


The quality of peri-implant soft tissue plays a pivotal role in the long-term success of dental implants. Thicker peri-implant mucosa, particularly when accompanied by adequate keratinized mucosa, is associated with enhanced aesthetic outcomes, reduced risk of peri-implant diseases, and improved patient satisfaction.
The peri-implant soft tissue complex, encompassing the keratinized mucosa (KM), mucosal thickness (MT), supra-crestal tissue height (STH), and peri-implant bone thickness (PBT), significantly influences the biological and esthetic outcomes of dental implants. A robust peri-implant mucosa acts as a barrier against microbial invasion, thereby reducing the risk of peri-implant diseases such as mucositis and peri-implantitis.1,4,5
Ideal characteristics of peri-implant soft tissue
Mucosal Thickness (MT): Studies suggest that a MT of ≥2 mm is optimal for preventing complications. Thicker tissues are less prone to recession and provide better esthetic outcomes.2
Keratinized Mucosa Width (KM): A KM width of ≥2 mm is recommended to facilitate oral hygiene maintenance and reduce inflammation.3,4,5
Supra-Crestal Tissue Height (STH): An STH of ≥3 mm is considered adequate to prevent bone resorption and maintain implant stability.4
Peri-Implant Bone Thickness (PBT): A PBT of ≥2 mm is desirable to support the implant and prevent bone loss.5
Read related article: Peri-implantitis: How to Reduce Risk and Manage Implant Failure?
Management of insufficient peri-implant soft tissue
When peri-implant soft tissue is insufficient, various surgical interventions can be employed:5,6,7
Connective Tissue Grafts (CTG): CTGs are considered the gold standard for augmenting peri-implant soft tissue thickness. They have been shown to improve esthetic outcomes and reduce the risk of peri-implant diseases.6,7 Connective tissue graft can be done at the time of implant placement, at second stage surgery, or after the healing of second stage surgery (for example, if relining bone graft was done at the time of second stage surgery). Sometimes connective tissue graft is also used to regain vestibule and create attached tissue after major bone grafting in esthetic zone. This approach is typically adopted after second stage surgery as well.
Free Gingival Grafts (FGG): FGGs can increase KM width but may have a higher risk of graft failure compared to CTGs.4 FGG provides the best approach in regaining the vestibular depth and creation of thick attached gingiva in cases of implant therapy involving significant bone grafting. This approach is typically adopted in non-esthetic zone cases.
Soft Tissue Substitutes: Materials such as acellular dermal matrix and xenogenic collagen matrices can be used as alternatives to autogenous grafts, offering reduced morbidity and practically unlimited supply.3 However, various studies have shown that autogenous tissue grafts can outperform these soft tissue substitutes.
Prevention of complications associated with poor soft tissue quality
To prevent complications related to inadequate peri-implant soft tissue, the following strategies are recommended:
• Adequate surgical planning: Ensure sufficient bone and soft tissue volume before implant placement to accommodate prosthetic requirements. In case of deficient bone or soft tissue, surgical planning should include strategies to address those deficiencies.
• Proper implant positioning: Optimal positioning of the implant can facilitate the development of adequate soft tissue profile and prevent potential complications.
• Proper restorative design: Proper restorative design ensures proper soft tissue emergence profile, creation of mucosal barrier against microbial invasion and allows for optimal plaque control.
• Maintenance of oral hygiene: Educate patients on the importance of maintaining good oral hygiene to prevent plaque accumulation and subsequent inflammation.
• Regular monitoring: Implement regular follow-up visits to monitor the health of peri-implant soft tissues and address any issues promptly.
Here we report two cases to demonstrate the application of FGG and CTG in creation of optimal peri-implant soft tissues.
Case 1
A 76-year-old female patient was referred to our clinic for the implant therapy to restore missing 25, 26. Patient reported high blood pressure that was controlled by medications. Patient presented with significant horizontal bone deficiency at sites 25, 26. Furthermore, the soft tissue phenotype was poor with lack of keratinized tissue and reduced vestibular depth. The surgical plan involved placement of implants using surgical guide with simultaneous bone grafting using the traditional guided bone regeneration approach. A significant portion of the buccal aspect of implants was exposed and outside the alveolar bone. Particulate bone graft comprising of autogenous bone chips mixed with allograft and xenograft was packed on the exposed buccal aspect of the implants. Resorbable collagen membrane was placed and secured using a combination of tacks and sutures. The site was then closed ensuring passive primary closure. After 4 months of healing, the second stage surgery was carried out. The goal of the second stage was not only to expose the implants but also to create a zone of keratinized attached gingiva, increase gingival thickness, remove frenal pull and regain vestibular depth. This was achieved through FGG. Subsequent to the healing of FGG, the implants were restored and have been stable in function for over 3 years.
Fig. 1
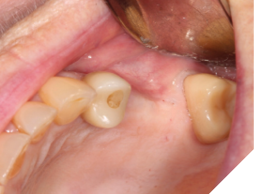
Fig. 2
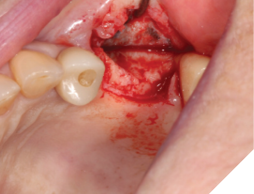
Fig. 3
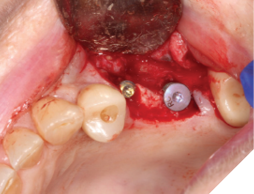
Fig. 4
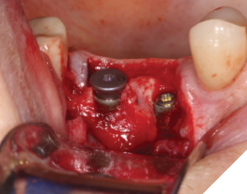
Fig. 5

