


Full arch implant-supported fixed protheses have become a highly desired solution for the rehabilitation of patients with terminal dentition or completely edentulous arches. New developments in digital dentistry have enabled practitioners to extract vital information from intraoral scans and cone beam computed tomography (CBCT) to plan and execute fully guided implant placement that is prosthetically driven. Preoperative implant planning using a digital workflow can significantly improve the predictability and success of implant-supported restorations, lessening the burden on the surgeon and restorative dentist during the time of surgery.
When designing a full arch implant-supported prosthesis, optimal implant positioning is not only determined by the available bone structure but also by the prosthetic design which accounts for occlusion, aesthetics, and soft tissue anatomy.1 Planning begins with data acquisition and may include the following: extraoral and intraoral digital photos, intraoral scans, facial scans and CBCT imaging. This information is used to formulate a facially-driven treatment plan that accounts for ideal incisal edge position, lip dynamics and patient preferences.2 The STL file from the intraoral scan and the DICOM data from the CBCT can be superimposed in an implant planning software to design a surgical guide and provisional prosthesis, which can be fabricated using additive or subtractive manufacturing. It is imperative that the surgical guide is stabilized to prevent any movement during surgery, and oftentimes fixation pins are incorporated into the design to attain the highest level of surgical accuracy.3 Once the implants are placed and primary stability is confirmed, the pre-fabricated provisional prosthesis can be picked up intraorally with resin and finalized extraorally while the sutures are placed. This offers the patient immediate aesthetics and function, improving their overall experience.
Achieving passive fit is a key factor in the success of implant-supported fixed dental prostheses. Misfit can lead to both mechanical and biological complications such as screw loosening, component fracture and bone loss.4 During impressions, it is crucial to accurately transfer the implant positions to the model to ensure a passive fit.5 While a fully digital pre-surgical work-up is advantageous to both patients and clinicians, the final step of the full-arch treatment (ie. the definitive prosthesis) has faced challenges with a digital workflow. Intraoral scanners (IOSs) have shown clinically acceptable accuracy compared to conventional impressions for single crowns and short span fixed dental prostheses.6 However, conventional impressions are more accurate for full-arch implant-supported restorations than IOS technology.7,8 While the technology continues to evolve and more recent literature has shown comparable results between the two impression modalities, it may still be wise to exercise caution when digitally capturing full-arch implant impressions as the accuracy greatly depends on the scanning strategy and many studies have been inconclusive.9
This case report demonstrates a hybrid digital-analog workflow for the design and fabrication of a full-arch fixed implant-supported maxillary prosthesis. By combining technological advances in digital dentistry for planning a predictable surgery and provisional prosthesis with the gold standard conventional impression technique for fabricating the definitive prosthesis, the patient experiences the best of both worlds in their care and treatment outcome.
Case Report
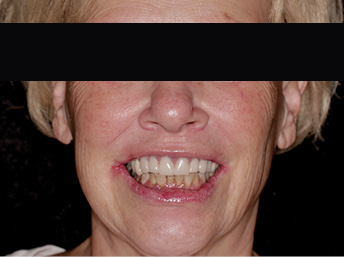
A 65-year-old female presented with maxillary terminal dentition seeking a fixed solution to replace her missing and failing teeth (Figs. 1A &B). Her maxillary arch was previously rehabilitated with a combination of crowns and bridges 20 years ago, most of which were extracted within the last two years due to recurrent caries. A maxillary partial acrylic denture was fabricated at the time to replace the extracted teeth; however, she was never happy with this prosthesis and used it in social situations only.
Fig. 1A

