


Seniors aged 65 years and older now constitute the fastest growing segment of the population.1 With advancing age, many seniors will be affected by some type of physical or pathological limitation. To treat this significant patient group, dentists should adapt their offices to make them senior-friendly. Dentists need to be aware of and to consider the ever changing physical and cognitive status of these patients. The declines in the health status of the aging are dual in nature: there are the age-related deficits termed functional physiological limitations, as well as the pathological limitations. The visual problems of seniors provide a clear example of the duality of aging deficits and pathological limitations. With age, the number of rod and cone receptors in the eye decreases; this is a functional physiological limitation. However, pathologies of the eye such as cataract and glaucoma may additionally affect vision and cause a true disability. The treating dentist must be mindful of both the functional physiological limitations and the pathological limitations. This essay will present important considerations for dealing with the senior patient, including communication tips for successful treatment, as well as ways in which dental offices can be adapted to make them more welcoming, accessible, and responsive to the needs of this steadily increasing patient population.
Physical accessibility
Dental offices should be designed with physical accessibility in mind. Many senior patients use physical aids such as wheelchairs, or walkers. Stairs present a major physical hindrance to entering a dental clinic. Offices located in buildings with stairs should be accessible via the use of ramps to allow easy entrance and exit of the dental clinic.
The waiting room should be able to accommodate both wheelchairs and walkers. This means that there should be sufficient spaces between adjacent chairs, and the waiting room and hallways should be free of any obstacles that may possibly hinder navigation to the dental operatories. It is important that all carpets be taped down to prevent an accident such as a walker catching an edge. The reception desk should have a lowered counter for patients in wheelchairs to provide access to sign forms and use point of sale machines.2
Waiting room chairs should preferably have arm rests, as they greatly assist the mobile senior’s transition from the seated position to standing upright. Soft couches and chairs, although esthetically pleasing, present “up and go” difficulties for many seniors. If possible, reception desks should have a lowered counter to allow for wheelchair accessibility.
The dental operatories should be easy to enter and exit. The operatory should be designed to allow sufficient space if required for wheelchair transfer to the dental chair, and for the safe maneuvering of the walker. The senior patient is often accompanied by a family member or caregiver. It is a good idea to have sufficient space for a chair for the family member or caregiver to sit in the room, as the patient often feels less stressed with a familiar person within the room. Additionally, the presence of the caregiver or family member in the operatory serves to enhance communication between the patient and dental professional, and also provides for improved comprehension of the dental status and oral hygiene requirements of the patient.
Related article: Should gerontology be a dental speciality in Canada?
If there is a washroom in the office, it must be wheelchair accessible. It is prudent to have grab bars to allow for toilet transfer. The washroom must comply with municipal and provincial standards for handicapped accessible washrooms, and be large enough for the patient, any physical aids (walkers and wheelchairs) and for the patient’s caregiver, if necessary.
Patient movement from the waiting room to the dental chair
Patients may require assistance in going from the waiting room to the dental operatory, and then transferring to and from the dental chair. After the patient has registered, the receptionist should ask whether they would like assistance in moving to the dental operatory. Often, even ambulatory seniors, will appreciate being accompanied to the treatment room. For those patients using a cane, it is important to note which hand is holding the cane, as it is important to place the cane in the patient’s dominant hand at the end of the appointment.3 For those patients with walkers or in wheelchairs, it is imperative to ensure that there are no obstacles or hazards along the trajectory between the waiting room and the operatory. Once in the dental chair, the patient should be asked to move as close to the backrest as possible, thereby decreasing the possibility of injury to the dentist or staff member due to the strain of pulling the patient backwards.
Patients in wheelchairs should be asked if they prefer to be treated in the wheelchair or in the dental chair. Some patients prefer being treated in the wheelchair as many are customized to the patient. Furthermore, many of the newer electric chairs have a tilt action allowing for the patient to recline. For those patients wishing to be treated in the dental chair, they should be asked whether they need assistance in the transfer. Some patients may prefer to independently transfer to the chair using a sliding board. For those patients requiring assistance, this can be done by a one-person or two-person transfer. Prior to any transfer, the dental team should verify whether the patient is restrained in the chair by a seatbelt, that there are no devices attached to both the patient and chair such as a Foley catheter and urine bag, or a feeding gastric tube and food bag. Additionally, any blankets which could create a tripping hazard should be removed. The footrests of the wheelchair should be removed or positioned out of the way. The wheelchair should be positioned as close as possible to the dental chair with the wheels in a locked position. The arm of the dental chair should be removed or moved to allow for a clear transfer. The dentist and staff should ensure that their backs are straight at all times throughout the transfer.
