
As G. K. Chesterton once wrote, “A man does not know what he is saying until he knows what he is not saying.” Use of the term “temporomandibular disorders” (TMD) clearly fits this description. Having been introduced into the literature as a means of solving a complex taxonomic dilemma, the term has been misused to the degree that it now has led to more confusion than clarification. Perhaps it is time to reconsider the value of maintaining this diagnostic classification. In making this decision, it is important to understand how we arrived at the current situation.
HISTORY OF THE TERM “TEMPOROMANDIBULAR DISORDERS”
Initially, although all of the conditions affecting the temporomandibular joint (TMJ) were not fully recognized or understood, there was a disease concept of TMJ involvement and conditions such as arthritis, ankylosis and mandibular dislocation were described and treated. Before the establishment of formal education in dentistry in the 1800s, these conditions were generally treated by physicians. Dentistry’s interest in this area was first sparked by an article by Prentiss in 19182, who suggested that “When the teeth are extracted the condyle is pulled upward by the powerful musculature and pressure on the meniscus results in atrophy.” Subsequently, publications by Summa, 3 Monson, 4 Wright5 and Goodfriend6 suggested other causes for the symptoms that these patients experienced such as missing teeth, lost vertical dimension, and the resulting displacement of the mandible. However, the focus was still on diseases of the TMJ.
All this changed in 1934 when the first of a series of articles by otolaryngologist James Costen7 not only resulted in even greater involvement by dentists in the management of TMJ disorders, but also changed the entire diagnostic concept. In this article, he described a series of TMJ, ear and “sinus” symptoms the ultimately came to bear his name (Costen syndrome), which he attributed to nerve impingement due to over-closure of the bite. Although it was eventually was shown that his anatomic explanations for the causes of the various symptoms was incorrect, 8,9 his work still had a profound and long-lasting effect on the manner in which TMJ pan and dysfunction was subsequently diagnosed and treated. As a result of his influence, there was a dramatic shift from the previous disease concept of diagnosis to a symptom (syndrome) concept of diagnosis in which conditions of diverse etiology were combined under one diagnostic heading merely because they produced similar signs and symptoms of pain and dysfunction. Moreover, this also led to a “one diagnosis, one treatment” philosophy, which may explain some of the reasons why clinicians had difficulty in successfully managing the care of many of these patients.
Although the term “Costen syndrome” ultimately was abandoned and through the years was replaced by such terms as “TMJ syndrome,” “TMJ pain-dysfunction syndrome,” “mandibular pain-dysfunction syndrome” and “craniomandibular syndrome,” the same diagnostic and treatment errors continued to be made. The focus still was on the TMJ, the etiology still was considered to be an alteration in the occlusion that caused condylar displacement (mechanical displacement theory),10,11 and treatment consisted mainly of various modifications of the occlusion (occlusal equilibration), orthodontics and full-mouth reconstruction).12,13 However, the evidence for these concepts was based mainly on the opinions of strong personalities and anecdotal success stories rather than on science, careful research and unbiased clinical data. As noted by Landa, 14 “One of the gravest mistakes in the diagnosis of temporomandibular joint disturbances is the misinterpretation of certain positions of the condyle head in the glenoid fossa as evidence of pathology.”
It was not until the 1950s that Schwartz15,16 and his colleagues at Columbia University demonstrated that the masticatory muscles were contributing to some of the pain and dysfunction seen in patients with TMJ paindysfunction syndrome. Although they still believed that improper occlusion may be a contributing factor, they emphasized that what patients do with their teeth in reacting to stress may be even more important than any malocclusion that they may have.
In 1969, on the basis of investigations my colleagues and I conducted at the University of Illinois TMJ and Facial Pain Research Center, I expanded on the psychophysiologic concepts of Schwartz and colleagues and proposed an entirely new theoretical concept of etiology for the muscular disorders. 17 I also urged a change in nomenclature that would clearly separate the muscular disorders from the intracapsular TMJ pathology, suggesting use of the term “myofascial paindysfunction (MPD) syndrome” for the former conditions.