Fig. 1B
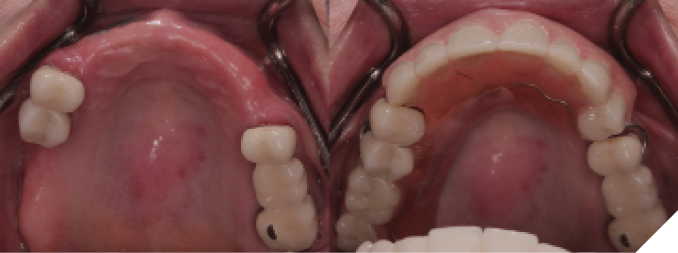
She presented with only four remaining maxillary teeth, two of which had large recurrent caries and were deemed unrestorable. Although heavily restored, her natural mandibular dentition was still intact with recurrent caries on all anterior teeth. After discussing both removable and fixed options, the patient decided to proceed with extraction of the remaining maxillary teeth and placement of six implants to support a fixed full-arch prosthesis. The recurrent caries on the mandibular teeth would be restored with direct composite resin restorations before injection moulding to level out the mandibular occlusal plane (Fig. 2).
Fig. 2

After comprehensive examination, periodontal assessment and scaling and root planning, an initial smile design was performed using full facial photos to determine the ideal incisal edge position. Both arches were scanned with an intraoral scanner (TRIOS 3, 3Shape A/S, Copenhagen, Denmark) for a digital wax-up based on the preliminary smile design. This data was merged with a facial scan to generate a facially-driven treatment plan. An intraoral mock-up was performed using a 3D-printed prototype of the digital wax-up to assess aesthetics and upper lip support without a flange (Fig. 3). Due to excessive lip mobility and a high smile line, the plan was to fabricate an FP1 prosthesis (with no pink in the design) (Fig. 4). Since the transition line could not be hidden without substantial bone removal, the patient accepted a prosthetic design with long teeth. Once the design was approved, fiducial markers were placed on the prototype and scanned intraorally. This was followed by a CBCT scan. The resulting STL and DICOM files were merged in an implant planning software (co-Diagnostix, Dental Wings GmbH, Dusseldorf, Germany) for restoratively-driven implant planning. This was used to produce a fixation pin guide, pin-retained surgical guide and pin-retained temporary prosthesis with access channels for pick-up (Fig. 5).
Fig. 3

Fig. 4

Fig. 5

When planning a full arch case, we have the challenge of determining where the most ideal implant locations would be. It is important to balance the anterior-posterior (AP) spread with the anatomical limitations that the patient presents with. While the published success rates in general appear to be very similar between tilted implants and straight implants in terms of failure rate or marginal bone loss levels over 3 years in function10, their placement is much more technique sensitive.11 It is important to maintain symmetry of implant placement for equal stress on the implants, and to manage the cantilevers. In this case it was determined that after osseous reduction there would be no or minimal native bone remaining around the distal implants. AP spread should be determined by bone quality, number and distribution of implants, rehabilitation design, and prosthesis material12 and in this case extending to the first molars was deemed appropriate.
At the time of implant surgery, the tooth-supported fixation pin guide was tried-in and full seating confirmed through the windows incorporated into the design (Fig. 6). After the four fixation pins were inserted, the remaining maxillary teeth were extracted and a full mucoperiosteal flap was raised prior to placing the pin-retained surgical guide (Fig. 7). Implants were placed at sites #15, 13, 11, 21, 23, and 25 (Straumann Roxolid BLT, Straumann, Basel, Switzerland), with angled placement at 15 and 25 to avoid sinus grafting (Fig 8). Primary stability was confirmed at all sites except 23, which was treated as a 2-stage surgery and left out of the provisional prosthesis. Angled multi-unit abutments (SRA, Straumann, Basel, Switzerland) were attached to the five stable implants, followed by insertion of temporary cylinders in preparation for pick-up (Fig. 9). The provisional prosthesis was then placed using fixation pins, and subsequently attached to the temporary cylinders with flowable composite resin (Fig. 10). Minor occlusal adjustments were made before removal of the provisional prosthesis for finishing and polishing while the surgical sites were sutured (Fig. 11). The provisional prosthesis was re-inserted and post-op instructions were given (Fig. 12).
Fig. 6
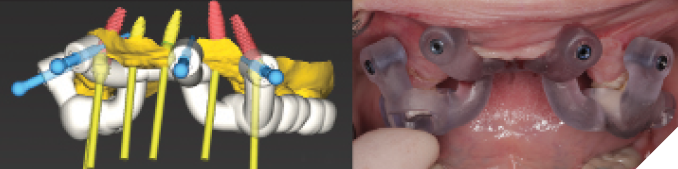
Fig. 7
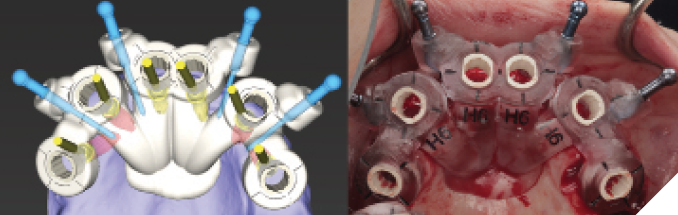
Fig. 8
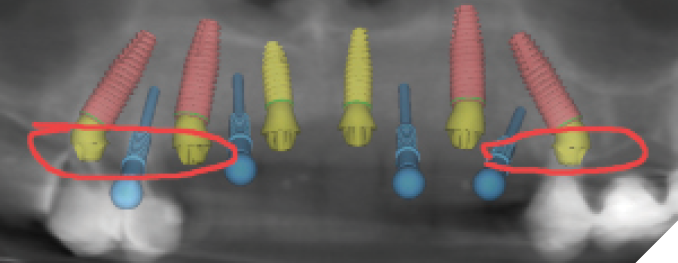
Fig. 9

