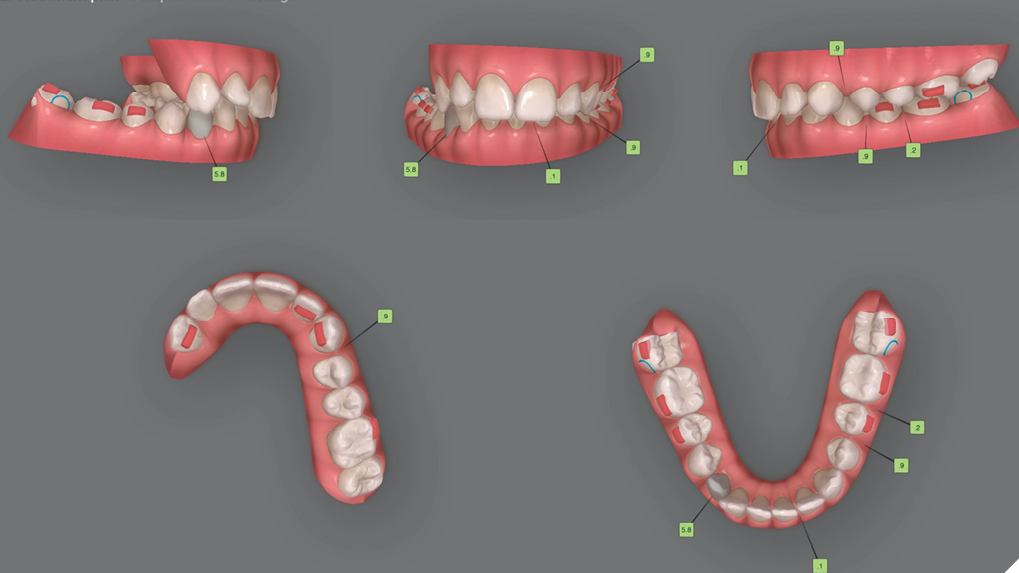
My strategies on the Clincheck Software
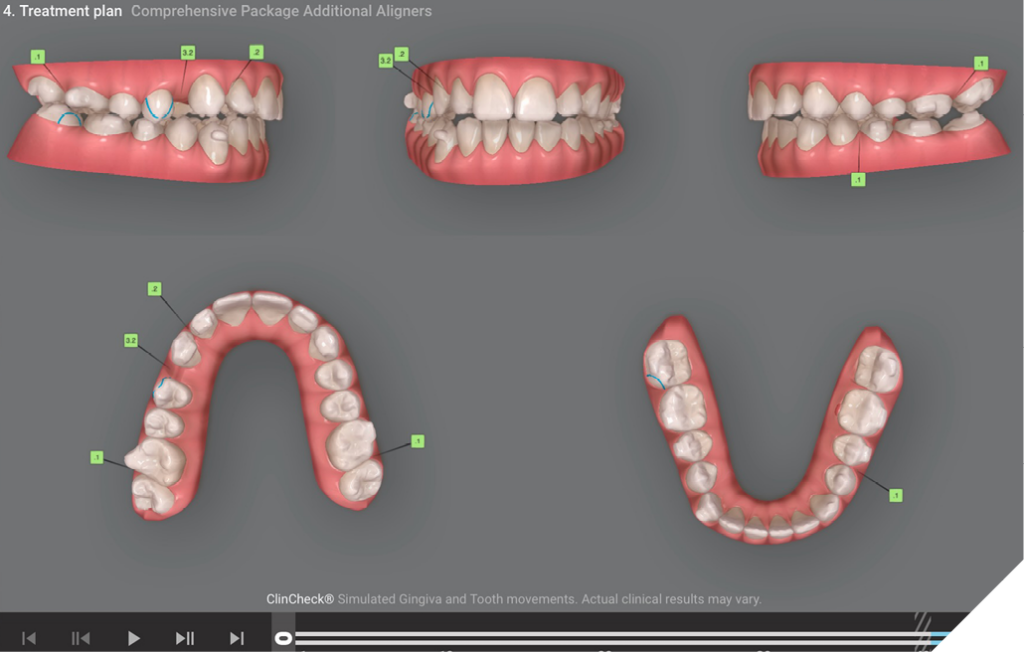
On the first Clincheck, I will ask to virtually remove upper 4-5-6-7 and treat only upper 3 to 3 for bilateral class II since the Clear Carriere Motion will be placed on upper 4’s. I usually treat the patient with this first phase over 6-8 months of aligners on adults and 4-6 months for teenagers. I will also design the attachments of upper six anteriors on the lingual side to elevate the elegancy of this approach.
I treat upper 3 to 3 and the complete lower arch. I will align, coordinate arches, level Curve of Spee and place button cutouts on lower 7’s. I will design class II elastics of Force 1 for the first 4 weeks and then Force 2 elastics for the rest.
Fig. 3
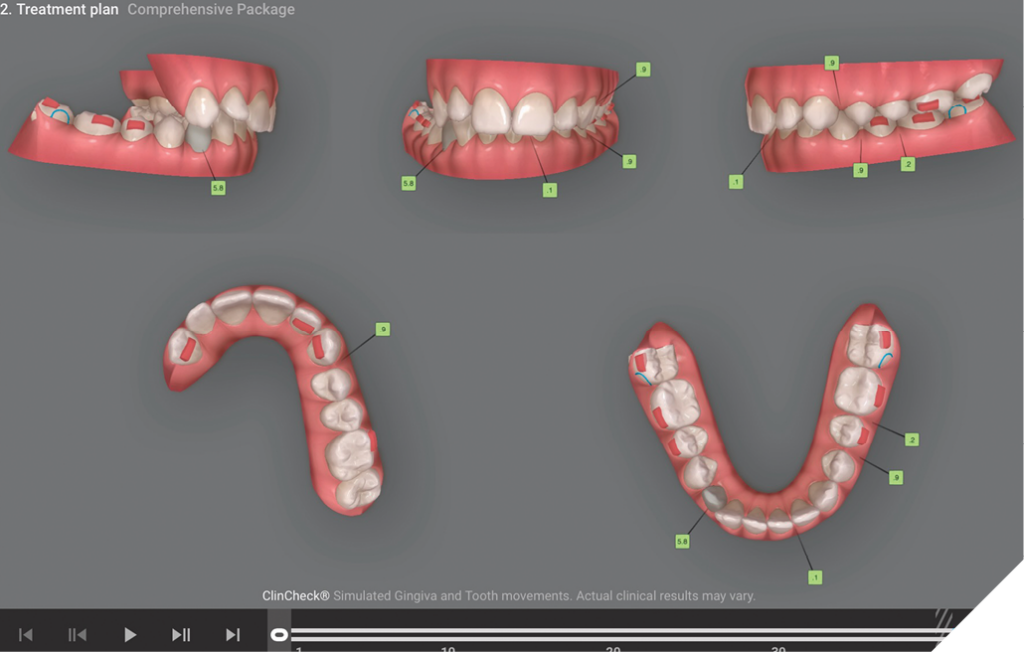
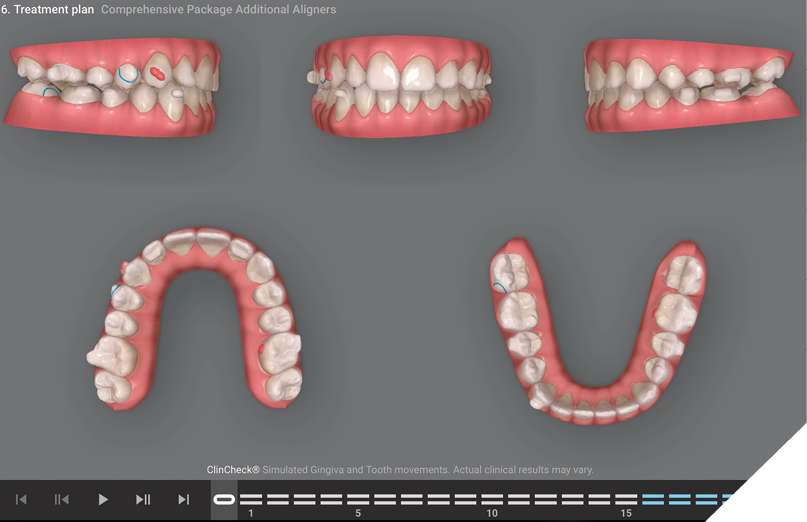
For my second round of aligners (refinement), I will ask Align to virtually remove the clear portion of the Carriere Motion that we will clinically remove at insertion of the refinement. The metal piece on the upper first molars will remain and act as an exceptional attachment for 3D control and will never wear out until the end of treatment. We then treat the 2 full arches, coordinating the width, and still have the option of using some other inter arch mechanics with class II or even in class III elastics.
Fig. 4
Force system for the impacted lower canine
Then in this clinical case of unilateral Carriere Motion, I also wanted to design the force system to simultaneously treat the impacted lower right canine. So, I will design my refinement ClinCheck with different possibilities of pulling with an elastic. I will request a double twisted 0,010 SS ligature connected on a bonded mushroom button to the impacted canine. A mushroom button will provide less side effects because the steel ligature can freely rotate around the neck of the button while we pull with the elastic. I requested a closed surgical approach and have the surgeon/periodontist make sure that the tooth will show of +1 mobility and, for sure, not be ankylosed. This approach is much better than with a gold chain, which is too flexible and impossible to hook and change the elastic by the patient. Depending on where this ligature will come out on the alveolar crest either buccal or lingual, I will design a canine pontic with a gingival convexity of at least 2mm. This geometry will create all of the aligners with the best anatomy to hook the elastic easily. The elastic can then be hooked at the gingival of this pontic, running at the incisal of the aligner and then reaching the steel ligature.
Fig. 5

