
Founded by Dr. Dirk Duddeck, a German dentist and biologist, the CleanImplant Foundation emerged from his research into unexplained implant failures and his concern over manufacturing quality inconsistencies. Officially established in 2016 as a non-profit, charitable entity, the Foundation was built on Dr. Duddeck’s pioneering work, which he performed in collaboration with the University of Cologne and the Charité University in Berlin, Germany. His vision was to create complete transparency in implant manufacturing through objective, scientifically rigorous testing entirely free from industry influence, driven by the fundamental belief that patients deserve to know what is being placed in their bodies.
The Foundation’s mission is executed through a rigorous scientific methodology, utilizing scanning electron microscopy (SEM) and energy-dispersive X-ray spectroscopy (EDS) conducted under cleanroom conditions in specialized testing laboratories that are officially accredited according to international standards (ILAC MRA). The elaborate process of analysis identifies harmful foreign metallic particles and carbonaceous contaminants that are invisible to the naked eye. Their work has led to the prestigious Trusted Quality Seal, a certification awarded to implant systems that meet stringent cleanliness standards and possess robust clinical documentation. Members of the Foundation’s global network receive detailed, bi-annual updates from these ongoing studies, which indicate which implant systems demonstrate and continue to meet the highest benchmarks. This commitment to continuous monitoring helps clinicians make evidence-based choices for their patients.
