
Abstract
There is a growing demand for fixed full arch implant supported restorations.1 The procedures associated with this type of treatment can be daunting due to the complexity of all aspects of this treatment modality, from the initial data gathering and diagnosis to the surgical and prosthetic treatment implementation.2 Recent technology with its associated workflows can streamline these procedures as well as remove the complexity, while improving the predictability of the outcome for this type of treatment.3 This report will introduce and describe the use of technology from the patient assessment through the delivery of the final fixed full arch implant supported prosthesis. Technology with its workflows impacts all phases of treatment, including data gathering, analysis of the patient, developing a treatment plan, performing surgical procedures, immediate provisionalization of implants, and the steps required to deliver a precise final implant supported prosthesis in a simplified efficient manner.4
The prevalence of edentulousness in Canada is 11% for adults 60 years old and older.5 In addition, there are an uncalculated number of people on their way to being edentulous due to periodontal disease, excessive caries as well as congenital and pathological disorders.6
Treatment of the edentulous patient can include complete dentures, overdentures, and fixed implant solutions. The fixed implant solution is frequently the preferred patient choice due to the increased quality of life enjoyed with fixed teeth over removeable prosthesis.7 Fixed full arch implant treatment can be complex and time consuming.2 New workflows and technology have streamlined the diagnosis, treatment planning, as well as surgical and prosthetic treatment implementation.8 This has made the full arch implant solution more efficient, effective, and predictable than previously experienced.9
Diagnostic and digital workflows
Diagnosis is accomplished by taking photos (intraoral and extraoral, conventional radiographs, PAs and panoramic xrays), iOS scans and CT scans, and performing a clinical exam. Virtual prosthetic software simplifies diagnostic wax-ups which are then integrated into CT scan-based implant surgical planning software.10 Virtual motion tracking hardware and software (eg. Modjaw) may be utilized to incorporate analysis of vertical dimension and functional jaw movements.11 All of this data then is used to complete a comprehensive diagnosis and treatment plan.
Technological treatment tools, such as computer guided surgery using surgical guides or handpiece assisted guidance, is then used to help implement surgical treatment.12 Intraoral scanning with 3D printing or rapid denture conversion solutions are used to immediately provisionalize the full arch of implants.9,13 Full digital workflows that ensure and validate prosthetic precision have been developed and are commercially available. They allow a full arch final prosthesis to be inserted at a high level of accuracy (10 micron average linear deviation) in a 3-appointment workflow.14 This type of streamlined digital workflow creates efficiency and predictably in a simplified workflow which should make full arch implant treatment more accessible to the general public.15
Case report
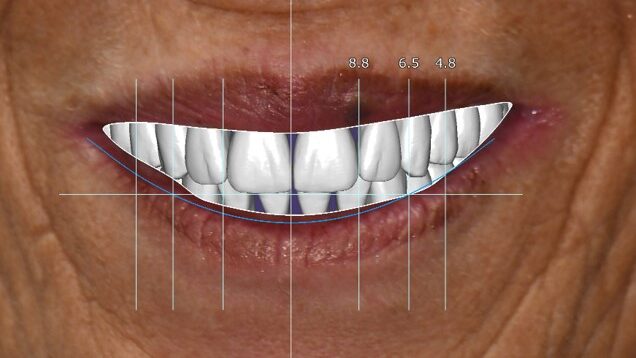
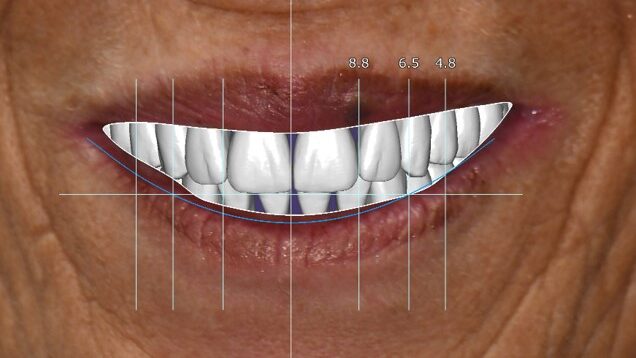
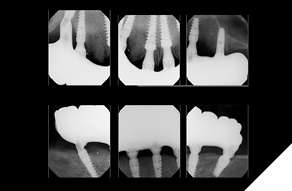
A 55-year-old woman presented with a chief complaint of wanting to complete the treatment of her maxilla and mandible that had begun elsewhere a number of years ago. The patient reported that she had several implants placed and provisional bridges inserted a number of years ago. A review of her medical history revealed no significant findings. A clinical exam was performed, and the following data was collected: a full mouth series radiographic survey, a cone beam CT scan, intraoral surfaces scans, full face and intraoral photos (Figs. 1,2,3).
Fig. 1