Fig. 10
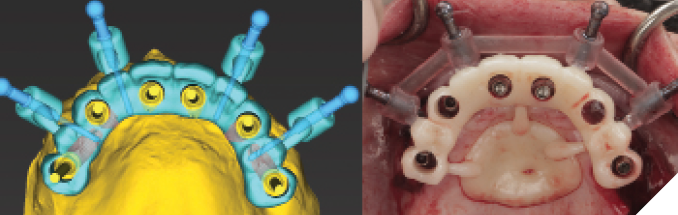
Fig. 11

Fig. 12

After four months of healing, osseointegration was confirmed and 2nd stage surgery was performed at site #23. A preliminary closed-tray impression was taken with polyvinylsiloxane (PVS) for the fabrication of a custom open tray. The final impression was captured using an open-tray technique with splinted impression copings (Fig. 13). A verification jig was designed and 3D-printed from the scanned master cast, and reluted intraorally with Triad gel (Fig. 14). Passive fit on the master cast was confirmed with a one-screw test. A new prototype with a hybrid FP1/FP3 design was milled from polymethylmethacrylate (PMMA) to assess if a more pleasing aesthetic result could be achieved, knowing that the pink transition line may be visible in the anterior (Fig. 15). The patient preferred the new design since the anterior teeth were more proportionate and the gingival shade blended well with her natural tissue (Fig. 16). The definitive prosthesis was milled from monolithic zirconia and a maxillary nightguard was provided at the final insertion appointment (Fig. 17, 18).
Fig. 13
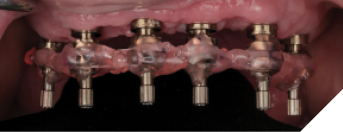
Fig. 14