Under Dr. Duddeck’s leadership, the CleanImplant Foundation has evolved into a globally recognized authority, boasting an international Scientific Advisory Board and ambassadors in over 20 countries. Its impact has been significant, raising industry standards, influencing manufacturing practices, and creating a network of Certified CleanImplant Dentists worldwide. For its contributions to sustainable healthcare and patient safety, the Foundation was recognized with a Global Sustainable Excellence Award in 2025, cementing its role as a transformative force advocating for higher quality and transparency in implant dentistry.
Compromised osseointegration and peri-implantitis
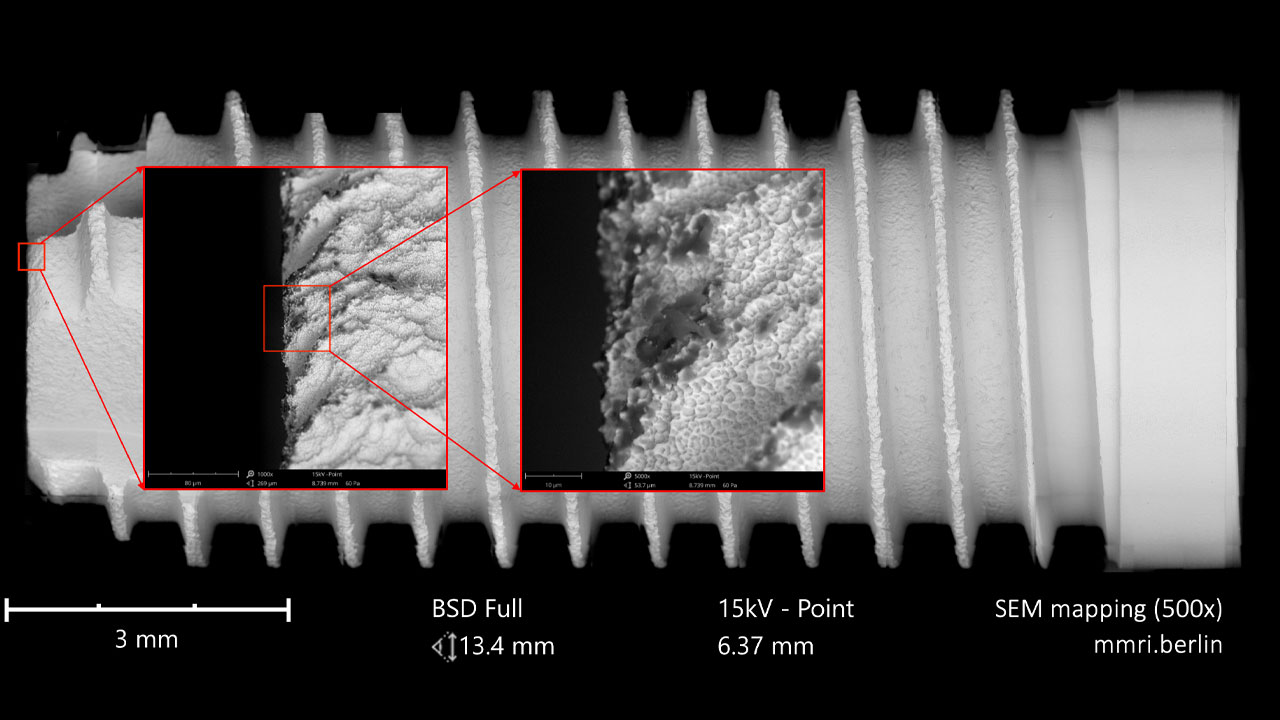
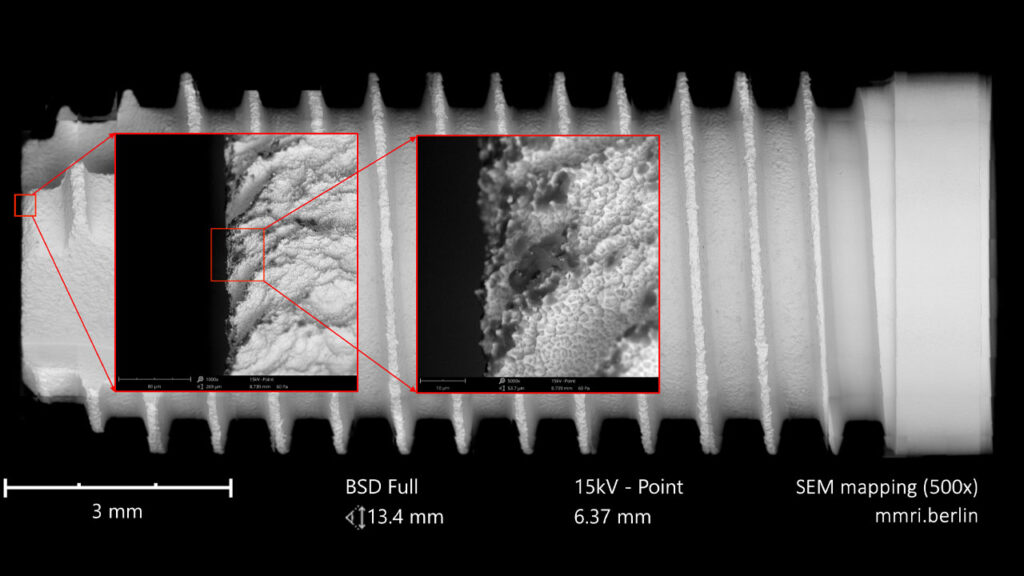
Peri-implantitis represents a significant challenge in modern dentistry, threatening the long-term success of dental implants and patient oral health (Fig. 1). This inflammatory condition, affecting tissues surrounding dental implants, leads to progressive bone loss and eventual implant failure if left untreated. Systematic reviews indicate an alarming overall prevalence of 19.53% at the patient level and 12.53% at the implant level, highlighting the scale of this clinical challenge.1 While multiple risk factors contribute to peri-implantitis, including poor oral hygiene, smoking, and history of periodontitis, emerging research has identified implant surface contamination as a critical yet preventable contributor to these complications. The clinical relevance of this factor was substantiated in various quality assessment studies over the past 10 years analyzing hundreds of commercially available implants.2-5 On average, one in four tested implants showed significant impurities with more than 50 plastic particles, most of them small enough for phagocytosis by immune cells (Figs. 2-12).