As a result of the contributions of Schwartz16 and colleagues and my colleagues and me, 17 there was a gradual acceptance by some clinicians that patients experiencing pain and dysfunction could have a joint problem, a muscle problem or both. Nevertheless, many clinicians continued to focus on correction of the occlusion as the way to manage these conditions. Recognizing the existing confusion in the field, in 1982 Robert H. Griffiths, then president of the American Dental Association, ar ranged for the organization of The President’s Conference on The Examination, Diagnosis and Management of Temporomandibular Disorders with the hope of “establishing a rational, unbiased approach to these disorders” (cited in Laskin and colleagues18) Some of the resulting recommendations from this conference were that the use of broad, nonspecific diagnostic labels such as “temporomandibular joint dysfunction” be discouraged, that the all-inclusive umbrella term be “temporomandibular disorders” and that separated under this heading would be conditions that primarily involved the muscles of mastication and those that involved the TMJ. Whereas this seemed like a logical solution to a confusing situation, a review of the literature since that time indicates that it has not necessarily had the desired effect. Unfortunately, many clinicians have merely substituted the inclusive term “TMD” problem” for “TMJ problem” without changing their thinking about the source of each patient’s problem, its diagnosis, its etiology or its specific treatment. Perhaps even more confusing has been use of the term TMD as a singular noun in the literature, making it difficult to determine what condition (or conditons) the “TMD patient(s)” actually had and, therefore making it impossible to interpret the findings logically and apply them clinically.
THE CURRENT SITUATION
A review of some of the current literature shows many instances of such confusion. For example, examination of the 18 issues of The Journal of the American Dental Association published from January 2006 to June 2007 revealed seven articles dealing with TMDs. In four of these articles, either the Research Diagnostic Criteria for Temporomandibular Disorders (RCD/TMD) 19 were used correctly to indicate the patient population or the conditions being studied were specifically stated. 20-23 In three other articles, however, it was not possible to establish clearly what condition was being investigated 24-26 or, therefore, how to apply the findings. In an article entitled “Efficacy of an early intervention for patients with acute temporomandibular disorder-related pain: A one-year outcome study” 24 selection of the subjects was based on palpation of 20 muscle sites and potential subjects’ answers to the question, “Have you had pain in the face, jaw, temple, in front of the ear, or in the ear in the last month?” Based on such criteria, this would obviously include patients with both myogenous and arthrogenous problems, who might respond differently to a biopsychosocial intervention; however, no distinction was made.
Another example of an ill-defined subject p
opulation is found in the article entitled “Thirdmolar extraction as a risk factor for temporomandibular disorder.” 25 In this study, the authors examined the dental insurance records of 34,491 subjects who had had third molars removed for claims indicating subsequent development of TMD. The authors found that 391 patients had such claims and concluded that
third-molar removal is a risk factor. However, without knowledge of the specific diagnoses of the conditions that were included, it is not possible to conclude that there is a cause-and-effect relationship, because there are temporomandibular disorders that could not possibly be caused by a tooth extraction, such as degenerative arthritis or an internal derangement in a patient with a previously normal TMJ.
Examples of similar problems in accurately identifying the subjects studied also can be found in articles published in other journals. In two reports published in a single issue of the Journal of Orofacial Pain 27-28 researchers studied coping mechanisms in patients who had at least one RDC/TMD Axis I TMD pain diagnosis. 19 This study, therefore, would have included patients with a muscle problem diagnosis, a disk displacement, or arthralgia or arthritis. On the basis of their findings, one would have to assume that the coping mechanisms would be the same regardless of which condition was the cause of the chronic pain. Although this may be true, it also is possible that dividing the subjects into the three specific diagnostic categories would have revealed differences.
An article in Angle Orthodontist entitled “TMD in relation to malocclusion and orthodontic treatment” 29 is another example of how using TMD as a single entity makes what could be useful information difficult to interpret. The purpose of this study was to answer the question “Are signs and symptoms of TMD related to malocclusion or orthodontic treatment?” After an extensive review of 58 articles, the authors found that associations between specific malocclusions and the development of significant signs and
symptoms of TMD could not be verified. However, there was no indication of either the specific TMDs that were being evaluated or the types of malocclusion that were being considered. Whereas malocclusions may not be associated with the development of myofascial pain or an internal derangement, one certainly would expect to see various types of malocclusion in people with developmental disturbances.
