
Imagine your patient walking into your office for a routine check-up, expecting the usual dental/perio conversation, only to leave with a referral to a specialist that could save his or her life. Thanks to artificial intelligence (AI), this is not science fiction—it is the future of dentistry.
The integration of AI is revolutionizing the screening workflow in dentistry, transforming how dentists approach detection, documentation, claim processing, and patient communication. AI currently excels at identifying common tooth-related pathologies, such as caries, bone loss, apical lesions, restorations, and the position of the mandibular nerve, serving as a powerful tool for both clinical practice and patient engagement. Beyond its role as a diagnostic aid, AI has emerged as an effective communication and marketing tool, enhancing patient trust and understanding. However, the true frontier for AI lies in detecting “outliers”—rare or subtle pathologies that often go unrecognized due to their deviation from routine findings.
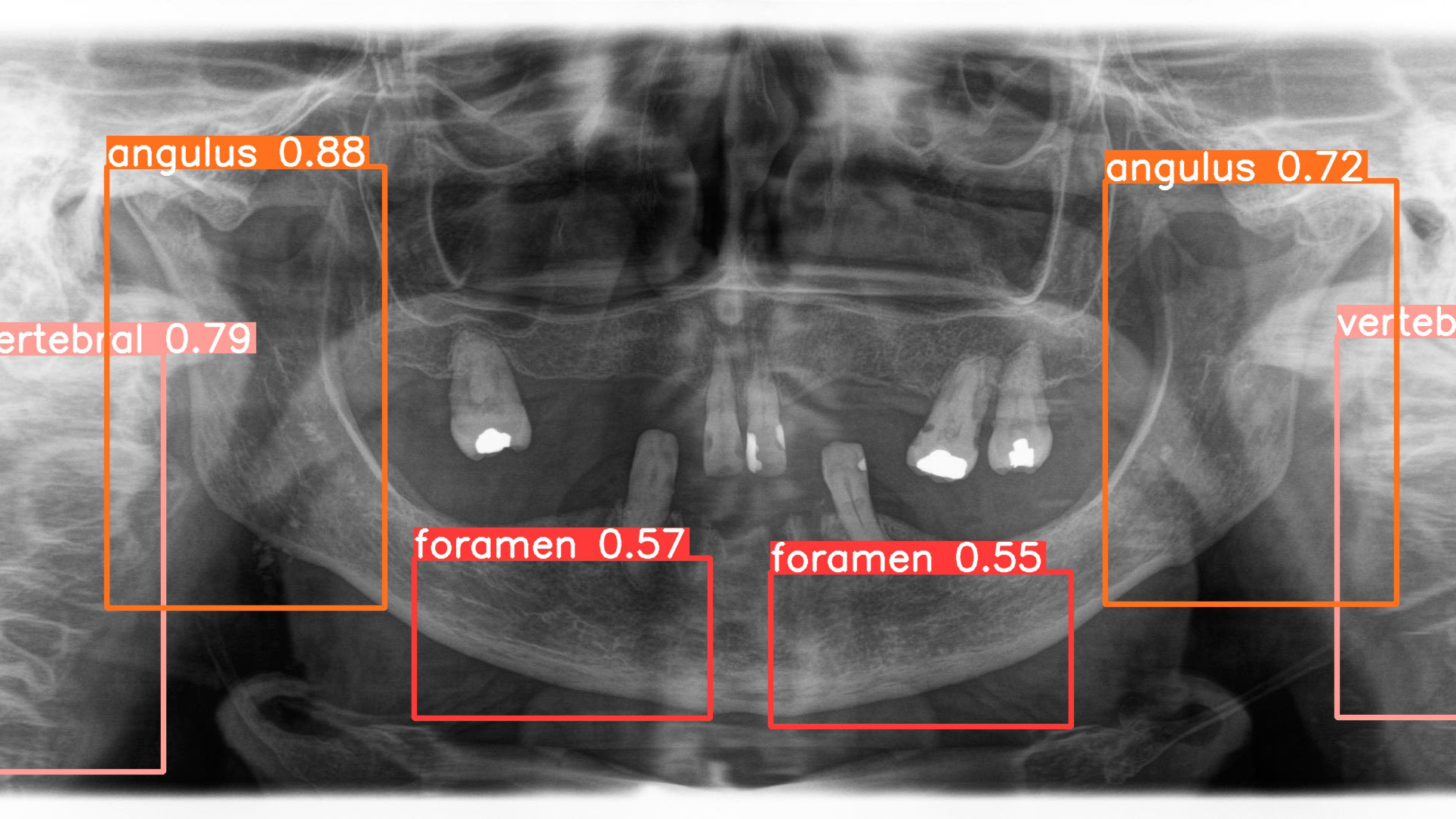
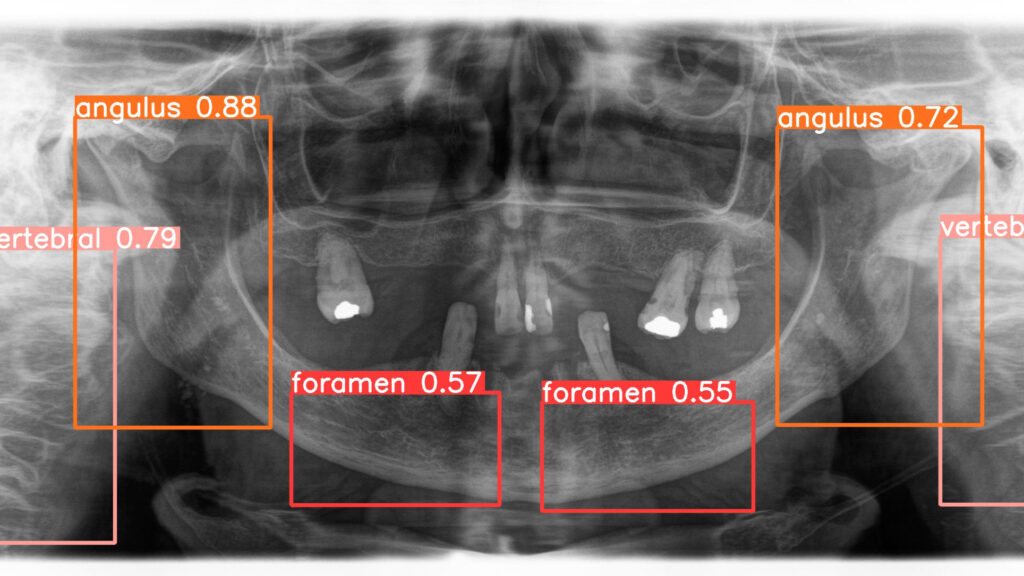
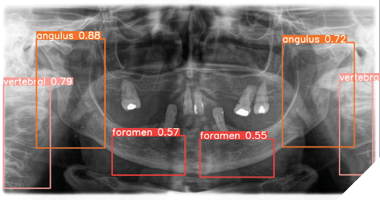
Panoramic radiographs, a cornerstone of dental diagnostics, are widely used by dentists and oral and maxillofacial (OMF) surgeons in routine clinical practice. While radiologists may occasionally interpret these images, OMF surgeons frequently analyze their own panoramic radiographs. Research highlights that a clinician’s training significantly influences the accuracy of radiographic interpretation. In dentistry, diagnostic performance varies due to differences in individual knowledge, skills, and biases, leading to inconsistencies in assessing radiographic images. This variability can result in misdiagnosis or mistreatment, with studies indicating that misdiagnosis rates for caries depth in conventional radiographs can reach 40%, and 20% of teeth may be incorrectly identified as diseased. These challenges underscore the potential for AI to enhance diagnostic precision and reduce errors in dental practice (Fig. 1).
