


When a tooth is out of place, it can affect both the aesthetics of a smile and the overall function of the bite. However, not all cases of misalignment require complex orthodontic treatment. In many instances, creating an illusion of a properly aligned smile can be just as effective in achieving the desired results. Through techniques like cosmetic bonding, veneers, and strategic contouring, dental professionals can mask misalignments and give the appearance of straight, evenly spaced teeth without the need for lengthy procedures. This approach is particularly valuable for patients who desire a quick, minimally invasive solution, or those who are not yet ready for orthodontic intervention. Understanding how the art of illusion can enhance both confidence and comfort is crucial for modern dental care, where appearance often holds as much weight as function. One of the most difficult cases of malpositioned teeth involves canines, especially when they are in the position of the lateral incisor.
Case presentation
A 45-year-old male presented with a chief complaint of “I do not like my smile and different sizes of my teeth. I want them more symmetrical.” Upon intraoral examination (Figs. 1-3), multiple esthetic concerns were noted: tooth size discrepancies, gingival height discrepancies, variations in color, and position of the upper anterior teeth. The biggest challenge in correcting the patient’s chief complaint would be the upper left cuspid positioned in the space of the lateral incisor. Due to the size difference between cuspids and lateral incisors, creating the illusion that a cuspid is a lateral is often a daunting task.
Fig. 1

Fig. 2

Fig. 3

After reviewing treatment options with the patient, a decision was made to treat the upper four anterior teeth. A cosmetic photo series, along with intraoral scans, was acquired and sent to the laboratory for a digital design with specific instructions (Fig.4). The initial design (Fig. 5) was approved, files printed, and a provisional matrix was fabricated.
Fig. 4
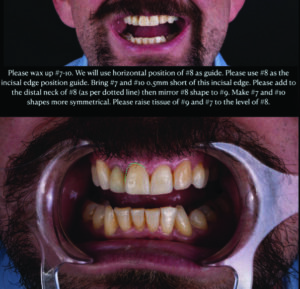
Fig. 5

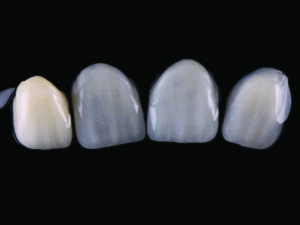
When the patient presented for treatment, the teeth were anesthetized, and a rubber dam (Nictone Heavy Gauge) was placed using the split dam technique and the palate was sealed with Futar-D (Kettenbach). Initial depth cuts were made in teeth #8 (11) and “10” (22), and the crown was removed on tooth #7 (12) (Figs. 6-9). The teeth were noted to be correctly positioned horizontally. The reason tooth number 9 was not prepped initially is that it is positioned lingually to the finally horizontal position. Therefore, we can place the final provisional design over this tooth later and prep through it to ensure minimal tooth removal. Once the rough preps were completed, a bisacryl provisional was placed on the preps utilizing the final smile design (Figs. 10 and 11). With the provisional in place, another set of depth cuts were completed through the matrix to ensure both adequate and minimal removal of tooth structure. This technique, known as the APT technique, was developed by Galip Gurel (Figs. 11-13). Once all the preparations were completed and verified, conventional impressions were taken with light and heavy body PVS (RSVP, Cosmedent), along with a bite registration and an opposing model. Prep photos were taken with the Ivoclar Natural Die prep shade guide (Figs. 14-16). Since the preparation depth was different for each tooth, the prep shades were not uniform, so it was critical to accurately capture the correct prep shade for each tooth. The maximum thickness of the final restorations was .5mm, so the underlying shade variation could compromise the final esthetic outcome and challenge the laboratory to create four restorations with identical shades. Once the prep photos were completed, a provisional was fabricated and cemented with spot etch and flowable resin (Figs. 17 and 18). The patient was dismissed and returned one week later for approval of the provisional restorations. The case was sent to the laboratory for fabrication of three lithium disilicate veneers and a full crown. The restorations were designed to replicate the provisionals and milled from lithium disilicate blocks (Fig. 19). Dies were made for each preparation in the appropriate shade (Figs. 20 and 21) to ensure a uniform outcome in color. As seen in Figure 23, three of the four restorations were very thin and would be affected by the underlying tooth color. The final restorations were completed by Aaron Johnson, CDT of CMR Labs (Fig. 22).
Fig. 6

Fig. 7

Fig. 8

Fig. 9

Fig. 10

Fig. 11

Fig. 12

Fig. 13

Fig. 14

Fig. 15

Fig. 16

Fig. 17

Fig. 18

Fig. 19

Fig. 20

Fig. 21

Fig. 22
On the day of seating, the patient was anesthetized and the provisionals removed. The restorations were tried in to assess fit and for patient approval. Once approved, the custom rubber dam was placed (Nictone) isolating from canine to canine and secured with primary clamps (W2, Hu Friedy) over the bicuspids. Once secured, the secondary clamps (B4, Brinker, Coltene Whaledent) were applied to the centrals for a two-by-two insertion technique (Fig. 24). The preps were air abraded using a Prep Start (Danville), veneers tried in (Fig. 25) and then the bonding protocol was initiated. The teeth were etched with phosphoric acid (Select Etch HV, Bisco), rinsed and dried with a cotton roll to avoid desiccation. Three coats of bonding agent (All Bond Universal, Bisco) were applied, thinned with hot air and cured for 15 seconds. The veneers were cemented with Choice 2 cement (Bisco). All excess cement was removed and each surface was cured for 40 seconds per the manufacturer’s instructions. The B4 clamps were then moved to the laterals and the same sequence was followed (Fig. 26). Following final cure, the rubber dam was converted to a split dam (Fig. 27) for final evaluation, polishing of the margins, and removal of any excess cement. The patient was dismissed and returned in four weeks for post op photos (Figs. 28-30). The final result was favorable in terms of color and shape. With a good design and excellent ceramics, the cuspid was transformed into a lateral incisor, improving overall symmetry and harmony of the smile.
Fig. 23

Fig. 24

Fig. 25

Fig. 26

Fig. 27

Fig. 28

Fig. 29

Fig. 30

In conclusion, while traditional orthodontic treatments are often necessary for significant misalignments, cosmetic dental techniques offer a viable alternative for patients seeking faster, less invasive solutions. By utilizing methods like bonding, veneers, and contouring, dental professionals can effectively correct the appearance of misaligned teeth, enhancing both aesthetics and function. This approach is particularly beneficial for individuals with alignment issues, such as mispositioned canines, where the visual result can be transformative without the need for extensive procedures. As dental care continues to evolve, these innovative solutions provide a valuable option for those who wish to improve their smile and boost their confidence, without compromising comfort, tooth structure, or undergoing lengthy treatments. 
Oral Health welcomes this original article.
About the author

Dr. Adamo Notarantonio is a graduate of the State University of New York at Stony Brook School of Dental Medicine (2002), where he received honors in both removable and fixed prosthodontics. Dr. Adamo was Accredited by the American Academy of Cosmetic Dentistry in 2011, and received his Fellowship in the AACD in 2018. He is the current President of the AACD, Credential Examiner and Fellowship Chairman. Dr. Adamo is a graduate and faculty of the Kois Center. He has received his fellowship in the International Congress of Oral Implantologists. Dr. Adamo has been published in multiple dental journals and lectures nationally and internationally on such topics as CAD/CAM dentistry, implant dentistry, cosmetic dentistry, composite dentistry and dental photography.