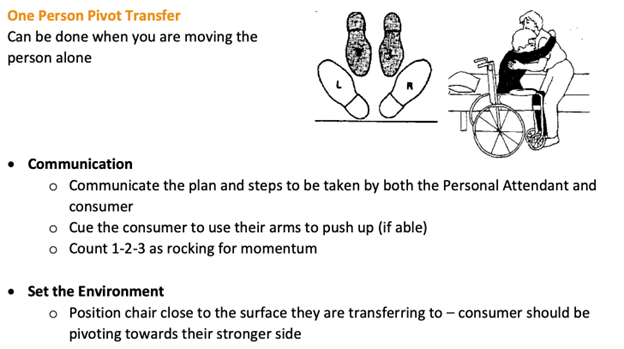
The one-person transfer should only be performed by an individual who is physically strong and able to lift the patient and return him/her back into their wheelchair if the transfer is unsuccessful. It is important for the patient to assist the dental team member. The patient will be asked to place their arms around the dental member’s shoulders, the dental team member will place their feet outside the feet of the patient and on a coordinated cadence, lift and pivot the patient into the dental chair4 (Fig. 1). Once the patient is stabilized in the dental chair, the arm of the chair should be returned to its usual position.
Fig. 1
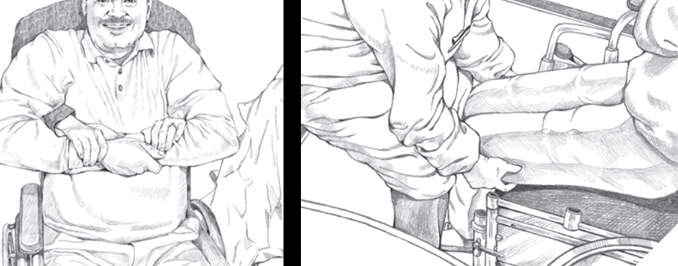
For the two-person transfer technique, the headrest of the dental chair is removed, and the dental chair is lowered to the height of or lower than the wheelchair. The removal of the headrest decreases the amount of lifting required in the transfer. The patient is asked to cross their arms, and the first dental team member will then position their arms under those of the patient and take hold of the patient’s wrists. The second team member then places their arms under the patient’s thighs and in coordination the two team members lift the patient into the dental chair5 (Fig. 2). The arm rest must be returned, and the headrest is replaced. The methods used to transfer the patient should be noted in the chart. This will allow the other dental professionals in the office to immediately know the best transfer option.
Fig. 2
Finally, it is important to be aware that certain medications such as antihypertensives and/or a delayed physiological postural aging response may cause many senior patients to be dizzy and unsteady after laying supine in the dental chair for an extended period of time during dental treatment. Consequently, patients should not be asked to stand up immediately upon the completion of treatment. They may require extra sitting time in the dental chair as well as assistance in getting out of the chair. This extra time should be built into the schedule in order to decrease stress upon both the patient and staff.
Sensory considerations
Most older patients will have functional and pathological changes affecting their vision and hearing. The decreased number of rods and cones in the retina will affect their ability to see in dim lighting and also affect depth perception. Glare can be a problem for patients with cataracts. Any stairs should be well lit and the edges of the steps should be clearly identified with bright coloured tape in order to aid the patient with depth perception difficulties.
Music should not be played at loud volumes as the patient may have hearing loss and the competition between the health professional and the extrinsic sounds will make communication difficult. It is important that all verbal communications be presented in an even tone and repeated in a different manner. For example, in discussing the need for a restoration, one could say that “this tooth requires a filling” and repeat the message again differently by saying “this tooth has a cavity”. The dentist should ensure that the patient comprehends the treatment and may politely inquire as to whether the patient understands the treatment required. The use of large diagrams and clear fonts will enhance communication.
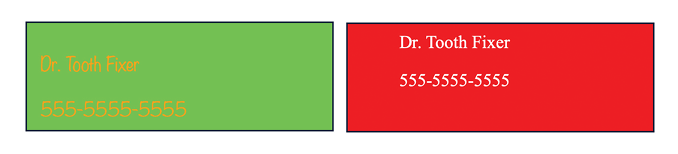
For those patients with hearing aids, the dentist should never assume that the patient is wearing his/her hearing aids, or that they are actually turned on! Many seniors may not have or wear their hearing aids. This may be due to their denial of the aging process, high costs, difficulty in manipulating the controls, and/or the hearing aids draw attention to their handicap.6 If the patient must read or interpret chairside drawings or consent forms, ensure that they are wearing their glasses. All written material should be printed in a large, clear font with appropriate background contrast (Fig. 3). Please note that all fonts within this example are the same size. The background and script design must be easy to read. This is vitally important for patients receiving post-surgery instructions.