Fig. 6

Fig. 7

Fig. 8

Fig. 9
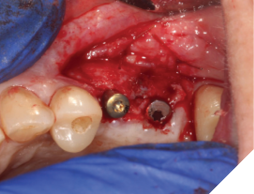
Fig. 10

Fig. 11

Fig. 12

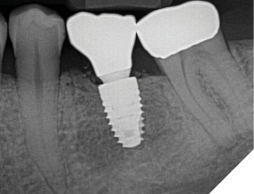
Case 2
A 56-year-old male patient without significant medical history was referred to our practice for the implant therapy at 36. The tooth was extracted by the referring dentist and no bone grafting was done. After clinical and radiographic exam, a surgical plan was devised that involved placement of dental implant with simultaneous bone grafting. A 4.8mm diameter implant was placed using surgical guide. The bone width on the buccal aspect of the implant was less than 1.5mm. Khoury technique was used for the augmentation of the buccal bone. Briefly, a thin cortical bone plate was harvested from the retromolar area. The bone plate was fixated on the buccal aspect of the implant using bone fixation screws (Profix Screw System by Osteogenics). This led to creation of bone box. This bone box was filled with autogenous bone chips harvested from the retromolar area and from thinning of the cortical bone plate. Blunt dissection of lingual flap and periosteal release incision of buccal flap allowed for passive primary closure. After three months of healing, the second stage surgery was performed. Upon flap elevation, over 5.5mm of beautifully regenerated vital autogenous bone was noted. The implant was completely buried under the bone. The fixation screws were removed, and the healing abutment was placed. A thin layer of xenograft was placed over the newly regenerated autogenous bone to counter any potential resorption as sometimes noted in cases managed using autogenous bone. This layer of xenograft was covered by a resorbable collagen membrane. At this stage, an FGG was harvested from the palate. The overlying epithelium was removed to convert the FGG into a CTG. The CTG was then sutured on the inside of the buccal flap and the site was closed and allowed to heal. Following the healing of the second stage surgery, the implant was restored and has been successfully in function for four years as of the writing of this report.
Fig. 1

Fig. 2

Fig. 3

Fig. 4

Fig. 5

Fig. 6

Fig. 7

Fig. 8
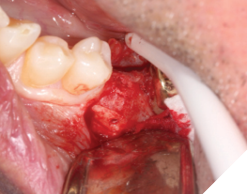
Fig. 9

Fig. 10

Fig. 11

Fig. 12

Fig. 13

Fig. 14

Fig. 15
Conclusion
The quality of peri-implant soft tissue is a critical factor in the success of dental implants. Thicker, keratinized mucosa provides a protective barrier against microbial invasion, enhances esthetic outcomes, and reduces the risk of peri-implant diseases. When soft tissue is insufficient, surgical interventions such as CTGs can be employed to augment tissue volume. Preventive measures, including adequate surgical planning, proper implant positioning, and maintenance of oral hygiene, are essential to mitigate complications associated with poor soft tissue quality. 
Oral Health welcomes this original article.
References
- Bienz SP, et al. The influence of thin as compared to thick peri-implant soft tissues on aesthetic outcomes: A systematic review and meta-analysis. Clin Oral Implants Res. 2022;33(6):755-765.
- Thoma DS, et al. Effect of peri-implant mucosal thickness on esthetic outcomes and the efficacy of soft tissue augmentation procedures. Clin Oral Implants Res. 2022;33(6):766-776.
- Schwarz F, et al. Soft-Tissue Augmentation for Management of Periimplant Diseases. Implant Dent. 2018;27(3):309-315.
- Zucchelli G, et al. Soft-Tissue Conditions Around Dental Implants: A Literature Review. J Clin Periodontol. 2019;46(10):1073-1086.
- Sanz-Martín I, et al. Management of Soft Tissue Defects Around Single Implants: A Systematic Review of the Literature. J Clin Periodontol. 2022;49(3):257-269.
- Gamborena I, et al. Soft tissue-related complications and management around dental implants. Periodontol 2000. 2019;79(1):173-192.
- Al-Nawas B, et al. A modified surgical approach for hard and soft tissue reconstruction of severe periimplantitis defects: laser-assisted periimplant defect regeneration (LAPIDER). Int J Implant Dent. 2020;6(1):22.
- Bressan E, et al. Influence of soft tissue thickness on marginal bone level around dental implants: A systematic review with meta-analysis and trial-sequential analysis. Clin Oral Implants Res. 2023;34(1):1-13.
- Lemos CAA, et al. Influence of vertical soft tissue thickness on occurrence of peri-implantitis in patients with periodontitis: a prospective cohort study. J Clin Periodontol. 2020;47(3):324-331.
- Roccuzzo M, et al. The clinical significance and application of the peri-implant phenotype in dental implant surgery: a narrative review. J Clin Periodontol. 2023;50(5):563-577.
About the author

Dr. Mo, as his patients like to call him, is a certified Periodontist, the Director and Principal Clinician at the Cityview Periodontal and Oral Surgery Centre, Regina. Dr. Mo mentors’ dentists nationally and internationally. He regularly conducts hands on courses and workshops for dentists. He has published numerous articles and book chapters. His surgical work has been used by other authors for their scientific endeavors in research article and book chapter. He is an international speaker, who likes to unfold and simply the connection between academic scientific literature and real-life clinical practice. He can be reached at mohammad.javaid2@yahoo.com.