Fig. 1

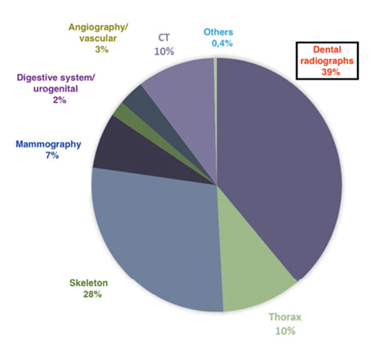
Dentistry has always been about more than just teeth, but AI is taking it to a whole new level. Routine dental visits, often more frequent than medical check-ups, offer a unique opportunity to screen for systemic diseases (Fig. 2). Panoramic radiograph (PR), a standard imaging modality for dental diagnostics, captures a detailed view of the jaw, teeth, and surrounding structures, making it ideal for spotting abnormalities beyond cavities and crowns. Yet, dentists often lack specialized training to recognize signs of conditions like carotid artery calcification (CAC) or osteoporosis, leading to missed opportunities. AI steps in where human expertise falls short, automating the detection of these “outlier” pathologies with remarkable accuracy. By doing so, it empowers dentists to act as first responders in healthcare, flagging risks and referring patients to specialists before symptoms escalate.
Fig. 2
Atherosclerosis, the silent buildup of plaque in arteries, is a major driver of cardiovascular diseases, including stroke. Carotid artery calcification, a telltale sign of atherosclerosis, shows up in 3-15% of PR, with 7% of cases indicating severe stenosis—narrowing of the artery by over 50%. This is a red flag for stroke, which affects millions yearly, causing disability, diminished quality of life, and billions in healthcare costs. Unfortunately, most dentists aren’t trained to spot CAC on PR, meaning these warning signs often go unnoticed, delaying life-saving interventions.
Osteoporosis, another silent disease, affects about 60% of women over 50, weakening the bone structure and increasing fracture risk. The gold standard for diagnosis, Dual-Energy X-ray Absorptiometry (DXA), is typically used after a fracture, missing the chance for early prevention. PR can reveal osteoporotic changes, like thinning mandibular bone, but existing indices that must be manually calculated, like the Klemetti Index, are time-consuming and prone to errors.