Fig. 1

Fig. 2
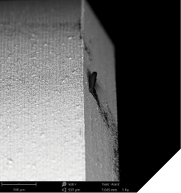
Fig. 3
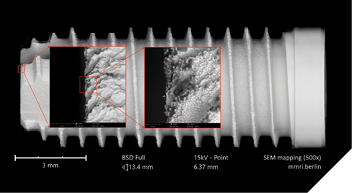
Fig. 4
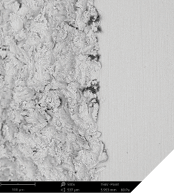
Fig. 5

Fig. 6
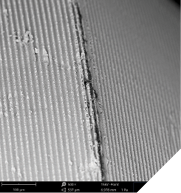
Fig. 7
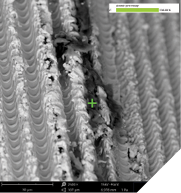
Fig. 8
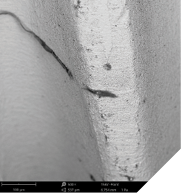
Fig. 9
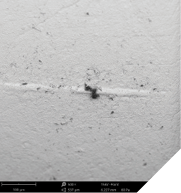
Fig. 10
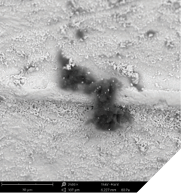
Fig. 11

Fig. 12

The presence of manufacturing residues—invisible to the naked eye but quantifiable through advanced microscopy—creates biological environments that fundamentally compromise osseointegration and predispose implants to inflammatory reactions.6 These contaminants, such as plastic particles, fluorocarbons, remnants of cell-toxic surfactants, hydrocarbon lubricants, and silicone residues, trigger complex immune responses that can lead to early implant failure.7-9 Understanding the triad between industry responsibilities in producing clean implants, the ethical obligations of dental professionals, and patient expectations of safety and efficacy is crucial for addressing this preventable cause of peri-implantitis.
Industry responsibilities: The manufacturing imperative
The dental implant industry bears significant responsibility for addressing the challenge of surface contamination, as it may originate from various stages of the manufacturing process—such as machining, cleaning, handling, and final packaging. Particles of tungsten may remain from machining tools; thin-film layers of cleaning agents such as hazardous dodecylbenzene sulfonic acid (DBSA), chemically identified in the testing laboratories, show an insufficient washing process, and plastic particles remain from handling or packaging materials. The presence of these substances, which can technically be avoided, reflects inadequate quality control measures during production and packaging processes.
Ethical implications of manufacturing choices
The identification of significant contaminants on sterile-packaged implants, which are ready to use for patients, raises serious ethical concerns regarding product safety and transparency. Manufacturers have a moral and professional obligation to ensure that their products do not harm patients, which includes minimizing potential triggers for inflammatory responses. This obligation extends beyond mere regulatory compliance to embrace the precautionary principle, actively working to eliminate potential hazards even when absolute proof of harm may not yet be established.
The economic pressures to produce less expensive implants should not compromise fundamental quality standards. When manufacturers prioritize cost reduction over impeccable surface cleanliness, they potentially contribute to future patient harm and additional healthcare costs associated with treating peri-implantitis. This represents a false economy that transfers costs from the manufacturer to the clinician and patient through increased failure rates and complication management.
Bioethical principles in implant dentistry
The ethical framework for addressing implant contamination issues rests on four fundamental bioethical principles: beneficence (acting in the patient’s best interest), non-maleficence (avoiding harm), autonomy (respecting patient decision-making), and justice (ensuring fair distribution of benefits and risks).
In the context of implant surface quality, beneficence requires clinicians to select implants with the highest probability of long-term success based on scientific evidence rather than cost or convenience. Non-maleficence imposes an obligation to avoid implants with known contaminants that might trigger inflammatory responses. Autonomy necessitates fully informing patients about implant choices, including potential risks associated with different systems. Justice requires consideration of how implant selection affects broader healthcare costs and outcomes across patient populations.
Informed consent and shared decision-making
The ethical concept of informed consent extends beyond mere legal formalism to represent a fundamental aspect of respectful patient care. Patients considering implant therapy should be informed about the importance of surface quality and how it might affect their long-term outcomes.
Unfortunately, current informed consent processes often neglect technical aspects of implant selection, focusing primarily on surgical risks and benefits. A more comprehensive approach would include a discussion of implant characteristics and quality evidence, empowering patients to participate meaningfully in device selection based on long-term success rather than short-term considerations.
The foundation of trust in dental care
Trust represents a fundamental component of the patient-clinician relationship, particularly in elective procedures like implant dentistry. Patients rightly expect that the devices permanently placed in their bodies have been manufactured to the highest standards of safety and efficacy. When implants contain preventable contaminants that contribute to inflammatory responses, this trust is violated.
The psychological impact of implant failure extends beyond physical discomfort to include diminished trust in dental professionals and reluctance to pursue necessary tooth replacement options. Patients who experience peri-implantitis often report feelings of betrayal, particularly when they discover that their complications might have been prevented through different implant selection or more thorough informed consent processes.
