
Temporomandibular disorders (TMDs) are a group of musculoskeletal conditions (MSK) primarily affecting the jaw muscles, and the temporomandibular joint (TMJ). These disorders are increasingly prevalent, with a rising number of patients seeking treatment for associated pain and dysfunction. They affect approximately 1 in 12 adults and are now the second most commonly occurring musculoskeletal condition disorder following back pain.1 TMDs are also a leading cause of odontogenic pain.2
It is our role as healthcare practitioners to thoroughly examine and identify the possible causes of the patients’ pain and refer/treat accordingly. The more we can demonstrate effective outcomes increases patient trust in our ability to ease their pain and return them to normal function.
The most commonly occurring TMDs are MSK. This is defined as injuries involving the muscles, bones, tendons, ligaments and soft tissues, that are either aggravated or relieved from specific positions or motions. While many strains or sprains to the face or jaw can be acute or traumatic injury, TMDs are more commonly overuse, cumulative or repetitive strain injuries. TMDs can also be the result of disease, active or passive altered mechanics, the long-term effects of physical trauma, degenerative changes, medication induced, psychological and the list goes on. The vast majority of these can be treated conservatively using self-directed or manual therapist assisted care with multi-disciplinary collaboration.
The need for effective, standardized, evidence-based treatment options has increased with the increase in prevalence. Similarly, the increased prevalence requires primary healthcare practitioners to accurately identify TMDs and understand the appropriate therapeutic interventions for the best outcomes of the patient.
This article aims to soft outline the steps and processes for dentists to follow and to be able to rule-out red flags, examine thoroughly to determine odontogenic vs musculoskeletal causes of pain, and the importance of manual therapists and dentists working together in a collaborative manner.
The evolving roles of dentists
The approach to diagnosing and managing TMDs has evolved significantly. While dentists remain the primary point of contact for odontogenic patients, their role has expanded to being a primary point of contact for TMDs. With a prevalence of 1 in 12, the average dentist will most likely be presented with a TMD almost daily. Dentists will serve as TMD diagnosticians, provide initial directions on conservative care, and coordinate referrals when necessary.
Diagnosis
Standardization of diagnosis has progressed in recent years with tools such as the Diagnostic Criteria for Temporomandibular Disorders (DC-TMD).7 The DC-TMD is a tool/process with high sensitivity and specificity for primary health care practitioners to rule in TMDs. Expertise in ruling in or out red flags or odontogenic causes is a crucial first step prior to identifying MSK pain. Dentists must rely on their training and experience and a thorough history and examination, prior to engaging the DC-TMD to ensure patient safety. Following the DC-TMD may be applied to help the patient understand what MSK condition may be causing their pain.
Similarly, the patient once diagnosed needs to understand TMD rehabilitation emphasizes a biopsychosocial model of care, advocating for a conservative, multidisciplinary rehabilitation approach before considering aggressive interventions. The first step in TMD management is an accurate diagnosis and self-care strategies. If these fail, the next phase involves practitioner-directed conservative interventions.3
Manual therapists and allied health
The first intervention for MSK care is prescribing evidence-based self-care strategies. When this intervention fails, or patients lack compliance or discipline, referrals for manual therapy and allied health play a role.8 The MSK aspect of TMD treatment is often managed by chiropractors, physiotherapists, massage therapists and various other types of manual therapists. However, the effectiveness of treatment is determined not by the type of provider, but by the specific interventions used. Across all MSK conditions it is scary to think 81% of practitioners chose treatments that have no recommendation and 43% chose treatments that were recommended against.9,10
When evidence-based recommended/guideline care is ignored (either by dentist or manual therapist), patients become predisposed to prolonged and chronic pain, unnecessary medications or aggressive non-conservative interventions. In 2023, the British Medical Journal (BMJ) published the Rapid Recommendation on the Management of Chronic Pain Associated with TMD’s,5 strongly recommending:
- Jaw exercises
- Jaw stretching
- Trigger point therapy
- Postural exercises
- Cognitive Behavioural Therapy
Similarly, a 2020 BMJ article introduced a new rehabilitation paradigm for soft-tissue injuries that focus on progressive loading and return to normal function known as PEACE & LOVE.4 This is a stark contrast to the previous models of avoidance and accommodation of pain.