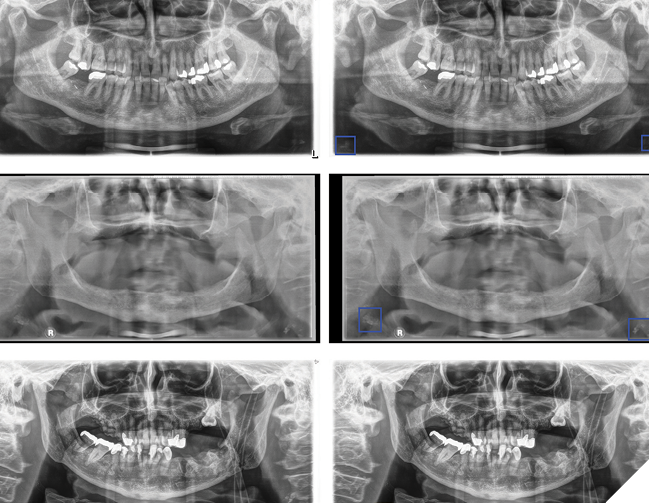
The Department of Oral and Maxillofacial Surgery at the Charité Berlin developed a deep learning model to detect CAC on PR (Fig. 3). Using a detection/segmentation model, researchers analyzed 6,404 PR from 5,621 patients, ranging in age from 18 to 99. They focused on 185 PR with confirmed CAC, matched with an equal number without, all meticulously annotated by three experienced clinicians. The dataset was enhanced with techniques like horizontal flipping, and images were normalized for consistency. The model was carefully tested in multiple rounds. It correctly identified about 90% of cases, missed very few, and achieved overall accuracy that shows it works reliably and is promising for real use. Dentists using it can confidently identify CAC during routine check-ups, acting as gatekeepers who refer patients to vascular specialists for further tests like Doppler ultrasound.
Fig. 3
On the osteoporosis front, a collaboration between Charité Berlin and Danube Private University developed an AI classifier to spot signs of the disease in PR (Fig. 4). We used a dataset of patient images divided into training (348 patients/radiographs), validation (58 patients/radiographs), and testing groups (51 patients/radiographs), with bone health confirmed by scans and their DXA scores. A DXA score (or T-score) is a measurement from a bone density scan that compares a person’s bone strength to that of a healthy young adult. Our two-step model first located areas of interest, then classified them. It detected osteoporosis with 83% sensitivity. Although overall accuracy was modest, the model prioritized finding true cases—important for early screening. This tool empowers dentists to flag osteoporosis during routine visits, referring patients to specialists for DXA scans and treatments like bisphosphonates. For women over 50, this early detection can prevent fractures, saving lives and healthcare costs.
Fig. 4
But challenges remain. In general AI studies with single-center data and single imaging devices raise generalizability concerns. Multi-center studies, more data and broader equipment testing are needed, along with prospective trials to confirm real-world benefits. Factors like age and gender, which can skew results, also need addressing. Ethical concerns—patient consent, data privacy, and avoiding over-reliance on AI—require careful handling. Dentists need training to interpret AI results critically, and clear patient communication is vital to maintain trust. Integrating these tools into practice means tackling logistical hurdles like system compatibility and staff training, which calls for teamwork between AI developers and dental professionals. Despite hurdles, these tools promise better patient outcomes, lower healthcare costs, and a bold new role for dentistry as a cornerstone of preventive care, ensuring no health risk slips through the cracks.
AI is redefining dentists as gatekeepers, turning routine check-ups into health checkpoints. Dental visits, often annual, offer unmatched screening opportunities compared to sporadic medical visits. By catching diseases like CAC and osteoporosis early, dentists can refer patients to specialists, preventing strokes and fractures that burden healthcare systems with billions in costs. AI’s automated, accurate PR analysis overcomes training gaps, reducing missed diagnoses and malpractice risks.
Looking ahead, AI could spot other conditions on dental imaging modalities, like diabetes or cancers on x-rays, records and intraoral pictures, further expanding dentists’ roles. Combining these image modalities could boost accuracy, while prospective studies will validate real-world impacts. Open-source AI development, sharing data and models, could democratize these tools, making them accessible to all dental practices. 
Oral Health welcomes this original article.
About the authors

Robert Gaudin, MD, DMD, Professor Gaudin is a maxillofacial surgeon and AI pioneer in dentistry. He has founded dental AI companies VideaHealth (Harvard, MIT) and DentalXrai (Charité Berlin). His research focuses on AI-driven early detection. He works at the SailerClinic in Zurich and as a researcher at Charité Berlin and the University for Digital Technologies in Medicine and Dentistry.

Martin Lanzer, MD, DMD, PHD, Doctor Lanzer is a maxillofacial surgeon and a lecturer at the University of Zurich, where he has worked as a surgeon. He holds an eMBA from IMD Lausanne. Since 2024, he has served as Clinic Director and CEO of SailerClinic in Zurich.

Iman Ghanad, MD, Doctor Iman Ghanad earned his medical degree from Charité University Berlin. He completed a Research Fellowship at Mass Eye and Ear, Harvard Medical School (2016–2018). He began residency training in Plastic Surgery at BG Klinik Ludwigshafen and now pursues Oral and Maxillofacial Surgery at Charité Berlin, focusing on 3D printing and medical AI.