Economic and quality of life implications
Peri-implantitis significantly reduces patients’ quality of life by inducing pain, discomfort, functional limitations, and psychological distress. A Swedish study with an average follow-up of 8.2 years found that peri-implantitis increased treatment costs by approximately 1,500 CDN for patients with single-tooth restorations and 2,000 CDN for those with full-arch restorations.10 These economic impacts, combined with the physical and psychological burden of treatment, highlight the importance of preventing rather than managing peri-implantitis.
Scientific validation through rigorous testing
The CleanImplant Foundation has established a scientifically rigorous protocol to address the challenge of implant surface contamination. The Foundation’s methodology involves examining sterile-packaged implants under controlled cleanroom conditions to prevent external contamination during analysis. Scanning electron microscopy (SEM) coupled with energy-dispersive X-ray spectroscopy (EDS) can precisely identify and quantify both organic and inorganic residues on implant surfaces. Elemental mapping distinguishes intrinsic titanium or zirconia from extrinsic contaminants, including carbonaceous residues and foreign metals like iron-chromium compounds or tungsten. This analytical framework is performed exclusively in officially accredited testing laboratories according to ILAC MRA / DIN EN ISO/IEC 17025 standards, ensuring consistent and reliable results across evaluations. This systematic approach enables an objective comparison of implant surface cleanliness across different manufacturers and product lines.
Shifting from treatment to prevention
Significant impurities associated with implant manufacturing processes, which have been identified on far too many different implant systems, may constitute an undervalued factor contributing to an early onset of peri-implantitis.11 The recognition of implant surface contamination as a modifiable risk factor for peri-implantitis represents a paradigm shift in implant success strategies. Traditional approaches have focused primarily on surgical precision, prosthetic design, and patient maintenance, whereas contemporary understanding recognizes that microscopic surface properties determine biological acceptance and long-term stability.
This preventive approach is particularly important for patients with systemic health considerations like diabetes or osteoporosis, conditions that already impair bone metabolism and healing capacity. For these vulnerable populations, eliminating contamination-related inflammation becomes even more critical for achieving successful outcomes.
Economic rationale for quality investment
The cumulative cost of managing peri-implantitis complications—both financial and biological—makes prevention through verified surface quality a rational clinical priority. Complex regenerative surgeries required to address advanced peri-implantitis often involve significant practice burden, unpredictable outcomes, and substantial patient expenses. Investing in verified clean implants represents a cost-effective strategy for reducing these downstream complications and their associated burdens.
Toward an integrated ecosystem of trust and quality
The understanding of immune responses to implant surface contaminants has created an opportunity to fundamentally improve implant success rates through science-driven quality assurance. Yet the CleanImplant initiative extends beyond laboratory testing. It represents a complete ecosystem of collaboration, education, and patient-centered communication.
It is a systemic approach. Beginning with industry collaboration in manufacturing and packaging, extending through clinical treatment and long-term maintenance as part of the “Approved by” CleanImplant recommendation, and reinforced by certification and post-market surveillance, the Foundation provides a continuous cycle of improvement. Within this cycle, certified dentists and clinics act as ambassadors of quality, while structured patient communication ensures that transparency and trust remain central to care.
By linking rigorous testing and validation with professional certification, industry responsibility, and patient empowerment, CleanImplant transforms implant dentistry from a series of isolated choices into a sustainable, interconnected ecosystem. This model elevates surface quality verification from a niche concern to a new standard of care, where prevention, accountability, and ethical responsibility converge.
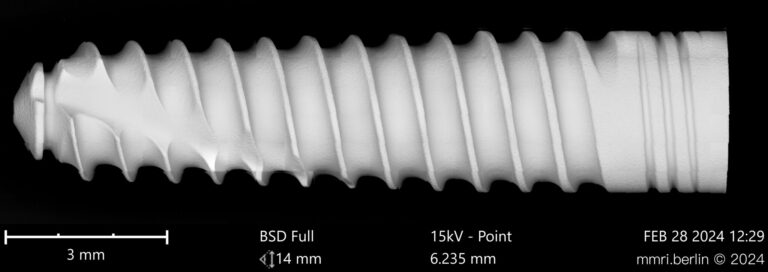
For clinicians committed to predictable outcomes and ethical practice, engagement with the CleanImplant Foundation means more than selecting cleaner implants (Fig. 13). It means participating in a global movement that integrates science, practice, industry, and patient trust into one coherent framework. This is how implant dentistry can truly shift from reactive treatment toward proactive prevention, ensuring safer, longer-lasting outcomes for patients worldwide.