RESOLVING THE DIAGNOSTIC DILEMMA
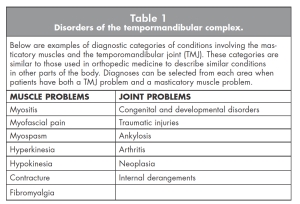
Clearly, the simplest way to avoid the diagnostic confusion in the literature is to eliminate use of the term “TMD. Although it once may have served a useful purpose as a transition from even worse diagnostic labeling, its continued use no longer can be defended in light of the many scientific advances that have been made in this field. Because the term TMD mixes together conditions involving two separate anatomic areas, it is not logical to use such an umbrella term to describe these disorders when the conditions in each area now can be diagnosed precisely and assigned specific names (Table 1). This is framework/nomenclature of temporomandibular disorders rather than the categories I have suggested here.
CONCLUSIONS
Just as we once abandoned use of the term “TMJ syndrome” because our increased knowledge about the patients involved allowed more accurate diagnosis and treatment, so the time has come to eliminate TMD from our vocabulary. Table 1 provides a list of the more common diagnostic terms that I suggest be substituted for TMD. When reporting particularly important for clinicians to consider when determining the appropriate treatment for a patient.
Moreover, to standardize future reporting in the literature and make it possible to determine the exact conditions being studied, I suggest that Axis I of the RDC/TMD19 be reorganized into the recommended major categories of muscle and joint conditions, and that the subcategories be expanded to include the missing diagnoses. I also propose that the title be changed to Research Diagnostic Criteria for Disorders of the Temporomandibular Complex. In this regard, it should be noted that the original RDC/ TMD is currently in the process of major revision, based on a 5-year multi-center validation study30, 31 and that a new version will be proposed after these data are published. This version is expected to contain some new diagnostic categories as well as some changes in the present ones. However, it is not likely that this revision will satisfy the objections I have raised in this article, because the authors still maintain the diagnostic their findings, authors need to use these terms and define clearly their study patient populations. Moreover, journal editors need to monitor more carefully that this is being done before accepting an article for publication.
OH
Dr. Laskin is a professor and chairman emeritus, Department of Oral and Maxillofacial Surgery, School of dentistry, Virginia Commonwealth University, Richmond, VA.
Oral Health welcomes this original article.
REFERENCES
1. Chesterton GK, Essay III: about impenitence. Quoted in: Tripp RT, ed. The international thesaurus of quotations. New York: Harper & Row; 1987:87.
2. Prentiss HJ. A preliminary report upon the temporomandibular articulation in the human. Dent Cosmos 1918; 60(6):505-12.
3. Summa R. The importance of the interarticular fibrocartilage of the temporomandibular articulation. Dent Cosmos 1918; 60(6):512-4.
4. Monson GS. Impaired function as a result of closed bite. JADA 1920; 7(5):399-404.
5. Wright WH. Deafness as influenced by malposition of the jaws. JADA 1920;7(12):979-92.
6. Goodfriend DJ. Dysarthrosis and subarthrosis of the mandibular articulation. Dent Cosmos 1932; 74(6):523-35.
7. Costen JB. A syndrome of ear and sinus symptoms dependent upon disturbed function of the temporomandibular joint. Ann Otol Rhin Laryng 1934; 43(1):1-15.
8. Sicher H. Temporomandibular articulation in mandibular overclosure. JADA 1948; 36(2):131-9.
9. Zimmerman AA. An evaluation of Costen’s syndrome from an anatomic point of view. In: Sarnat BG, ed. The temporomandibular joint. Springfield, III: Charles
C. Thomas; 1951:82-110.
10. Thompson JR. Abnormal function of the stomatognathic system and its orthodontic implications. Ann J Orthod 1962; 48(10): 758-65.
11. Ricketts RM, Roentgenography of the temporomandibular joint. In: Sarnat BG, ed. The temporomandibular joint. 2nd ed. Springfield, Ill: Charles C. Thomas; 1964:102-32.