Fig. 2
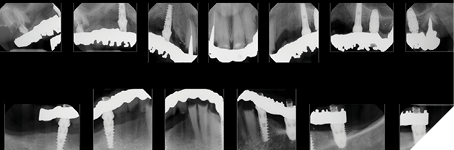
Fig. 3

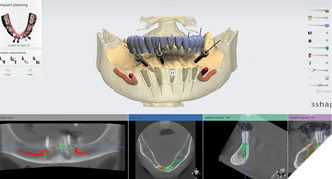
The data recorded during the clinical exam in conjunction with the FMS xrays and CT scan data were analyzed, and a diagnosis was made as to the viability of the patient’s existing teeth. A virtual diagnostic wax up was completed using prosthetic planning software (ExoCad) (Figs. 4A, 4B). The .STL file of the virtual wax up was integrated with the CT scan data in implant surgical planning software (3Shape Implant Studio) and a surgical plan was designed (Figs. 5A, 5B). The viability of this surgical plan was then evaluated in conjunction with the previously determined prognosis of the patient’s existing dentition and surrounding periodontium, and a treatment plan was formulated. The plan with the anticipated predictability of achieving the planned result was presented to the patient. The patient approved the treatment plan.
Fig. 4A
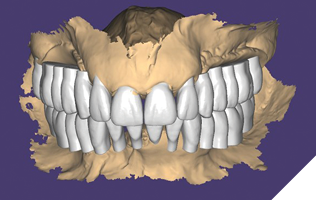
Fig. 4B
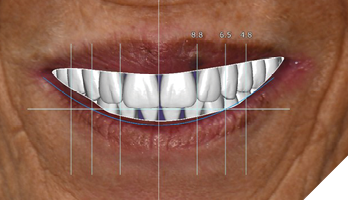
Fig. 5A
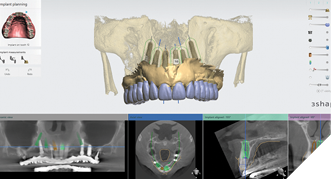
Fig. 5B
All teeth and implants were evaluated, and it was determined that due to their poor and compromised prognosis that fully implant supported fixed prosthesis would be the treatment of choice and that all the patient’s remaining teeth would be extracted. The patient had 1 maxillary implant that was to be retained due to its favorable prognosis. All other maxillary implants and mandibular implants exhibited significant bone loss and were to be removed.
Treatment phase: The patient requested that we treat the maxilla first followed by the mandible. The surgical visit included the following treatment. Extraction of teeth 2,7,8,9,15 and removal of implants 5 and 13. Implant 14 was kept due to its good bone support and favorable prognosis (Figs. 6A, 6B). Computer guided surgery (Keystone – Contra Angle Guidance System) with a surgical guide was utilized to perform all osteotomies and place the dental implants (Figs. 7A, 7B).
Fig. 6A

Fig. 6B

Fig. 7A
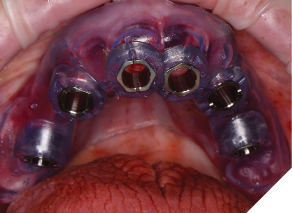
Fig. 7B

Implants were placed in tooth positions 4,6,8,9 and 12 (Genesis Active – Keystone Dental). Allograft bone grafts (Dynacore – Keystone Dental) were placed into all extraction sockets and intraboney defects. Multiunit abutments were inserted and torqued to 30ncm (Figs. 8A, 8B). All soft tissues were sutured. Nexus scan gauges (Osteon Medical KDG) were placed on the multiunit abutments and iOS impressions were taken (Figs. 9, 10). The pretreatment virtual wax-up was integrated to the actual implant positions using prosthetic design software (Exocad) and the provisional restoration was 3D printed (Figs. 11A, 11B).
Fig. 8A
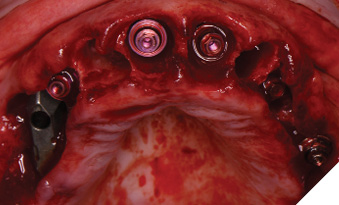
Fig. 8B

Fig. 9

in the scan path and implementation
of artificial intelligence algorithms.
Fig. 10