I will cut and adjust the steel ligature like a ‘’J” hook and I will cover with composite at its end for more patient comfort. This design will be when the canine is positioned at lingual. If the canine and ligature are clearly buccal, I will the make 2 slits on the lingual of the pontic or on some occasions, on the lingual of the first premolar if there is a need to create not only an extrusive force but also a distalizing one at the same time. The patient will hook the elastic on the aligner first, then engage the aligner to eventually stretch the elastic on top of the aligner, to reach the steel ligature. This will automatically create the pull force we need to extrude and guide the impacted tooth. I got this idea in 2008, of treating impactions with the boot strap technique from the approach for an upper lateral not tracking well with an aligner. We all know that aligner therapy can only push. But with an elastic, we can create a pull force. If we can force the extrusion of a non-tracking lateral for 1mm, we could surely force the extrusion of an impacted tooth the same way for many millimeters. Depending on the total distance to stretch the elastic, I will use a 3/16’’ with 3.5 ounces of force for majority of cases. We also can use a vector more horizontal to better move mesio-distally or rotate the impacted tooth when we eventually see it clinically. The elastic can also be placed directly on the button when it is clinically possible.
Fig. 6

Fig. 7

Fig. 8

Fig. 9
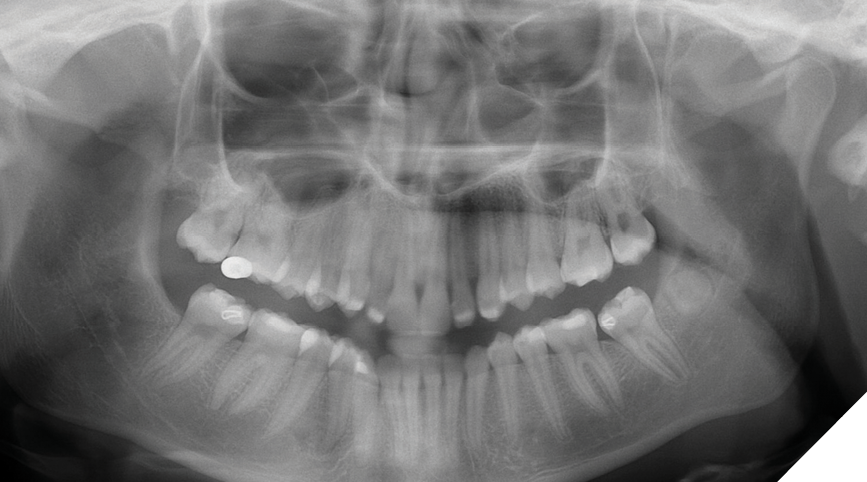
Fig. 10A

Fig. 10B
Total treatment time was 14 months, but some clinicians describe this as 12 months of treatment only, since we used to need 4-5 weeks of passive aligners in between the intervals of receiving the next series of aligners.
Fig. 11