The Oral Facial Pain Training (OFPT) Program
To effectively treat TMDs, manual therapists need to be better trained in evidence-based, recommended/guideline care. Manual therapists, allied health professionals with advanced training or experience working collaboratively with dentists or dental specialists is an already proven successful model for the treatment of TMDs and decreased complications for patients.8 This collaboration has yielded increased accuracy in diagnosis, better outcomes for patients, a greater focus on TMDs as a disease and increased collaborative research efforts.
Specific to manual therapists, many dentists and family physicians are unsure of how or where to identify those with advanced training who practice evidence-based, recommended/guideline care. This can result in patients receiving ineffective or even harmful treatments, delays in appropriate care and prolonged pain. We now know prolonging care alone can lead to central sensitization of the patient, which can lead to chronic pain.
Recognizing this challenge, a dedicated effort began in 2016 to develop the Oral Facial Pain Training (OFPT) program. This initiative, based on two decades of clinical experience, research and collaboration with major health institutions and health professionals, aims to:
- Expand our reach and train practitioners in evidence-based TMD care.
- Reinforce adherence to evidence-based, recommended/guideline care.
- Improve patient outcomes through safe, conservative interventions.
The OFPT program integrates years of patient care, research, the DC-TMD, the NASEM recommendations, evolving rapid recommendations and modern rehabilitation paradigms, to create an effaceable plan to treat TMDs and other acute injuries to the head, face and jaw. Similarly, we are seeing consistent comorbidities in presentation with TMDs and a goal to address these are a primary focus of the OFPT program. It emphasizes information, such as:
- Training in assessment, diagnosis, imaging review, rehabilitation, and comorbidity management.
- Pain reduction strategies.
- Exercises that mimic natural jaw function.
- Allied health collaboration strategies.
Successful case examples
Below are two case studies that illustrate with the correct training, dentists and manual therapists working together identified accurately causes of pain and made the appropriate recommendations and applied appropriate interventions.
Fig. 1

Case study 1: Patient AB
A 60-year-old patient who identifies as a female presented to our clinic with a five-month history of left sided jaw, ear, and head pain with continuous pain that appeared to be referred to the lower left molars and mandible. The patient also had trouble brushing their teeth in the lower left molars due to an increase in sensitivity. The patient had previously seen their dentist at their last visit 3 months ago, but not an endodontist. They had not seen a manual therapist with advanced training in TMDs but had seen a massage therapist with no results. The patient attended our clinic via referral from their dentist as the patient noted “the pain was intensifying!”
Examination revealed limited opening due to pain, full range of motion with assisted opening that was “very” painful, clicking at the left TMJ joint line tenderness, and left sided masseter muscle tenderness upon palpation that referred to the side of their head. With a clinical history of “tooth sensitivity with brushing,” a cursory odontogenic assessment by the chiropractor (OFPT trained) revealed tooth #36 to be severely sensitive to percussion and exquisitely painful to cold testing. In consult with the dentist, it was agreed that a referral to an endodontist was warranted.
The endodontists diagnosis of irreversible symptomatic pulpitis with symptomatic apical periodontitis was made and the patient was treated using root canal therapy of tooth #36. The dentist then provided a crown to cap the tooth. What was minimally presenting without findings as a tooth issue at the previous dentist visit and may have been misleading as a TMD due to confounding symptoms had developed more clinically accurate symptoms. Had the patient not seen a manual therapist with advanced training in TMDs who could provide a cursory dental screen, the patient may have continued to have ongoing pain unnecessarily.
The pain associate with their left TMJ was caused by antalgic movements (movements used to avoid pain) was prescribed simple exercises at home to restore confidence in normal motion and the pain resolved within a couple of weeks.
This case highlights a multi-faceted dental/dentals specialist approach with an advanced trained manual therapist who could review odontogenic issues to avoid prolonged pain for the patient.