Fig. 13
Proven clean implant systems that have been awarded after thorough testing with the “Trusted Quality” seal can be found on the Foundation’s website (www.cleanimplant.org). 
Oral Health welcomes this original article.
Images and Captions: All implants shown in this article have FDA clearance and are produced or distributed in North America).
References
- Diaz P, Gonzalo E, Villagra LJG, Miegimolle B, Suarez MJ. What is the prevalence of peri-implantitis? A systematic review and meta-analysis. BMC Oral Health. Oct 19 2022;22(1):449. doi:10.1186/s12903-022-02493-8
- Duddeck DU, Albrektsson T, Wennerberg A, Larsson C, Beuer F. On the Cleanliness of Different Oral Implant Systems: A Pilot Study. J Clin Med. Aug 22 2019;8(9)doi:10.3390/jcm8091280
- Duddeck DU, Albrektsson T, Wennerberg A, Larsson C, Mouhyi J, Beuer F. Quality Assessment of Five Randomly Chosen Ceramic Oral Implant Systems: Cleanliness, Surface Topography, and Clinical Documentation. Int J Oral Maxillofac Implants. Sep–Oct 2021;36(5):863–874. doi:10.11607/jomi.8837
- Duddeck DU, Iranpour S, Neugebauer J, Zoeller JE. Surface characteristics and quality of implants in sterile packaging – SEM examination and qualitative/quantitative elemental analysis of 57 implants. EDI journal. 2013;9(2013-1):48–58.
- Duddeck DU, Maghaireh H, Faber FJ, Neugebauer J. SEM Surface Analyses of 120 Sterile-packed Implants. EDI journal. 2015;11(2015-2):64–75.
- Alves CH, Russi KL, Rocha NC, et al. Host-microbiome interactions regarding peri-implantitis and dental implant loss. J Transl Med. Sep 23 2022;20(1):425. doi:10.1186/s12967-022-03636-9
- Matthews JB, Besong AA, Green TR, et al. Evaluation of the response of primary human peripheral blood mononuclear phagocytes to challenge with in vitro generated clinically relevant UHMWPE particles of known size and dose. J Biomed Mater Res. Nov 2000;52(2):296–307. doi:10.1002/1097-4636(200011)52:2<296::aid-jbm8>3.0.co;2-9
- Rader CP, Sterner T, Jakob F, Schutze N, Eulert J. Cytokine response of human macrophage-like cells after contact with polyethylene and pure titanium particles. J Arthroplasty. Oct 1999;14(7):840–8. doi:10.1016/s0883-5403(99)90035-9
- Wedemeyer C, Neuerburg C, Pfeiffer A, et al. Polyethylene particle-induced bone resorption in substance P-deficient mice. Calcif Tissue Int. Apr 2007;80(4):268–74. doi:10.1007/s00223-007-9005-5
- Karlsson K, Derks J, Wennstrom JL, Petzold M, Berglundh T. Health economic aspects of implant-supported restorative therapy. Clin Oral Implants Res. Feb 2022;33(2):221–230. doi:10.1111/clr.13885
- Ganz SD, Duddeck DU, Kurtzman GM. Peri-implantitis and the Effect of the Implant Surface at Placement. Compend Contin Educ Dent. Jan 2023;44(1):52–55.
About the authors

Kenneth S. Serota, DDS, MMSc graduated from the University of Toronto Faculty of Dentistry in 1973 and received his Certificate in Endodontics and Master of Medical Sciences degree from the Harvard-Forsyth Dental Center in Boston, Massachusetts in 1981. Dr. Serota is the Canadian ambassador of the Digital Dentistry Society, the North American representative of the CleanImplant Foundation, and on the board of the Build Your Smile Dental Foundation.

Dr. Dana Adyani Fard completed her dental degree and licensure at the University Frankfurt am Main/Germany in 2006 and earned her doctorate in periodontology in 2012. In addition to her work in clinical research consulting for medical devices, she is the founder and patent holder of an oral health product. Now based in Los Angeles, CA, she serves as an Executive Advisor at the CleanImplant Foundation.