Fig. 12
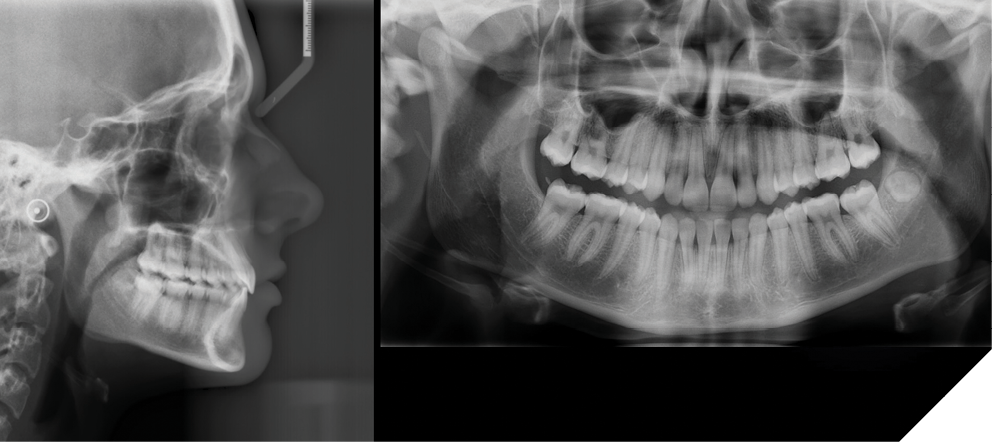
Fig. 13
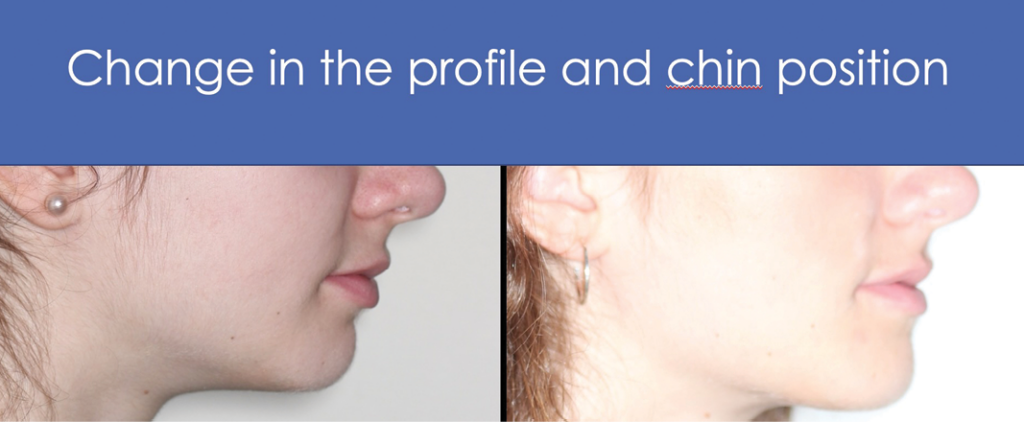
Fig. 14
The final scan will be for my final records and printing Vivera retainers from Align.
In conclusion, this case demonstrates the opportunity of designing multiple mechanics at the same time and applying them from the first day of treatment. This makes a win-win combination for the patient and for the treating doctor. Note that in this protocol, the patient was making bi-weekly change of her trays. 
Oral Health welcomes this original article.
Disclosure: Dr. Fournier is an invisalign Global Speaker since 2013.
About the Author

Dr. Christian Fournier is a graduate pedodontist and orthodontist from University of Montreal, Qc. He started using invisalign in 2004. He is a private solo practitioner using 100% only invisalign aligners for all cases since 2017. He has finished more than 4,500 comprehensive invisalign cases.