Fig. 2

Case study 2: Patient JR
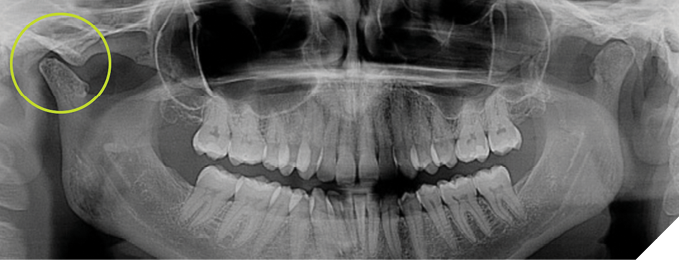
A 25-year-old who identifies as a female presented to our clinic with a 6-month history of bilateral TMJ pain. They had just seen a new dentist due to a relocation for work who reviewed an old panoramic image from 18 months prior. No report was provided. Upon review of the panoramic image, the dentist noted irregularities in the mandibular condyles and made a referral to our clinic. Following review of the images by the Chiropractor (OFPT trained), the dentist was contacted prior to proceeding with a physical exam or the DC-TMD and a CBCT was ordered. An image from almost 10 years previously was attached to the most current CBCT as the patient coincidentally had the CBCT taken with the same imaging group. The imaging was consistent with Juvenile Idiopathic Arthritis (JIA) of the mandibular condyles bilaterally but had not progressed. A referral was made to an oral surgeon by a family member, not in Canada, who had recommended bilateral total joint replacement of the TMJs. A second opinion was requested from a major oral surgery centre in Toronto and a recommendation to return and try conservative care first was presented.
The DC-TMD and a more advanced OFPT examination showed no findings for joint pain and only muscular pain and weakness. The muscular pain was very familiar to their ongoing jaw pain. The patient was diagnosed with a TMD – bilateral primary muscle of mastication myofascial pain with asymptomatic JIA.
A conservative build from passive to active therapies consistent with activities of daily living were applied over a reasonable timespan. A progressive loading model was used. These therapies predated the PEACE & LOVE model and rapid recommendations seen in the BMJ article in 2023, however were extremely consistent JIA rehabilitation of the hip. Cognitive behavioural therapy was successful to help the patient manage the challenges of their pain during the rehabilitation process and encourage them to trust that the pain would resolve with a return to normal function.
This case was approximately 6 years ago, and the patient returns for infrequent follow up and continues to be pain free.
This case highlights that although we may see condylar remodeling, we must assess and determine if the source of the pain is from what presents on images or physical exam. It also highlights the need for a multi-faceted dental/dental professional approach as it involved a general dentist, oral surgeon, dental radiologist as well as an advanced trained manual therapist and cognitive behavioural therapist. This helped avoid invasive surgeries and guide our rehabilitation treatment strategy.
Fig. 3
The ‘TMD’ dental professional check list
By following the steps outlined below, the dental professional can begin the process of finding the best treatment pathway for patients that present with jaw and facial pain.
Step 1: Rule-out red flags
The first step to any assessment regarding pain should be to rule out red flags. Red flags are signs and symptoms that could relate to serious underlying pathologies that mimic musculoskeletal or odontogenic pain and require immediate referral to medicine.
The following is a list of important questions that should be asked of the patient for red-flag identification:
- Unintentional weight loss
- Night pain that wakes you from sleep
- Night sweats
- Severe fatigue or malaise
- New and severe headaches
- Fever
- Vision or speech changes
- The 3 N’s and 5 D’s (Nystagmus, Nausea, Numbness, Dizziness, Diplopia, Dysarthria, Dysphagia, Drop attacks).
Note this is a quick screen of red flags. As health care practitioners one should be familiar with all red flags. For a more complete list please reference https://www.gponline.com/education/medical-red-flags.
Step 2: Odontogenic
Once red-flags have been ruled-out, your next step as the dental professional should be to determine if the pain is odontogenic in nature by performing a systematic diagnostic protocol.
