


Congratulations! You did it. We are proud of you.
Our patients are very happy as we are celebrating the completion of their orthodontic treatment. They check their smile at every possible angle, could not stop smiling, and cannot wait to celebrate it with their families and friends.
Our job as their orthodontists is not only optimize their bite and create a beautiful smile that fits their facial type; but also educate them about the stabilization of the treatment results and long-term maintenance of their bite. There is a misconception among the dentists and the public that the orthodontic treatment could result in teeth that were straight for a lifetime.1 There are many factors affecting the neutral zone for the teeth as our patients age such as changes in the muscle tone in the oral-facial complex, parafunctional oral habits, age-related or pathological changes in the mandibular condyle, etc. Understanding craniofacial development, growth, and the adaptation to its ever-changing dynamic functional needs is the key to make clinical decisions regarding the post-orthodontic retention needs of our patients.
The majority of the orthodontic practices offer a period of “supervised retention” to their patients and communicates the customized retention recommendation with the patient’s general dentists. It is extremely important to work as a team to achieve long term clinical success in maintaining a functional bite and aesthetic smile. The general dentists continue to see their patients on a regular basis and have an opportunity to assess the orthodontic retainers and the bite after the supervised retention period is completed by the orthodontists. With great care, orthodontic retainers would serve for a long time (Fig. 1) without any major issues. However, in some cases, the failure to notice the clinical problems early on results in functional issues that would require a comprehensive orthodontic treatment to correct it (Fig. 2).
Fig. 1A

Fig. 1B

Fig. 1C

Fig. 2A

Fig. 2B

Fig. 2C

The purpose of this article is to provide general dentists a short review on different types of tooth movements and to share some clinical guidelines on orthodontic retainer check protocol in dental recall appointments.
Different types of tooth movement
The teeth move throughout life. Understanding the different types of tooth movement makes it possible to determine the clinical decisions to help our patients to maintain the aesthetics of their smile and functionality of their bite.
1. Physiologic tooth migration
In simple terms, this tooth movement refers to the maturational changes that happen in humans as they age. Rajbhoj et al’s2 systematic review on dental changes in humans with untreated normal occlusion throughout lifetime concludes that:
- maxillary and mandibular inter-canine width de-creases after 13 years and 8 years of age, respectively;
- maxillary and mandibular inter-molar width de-creases after 15 years and 26 years of age, respectively;
- arch length and perimeter decrease after 8 years of age;
- crowding steadily increases from early permanent dentition until 60 years of age and incisor crowding is greater in mandibular arch, as well as in females.
These changes are partly due to the continuous changes in the size and shape of the craniofacial complex throughout a considerable part of adulthood.3
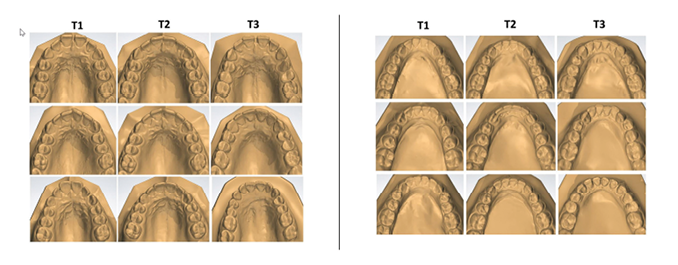
Physiologic tooth migration in orthodontically treated populations often cannot be distinguished from what is considered a relapse of the orthodontic treatment itself.4 In a 40-year follow up study comparing the aging changes of the dental arches in patients in untreated normal occlusion and non-extraction treated occlusion by Freitas et al5 showed that both groups showed maturational changes but the severity of the change is at a lesser degree in untreated subjects (Fig. 3).
Fig. 3
2. Pathologic tooth migration
This tooth movement refers to the tooth movement when there is a significant change in the functional dynamics of the bite such as oral habits (Fig. 4), missing teeth (Fig. 5), periodontal disease (Fig. 6), clenching (Fig. 7) etc.
Fig. 4A

Fig. 4B
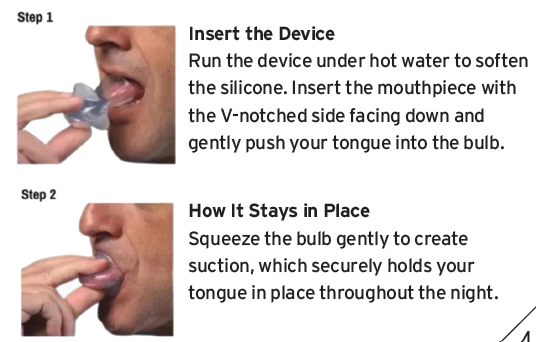
Fig. 4C

Fig. 4D

Fig. 5A

Fig. 5B

Fig. 5C

Fig. 5D

Fig. 6A

Fig. 6B

Fig. 6C

Fig. 6D

Fig. 7A

Fig. 7B

Fig. 7C

3. Rapid-to-slow tooth movement soon after removal of orthodontic appliances
This type of tooth movement occurs during the period of remodeling of the periodontal structures soon after the active orthodontic appliances are removed. In the absence of compliance with the orthodontic retainers, the tooth movements are seen within weeks after the removal of the orthodontic appliances (Fig. 8).
Fig. 8A