Fig. 15

Fig. 16

Fig. 17


Fig. 18A



Fig. 18B

Discussion
The hybrid digital-analog workflow presented in this paper displays the merging of digital advancements with conventional techniques to optimize the rehabilitation of a patient with terminal dentition. This approach enhances the predictability and success of full-arch implant-supported prostheses by addressing the inherent limitations of both methods when used in isolation. Precision and efficiency have increased substantially in modern implant dentistry through digital planning and guided surgery. The patient’s postoperative experience can be greatly improved with immediate placement of an interim prosthesis, restoring function and aesthetics on the day of surgery.
Despite the advantages of digital technology, the decision to use an analog technique for the definitive prosthesis underscores the current limitations of intraoral scanners for full-arch implant-supported prostheses. This case demonstrates how combining digital and conventional methods can streamline the workflow and reduce the risk of complications from improper implant placement or a non-passive fit.
Patient feedback and prototype testing were crucial in refining the prosthetic design before fabrication of the final prosthesis. This adaptability in the treatment plan created a more aesthetically pleasing result and improved overall patient satisfaction.
Conclusion
The use of dental implants can provide life-changing treatment for edentulous patients. Careful case selection and planning is key for obtaining optimal results. This case report illustrates the effective use of a hybrid digital-analog workflow for rehabilitating a patient with maxillary terminal dentition. By combining digital techniques such as intraoral scanning, CBCT imaging, and facial scans with conventional splinted open-tray impressions, the treatment achieved precise implant placement and ensured a passive fit for the definitive prosthesis. Overall, this hybrid approach highlights the benefits of integrating digital and traditional methods in complex full-arch rehabilitations. As digital technologies continue to evolve, further comparative studies are required to establish standardized protocols that take full advantage of these innovations in clinical practice. 
Oral Health welcomes this original article.
References
- T. Flügge, J. Kramer, K. Nelson, S. Nahles, F. Kernen. 2022. Digital implantology—a review of virtual planning software for guided implant surgery. Part II: Prosthetic set-up and virtual implant planning, BMC oral health 22(1): 1-11.
- Spear F. 1999. The maxillary central incisor edge: a key to esthetic and functional treatment planning. Compend Contin Educ Dent. 20(6):512-516.
- Ganz SD, Tawil I. 2019. Full-arch implant surgical and restorative considerations: utilizing a full template guidance technique. Dent Today. 38(9):72–8.
- Katsoulis J, Takeichi T, Gaviria S, Peter L. 2017. Misfit of implant prostheses and its impact on clinical outcomes. Definition, assessment and a systematic review of the literature. Eur J Oral Implantol. 10(Suppl 1): 121-138.
- Cheng J, Zhang H, Liu H, Li J, Wang H, Tao X. 2024. Accuracy of edentulous full-arch implant impression: An in vitro comparison between conventional impression, intraoral scan with and without splinting, and photogrammetry. Clin Oral Impl Res. 35:560-572.
- Revilla-Leon M, Att W, Ozcan M, Rubenstein J. 2021. Comparison of conventional, photogrammetry, and intraoral scanning accuracy of complete-arch implant impression procedures evaluated with a coordinate measuring machine. J Prosthet Dent. 125(3): 470-478.
- Gaikwad A, Joshi A, Oliveira-Neto O, Padhye A, Nadgere J, Ram S, Yadav S. 2022. An overview of systematic reviews and meta-analyses evaluating different impression techniques for implant-supported prostheses in partially and completely edentulous arches. Int J Oral Maxillofac Implants. 37(6):1119-1137.
- Palantza E, Sykaras N, Zoidis P, Kourtis S. 2024. In vitro comparison of accuracy between conventional and digital impression using elastomeric materials and two intra-oral scanning devices. J Esthet Restor Dent. 1-20.
- Ma J, Zhang B, Song H, Wu D, Song T. 2023. Accuracy of digital implant impressions obtained using intraoral scanners: a systematic review and meta-analysis of in vivo studies. Int J Implant Dent. 9:48.
- Mehta S, Sutariya P, Pathan M, Upadhyay H, Patel S, Kantharia N. 2021. Clinical success between tilted and axial implants in the edentulous maxilla. A systematic review and meta-analysis. J Indian Prosthodont Soc. 21(3): 217-228.
- Asawa N, Bulbule N, Kakade D, Shah R. 2015. Angulated implants: An alternative to bone augmentation and sinus lift procedure: Systematic review. J Clin Diagn Res. 9(3): 10-13.
- Walter L, Greenstein G. 2020. Utility of measuring anterior-posterior spread to determine distal cantilever length off a fixed implant-supported full-arch prosthesis: A review of the literature. JADA. 151(10): 790-795.
About the Authors

Marijana Eic completed her Doctor of Dental Surgery degree at the University of Toronto. She worked as a general dentist for 12 years before pursuing her specialty training in prosthodontics. She is currently a third year graduate prosthodontics resident at the University of British Columbia.

Don Robertson completed his Doctor of Dental Surgery degree at the University of the Pacific. He is currently a third year graduate periodontics resident at the University of British Columbia.

Jae Won Sim obtained his Bachelor of Industrial Design from Emily Carr University of Art and Design. He has worked in the dental field as a CAD/CAM technician for over 10 years. He is also a CAD instructor for the Dental Technology program at Vancouver Community College.