Common tests to determine odontogenic origins include pulpal and periapical tests to see if the patient’s symptoms can be reproduced:
Pulpal Tests
- Cold (ice stick or Endo Ice)
- Hot (warm gutta percha hot pulp tester tip attached to electric heat carrier)
- Electric Pulp Tester
Periapical Tests
- Percussion Test (tapping)
- Bite Test
- Apical Palpation
- Periodontal Probing
- Sinugrams
Also a thorough examination should be performed looking for the following:
- Presence of decay, fractures, periodontal pockets/sinus tracts
- History of recent dental work or trauma
Remember, when trying to reproduce symptoms with odontogenic testing, we are asking the patient if pain is elicited and if it is a familiar pain to their complaint.
If your dental exam proves inconclusive, and doesn’t elicit familiar pain to the patient, then the origin may be non-odontogenic which may include symptoms coming from a MSK origin.
Step 3: MSK pain
To accurately assess patients presenting with jaw or facial pain we must perform a detailed subjective and objective exam.
The subjective exam includes a detailed health history investigating patient complaints, other health concerns, symptoms, aggravating and alleviating factors, timelines, mechanisms of onset etc. and ruling out red flags.
The exam from the dentist should be consistent with the DC-TMD.
The exam from a manual therapist should involve, but are not limited to:
- The DC-TMD as symptoms may have changed since the referral.
- The requisite core cervical examination required by their professional designation. If no exam is required, and they cannot diagnose they should rethink their role.
- Palpation of the associated musculature.
- Orthopedic testing of the joints.
- Neurologic testing such as cranial nerve screening, myotomes, dermatomes and reflexes.
- Hypermobility testing (Beighton score).
Although the DC-TMD can help the dentist or assessing practitioner determine a diagnosis and source of pain for the patient, a more specific examination is necessary for targeted therapies.
Improving patient access to quality care through OFPT
Patient success is the goal. Identifying skilled practitioners with advanced training in TMD management is often difficult. The OFPT registry was created to bridge this gap, providing dentistry, medicine, allied health and patients with a reliable resource to find qualified practitioners who follow evidence-based, effaceable guideline care and who have committed to advanced training and education in TMDs.
Expanding access to high-quality, TMD care, the OFPT program aims to improve outcomes and reduce the prevalence of chronic pain associated with these disorders.
We know patients in pain will often seek answers from Google or AIs like CHAT GPT. Most often they are wrought with misinformation based on biased and out of date data. A patient in pain will ask anyone, so it is within the norm that they may ask their dentist about jaw or even back pain, ask their chiropractor about their jaw or tooth pain! A collaborative relationship will benefit the patient immensely. In these circumstances, all professions need to understand what questions to ask, what signs to look for, what answers to give and where to find a trusted practitioner best suited for their case.
We aim to ensure whoever the patient first seeks help from can find a practitioner who is trained and best equipped to identify the cause of their pain.
We would like to thank Dr. Gary Glassman for his contributions to this article and resolution with one of the patient cases. Dr. Gary Glassman a renowned endodontist and global educator, has created an hour-long lecture for the OFPT program on “How to rule out Red Flags, Rule out Odontogenic Pain, and Rule in Musculoskeletal Issues”, available to view for free, via the QR code (Fig. 4).
Fig. 4

To benefit you, your practice and the patients who need care in your area consider collaboration with an OFPT certified practitioner and/or consider encouraging a manual therapist to take one of our training courses.
To learn more about TMD management, connect with an OFPT certified practitioner near you, or even create an orofacial pain management clinic in your home town, please contact drchris@theofpt.com or visit us at www.theofpt.com.
Please Note: At this time the OFPT course is available for manual practitioners (chiropractors, RMTs, PTs) throughout North America, outside the inner Greater Toronto Area. If your practice falls between the 403 south west, the 412 north east, up to the 407, please contact us to discuss referral or training options. Ideally, recommending the OFPT advanced TMD training to MSK practitioners that you, the dentist, currently collaborate with is the best solution for improving patient outcomes. The OFPT program reserves the right to refuse entry into any of the training courses offered.