Fig. 3
Informed consent
The subject of informed consent by the senior patient is complex and is dealt with at length in another article within this issue of Oral Health. In summary, it is essential for the dentist to assess whether the patient has the mental capacity to give full and informed consent to dental treatment. Consent must be obtained via a thorough but simple discussion of the procedures proposed and how the patient’s medical history may affect their treatment plan. If a patient is unable to comprehend the discussion, the dentist may determine that the patient does not have the capacity to legally consent to treatment. This should be clearly indicated in the patient chart and consent be obtained from the legal guardian.
Empathy and patience
The entire dental team should exhibit empathy, kindness, patience, and understanding. These attributes must start with the reception staff. It is important for staff to be aware that many senior patients may have inherent anxieties about dental treatment. This may lead to increased stress and a lack of comprehension and mental acuity. As some patients may have a difficult time completing forms such as the medical health questionnaire, it may be appropriate to have the front desk staff assist the patient in a confidential area of the waiting room. Empathy and kindness will decrease anxiety in patients.7
Appointment scheduling
The timing of appointments should consider the patient’s medical status, transportation needs, treatment complexities, and the ability of the patient to withstand the stress of being supine for extended periods of time. Patients may require multiple confirmation phone calls. From a medical perspective, circadian rhythms and medications will affect a patient’s blood pressure, and platelet function.8,9 These patients should ideally be scheduled in the morning after they have taken their morning medications. Blood pressure is more likely to be stable and under control during the early part of the day. For those patients taking antiplatelet or anticoagulant medications (e.g., aspirin, warfarin, DOACs), an early appointment is advantageous as it allows for sufficient time during office hours to manage any potential post-procedure bleeding.
Oral hygiene and the senior patient
Many seniors have dexterity issues due to chronic conditions such as arthritis. This may decrease the ability of the patient to adequately brush their teeth. The use of a battery-operated power toothbrush such as the iO Power brush will enhance the efficacy of brushing versus a manual toothbrush.10 In addition to its increased efficacy, the larger handle of the power toothbrush allows for the patient to grasp it easier. A fluoridated toothpaste, and floss aids such as a water flosser or floss picks are also beneficial for the senior patient.
Conclusion
It is hoped that this article has shed light on the importance of adapting the dental office to the needs of our aging patient population. Improvements in accessibility and communication, as well as consideration of the physical and sensory limitations of aging are all key factors in the provision of safe and effective dental treatment for the senior patient. It is essential that the entire dental team is sensitive to and aware of the physical and cognitive limitations that come with aging. Providing a safe, inclusive and welcoming office environment can go a long way in reducing patient stress and barriers to dental care; and consequently, has the benefit of enhancing not only the patient-dentist relationship, but also the oral health and overall health of the senior patient. 
Oral Health welcomes this original article.
References
- https://www.cihi.ca/en/infographic-canadas-seniors-population-outlook-uncharted-territory.
- Rashid-Kandvani F, Nicolau B, Bedos C. Access to Dental Services for People Using a Wheelchair. Am J Public Health. 105(11):2312-7, 2015
- https://orthoinfo.aaos.org/en/recovery/how-to-use-crutches-canes-and-walkers
- https://www.cheshirelondon.ca/wp-content/uploads/BackCare-Handout.pdf
- US department of Health and Human Services (2009) https://www.nidcr.nih.gov/sites/default/files/2020-10/wheelchair-transfer-provider-guide.pdf
- Jerger J, Chmiel R, Wilson N, Luchi R. Hearing impairment in older adults: new concepts. J Am Ger Soc 43:928-35, 1995.
- Corah, N L; O’Shea, R M; Bissell, G D; Thines, T J; Mendola, P. The dentist-patient relationship: perceived dentist behaviors that reduce patient anxiety and increase satisfaction. J Am Dent Assoc. 116(1):73-6, 1988.
- Chrusciel P, Goch A; Banach M; Mikhailidis DP; Rysz J; Goch JH. Circadian changes in the hemostatic system in healthy men and patients with cardiovascular diseases. Med Sci Monit 15(10):RA203-208, 2009.
- Thomsen MB. Twenty-Four Hour Rhythms in Cardiovascular Physiology. Acta Physiol (Oxf). 241(11):e70116, 2025.
- Chan AKY, Tsang YC, Chu S, Chu CH. Comprehensive Strategies for Preventive Periodontal Care in Older Adults. Geriatr.. 10(3), 2025.
About the author

Dr. Michael Wiseman completed his dental degree in 1985 at McGill University. He presently is a part-time Clinical Associate Professor at McGill University Faculty of Dental Medicine and Oral Sciences. He has a full-time practice, and additionally provides care at a variety of long-term hospital centres in Montreal. He is the Founder of the McGill Outreach Program which provides free care to the needy of Montreal. Dr. Wiseman has lectured nationally and internationally and has published many peer reviewed papers and book chapters.