Fig. 8B

Supervised retention period
Supervised retention period starts once the active phase of the treatment is completed and all the orthodontic appliances are removed. During this period the orthodontist is able to assess the initial stability of the orthodontic treatment outcome, the compliance with the orthodontic retainers and the state of the orthodontic retainers. The frequency with which the patients are seen during the supervised retention period depends on the severity of the malocclusion, the complexity of the treatment and the psycho-social maturity of the patient.
Unsupervised retention period
This period starts after the patient is released from orthodontic care to the long-term care of their general dentist. Usually, the patients and their dentist receive a communication letter from the orthodontist outlining the retention recommendation going forward. Even with our best efforts to maintain a good treatment outcome, it should be noted that post-retention changes are unpredictable. Therefore, long-term retention is recommended to ensure the stability of the occlusion.
General dentists have the great advantage point of seeing their patients on a regular basis and diagnose the changes in their patients’ occlusion. It is important to ask and document any concerns regarding the patient’s smile and assess the occlusion at regular recall appointments. In this way the patients will be reminded to be aware of their maturational changes in their dentition and will become partners in the retention process.
If the patients are fitted with fixed orthodontic retainers and/or wearing removable retainers to maintain the alignment of their teeth; assessment of the condition of the orthodontic retainers should be a part of the dental recall exam. Early detection of any issues with the orthodontic retainers could be resolved with simple repairs or replacements and this would prevent more complex and expensive treatment options later on.
Step-by-step orthodontic retainer check protocol for general dentists:
1. Recordkeeping
Recording the type of the retainers and the orthodontist’s retention recommendation in the patient’s dental chart. Asking the patient their retainer practices, especially wear time, discomfort, fitting issues, cleaning practices and document the answers in the patients’ chart.
2. Removable retainer fit (Fig. 9AB)
A good fit means that:
i. there is no space between the teeth and the orthodontic retainer
ii. there is a snug fit, not too loose not too tight
iii. there is no rocking
Fig. 9A

Fig. 9B

3. Removable retainer condition (Fig. 10AB)
Checking for:
i. wear or tear on the retainer
ii. staining, excessive built up or foul smell
iii. incomplete or complete fracture
Fig. 10A
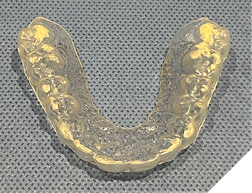
Fig. 10B

4. Bonded permanent retainer (Fig. 11AB)
Checking for:
i. smooth edges
ii. intact wire
iii. sufficient composite resin amount on bonded teeth
iv. showing good stability when checked with a hand instrument
Fig. 11A

Fig. 11B

Fig. 11C

Fig. 11D

5. Oral hygiene (Fig. 12AB)
Checking for:
i. Bleeding upon probing
ii. Plaque/calculus amount at the gingival of the fixed retainer
iii. Any gingival recession or hyperplastic gingival tissues
Fig. 12A

Fig. 12B

Conclusion
The majority of the orthodontic treatment stability is achieved within the first year after the active orthodontic appliances are removed. It is expected that the tooth positions and the occlusion will undergo continuous change many years after the orthodontic treatment is completed. Educating our patients about these age-related changes in occlusion is essential to prevent misconceptions regarding the long-term stability or perceived failure of orthodontic treatment. Implementing a simple retainer check routine into recall examination would let your patients know that they are responsible for observing post-treatment changes. Then, when post-treatment changes happen, you could offer different treatment options and have them decide how they would like to proceed. 
Oral Health welcomes this original article.
All photos that are submitted are from my clinic except Figure 3 (Copyright and License Information is below) and Figure 4B (this is an online advertisement of the appliance that my patient used)
Copyright and License information for Figure 3: Open Access.This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
References
- Vanarsdall, R.L. and White, R.P. Jr.: Relapse and retention: Professional and public attitudes. Am. J. Orthod. 98:184, 1990.
- Rajbhoj AA, Parchake P., Begnoni G., Willems G., Llano-Perula MC. Dental changes in humans with untreated normal occlusion throughout lifetime: A Systematic scoping review Am J Orthod Dentofacial Orthop 2021;160:340-62.
- Behrents RG. Growth in the Aging Caraniofacial Skeleton. Craniofacial Growth Series. Ann Arbour, MI: Center for Human Growth and Development, University of Michigan; 1985. Monograph #17.
- Sinclair, P. M. & Little, R. M. Maturation of untreated normal occlusions. Am. J. Orthod.83, 114–123 (1983)
- Freitas KMS, Massaro C, Miranda F, Gambardela-Tkacz CM, Cotrin P, de Freitas MR, Garib D. Comparison of aging of nonextraction treated and normal untreated occlusions: 40-year follow up. Sci Rep. 2024 Oct 26;14(1):25458. doi: 10.1038/s41598-024-76976-9. PMID: 39462009; PMCID: PMC11513092.
About the author

Dr. Emel Arat is a former Assistant Professor at the University of Toronto and past president of Ontario Association of Orthodontists and is in private practice in Leaside, Toronto, Ontario. She can be reached at drarat@leasideortho.ca