OFPT’s next course is in Toronto, May 23-25, at the Henry Schein HQ. Drchris@theofpt.com for inquiries. 
Oral Health welcomes this original article.
References
- Wieckiewicz, M., Shiau, Y. Y., & Boening, K. (2018). Pain of Temporomandibular Disorders: From Etiology to Management. Pain research & management, 2018, 4517042. https://doi.org/10.1155/2018/4517042
- Renton T. (2020). Tooth-Related Pain or Not?. Headache, 60(1), 235–246. https://doi.org/10.1111/head.13689
- Advancing the nation’s oral health through research and innovation | National Institute of Dental and Craniofacial Research. (n.d.). National Institute of Dental and Cranial Research. https://www.nidcr.nih.gov/
- Dubois B, Esculier J. Soft-tissue injuries simply need PEACE and LOVE. British Journal of Sports Medicine 2020;54:72-73.
- Busse J W, Casassus R, Carrasco-Labra A, Durham J, Mock D, Zakrzewska J M et al. Management of chronic pain associated with temporomandibular disorders: a clinical practice guideline BMJ 2023; 383 :e076227 doi:10.1136/bmj-2023-076227
- Wieckiewicz M, Shiau YY, Boening K. Pain of Temporomandibular Disorders: From Etiology to Management. Pain Res Manag. 2018 Jun 20;2018:4517042. doi: 10.1155/2018/4517042. PMID: 30026884; PMCID: PMC6031157.
- Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, List T, Svensson P, Gonzalez Y, Lobbezoo F, Michelotti A, Brooks SL, Ceusters W, Drangsholt M, Ettlin D, Gaul C, Goldberg LJ, Haythornthwaite JA, Hollender L, Jensen R, John MT, De Laat A, de Leeuw R, Maixner W, van der Meulen M, Murray GM, Nixdorf DR, Palla S, Petersson A, Pionchon P, Smith B, Visscher CM, Zakrzewska J, Dworkin SF; International RDC/TMD Consortium Network, International association for Dental Research; Orofacial Pain Special Interest Group, International Association for the Study of Pain. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J Oral Facial Pain Headache. 2014 Winter;28(1):6-27. doi: 10.11607/jop.1151. PMID: 24482784; PMCID: PMC4478082.
- https://www.nationalacademies.org/our-work/temporomandibular-disorders-tmd-from-research-discoveries-to-clinical-treatment
- Zadro J, O’Keeffe M, Maher C. Do physical therapists follow evidence-based guidelines when managing musculoskeletal conditions? Systematic review. BMJ Open. 2019 Oct 7;9(10):e032329. doi: 10.1136/bmjopen-2019-032329. PMID: 31591090; PMCID: PMC6797428.
- McKinlay JB, Link CL, Freund KM, Marceau LD, O’Donnell AB, Lutfey KL. Sources of variation in physician adherence with clinical guidelines: results from a factorial experiment. J Gen Intern Med. 2007 Mar;22(3):289-96. doi: 10.1007/s11606-006-0075-2. PMID: 17356957; PMCID: PMC1824760.
About the authors

Sid Lisser is the co-CEO of OFPT Certification and Lead Jaw Clinician at The Jaw & Facial Pain Centre. He is currently an associate in dentistry at the University of Toronto School of Dentistry, associate scientific staff at the Mount Sinai Hospital Department of Dentistry, Facial Pain Clinic and oversees externs from the Canadian Memorial Chiropractic College Externship Program.

Dr. Chris Oswald is a chiropractor of 36 years, entrepreneur, and speaker. He owns and operates a multi-disciplinary clinic in Canada, The Centre for Fitness, Health, and Performance, and he’s the co-founder of The Jaw & Facial Pain Centre.

Colby Bucci, MScPT, received his Master’s degree in Physical Therapy at the University of Toronto. He holds advanced training certifications in orofacial pain management, vestibular rehabilitation, acupuncture, and osteoporosis care through BoneFit Canada. Colby is the co-owner of The Centre for Fitness Health and Performance and The Jaw & Facial Pain Centre.