12. Ramfjord SP, Ash MM, Occlusion. Philadelphia: Saunders; 1966.
13. Shore NA. Occlusal equilibration and temporomandibular joint dysfunction. Philadelphia:Lippincott; 1959.
14. Landa JS. A preliminary survey and a new approach to the study of the temporomandibular joint syndromes Ann Den 1950; 9(1):5-12.
15. Schwartz LL. Pain associated with the temporomandibular joint. JADA 1955; 51(4):394-7.
16. Schwartz LL. Disorders of the temporomandibular joint: Diagnosis, management, relation to occlusion of teeth. Philadelphia: Saunders; 1959.
17. Laskin DM. Etiology of the pain dysfunction syndrome. JADA 1969; 79(1):147:53.
18. Laskin DM, Greenfield W, Gale E., et al, eds. The president’s conference on the examination, diagnosis and management of temporomandibular disorders. Chicago: American Dental Association; 1983.
19. Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders, review, criteria, examinations and specifications, critique. J Craniomandib Disord 1992; 6(4):301-55.
20. Klasser GD, Okeson JP. The clinical usefulness of surface electromyography in the diagnosis and treatment of temporomandibular disorders. JADA 2006; 137(6):763-71.
21. Wassell RW, Adams N, Kelly PJ. The treatment of temporomandibular disorders with stabilizing splints in general practice: one-year follow-up JADA 2006; 137(8):1089-98.
2
2. Truelove, E, Huggins KH, Marcl L, Dworkin SF. The efficacy of traditional, low-cost and nonsplint therapies for temporomandibular disorders: a randomized controlled study. JADA 2006; 137(8):1099-107
23. Conti PC, dos Santos CN, Kogawa EM, de Castro Ferreira Conti AC, dos Reis Pereira de Araujo C. The treatment of painful temporomandibular clicking with oral splints: a randomized clinical trial. JADA 2006; 137(8):1108-14.
24. Gatchel RJ, Stowell AW, Wildenstein L, Rigs B, Ellis E 3rd. Efficacy of an early intervention for patients with acute temporomanibular disorder-related pain: a one-year outcome study. JADA 2006; 137(3):339-47.
25. Huang GJ, Rue TC. Third-molar extraction as a risk factor for tempormandibular disorder. JADA 2006; 137(11):1547-54.
26. Stowell AW, Gatchel RJ, Wildenstein L. Cost-effectiveness of treatments for temporomandibular disorders: biospcyhosocial intervention versus treatment as usual. JADA 2007; 138(2):202-08.
27. Brister H. Turner JA, Aaron IA, Mancl LA. Selfefficacy is associated with pain, functioning, and coping in patients with chronic temporomandibular disorder pain. J Orofac Pain 2006; 20(2): 115-24.
28. Aaron LA, Turner JA, Mancl LA, Sawchuk CN, Huggins KH, Truelove EL. Daily pain coping among patients with chronic temporomandibular disorder pain: an electronic diary study. J Orafac Pain 2006; 20(2):125-37.
29. Mohlin B, Axelsson S, Paulin G, et al. TMD in relation to malocclusion and orthodontic treatment. Angle Orthod 2007; 77(3):542-8.
30. Steenks MH, deWijer A. Validity of the research diagnostic criteria for temporomandibular disorders Axis I in clinical and research settings. J Orofac Pain 2009; 23(1):9-16.
31. Greene CS. Validity of the research diagnostic criteria for temporomandibular disorders Axis I in clinical and research settings (Critical Commentary 2), J Orofac Pain 2009; 23(1): 20-23.
———
Evidence for these concepts was based mainly on the opinions of strong personalities and anecdotal success stories
———
Unfortunately, many clinicians have merely substituted the inclusive term “TMD” problem” for “TMJ problem” without changing their thinking about the source of each patient’s problem
———
After an extensive review of 58 articles, the authors found that associations between specific malocclusions and the development of significant signs and symptoms of TMD could not be verified
———
The time has come to eliminate TMD from our vocabulary