Fig. 11A
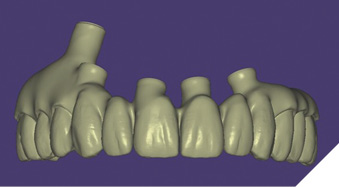
Fig. 11B

The printed provisional restoration was inserted and the patient was sent home. The patient returned 5 days later and a new machined provisonal restoration was inserted due to its superior strength (Figs. 12A, 12B).
Fig. 12A

Fig. 12B

Three weeks later, the patient returned for treatment of the mandible (Figs. 13A, 13B). Teeth 22,23,24 were extracted and implants 19,21 and 27 were removed. A surgical guide with computer guided surgery was used to prepare the osteotomies and place the implants (Figs. 14A, 14B). Implants (Genesis Active – Keystone Dental) were placed in tooth positions 19,20,23,26 and 30. Allograft bone grafts were placed into the extraction sockets and all intraboney defects. Multiunit abutments were inserted on all implants and torqued to 30ncm (Fig. 15). The soft tissues were sutured closed. A rapid denture conversion system was used to efficiently convert a denture into a fixed provisional restoration.20 (EasyPro – Keystone Dental). This denture conversion system maintained the structural integrity of the denture while maintaining an esthetic provisional restoration (Figs. 16A-D).
Fig. 13A

Fig. 13B

Fig. 14A

Fig. 14B
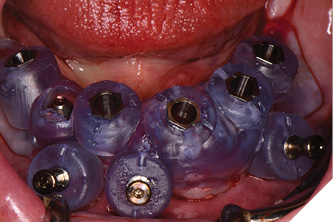
Fig. 15
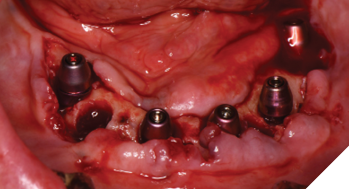
Fig. 16A

Fig. 16B

Fig. 16C

Fig. 16D

Nexus scan gauges (Osteon Medical – KDG) were placed on the multiunit abutments and iOS impressions were taken to record implant position for later use (Fig. 17). The completed provisional restoration was inserted and the patient was discharged (Figs. 18A, 18B).
Fig. 17

Fig. 18A

Fig. 18B

The patient returned after 3 months of healing (Figs. 19A, 19B). Accurate implant positions were recorded at the time of implant surgery using the Nexus scan gauges and protocol; however, as expected due to resolution of surgical swelling and bone remodeling, there were soft tissue changes following complete healing of the mandible and maxilla. Final prosthetic steps were now begun.
Fig. 19A

Fig. 19B

The full Nexus protocol was not required due to the accurate impressions of the implant positions using the Nexus protocol at the initial implant surgical visits. The Nexus protocol used at this point was impressioning of the healed soft tissue (emergence profile scan) (Figs. 20A-C), iOS scans of the maxillary and mandibular provisional restorations intraorally (seated on the supporting multi-unit abutments), iOS scan of the centric occlusion intraorally (Fig. 21) and iOS scans of the maxillary and mandibular provisional restoration removed from the patient’s mouth (Figs. 22A, 22B).
Fig. 20A

Fig. 20B
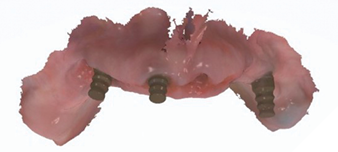
Fig. 20C

Fig. 21

Fig. 22A

Fig. 22B

These new records along with the Nexus scans taken at the time of implant surgery were sent to Osteon Medical through the Nexus iOS portal with instructions to replicate the provisional restoration design with correct adaptation to the healed soft tissue. Three days after the data was submitted to Osteon Medical, .STL files of the final design for the maxillary and mandibular restorations were sent through the portal to our office and 3D printed in our office (Figs. 23A-C).
Fig. 23A
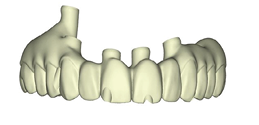
Fig. 23B
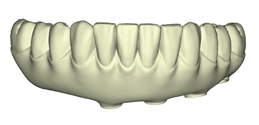
Fig. 23C

The patient returned 2 weeks from the impressioning appointment for a prototype try in. At this appointment the esthetics, phonetics, soft tissue approximation and occlusion were confirmed. There was no requirement for a verification jig due to the accuracy of the Nexus solution. The restorations were manufactured with milled gold anodized titanium bars overlaid with monolithic zirconia (Figs. 24A-C, 25A-C).
Fig. 24A

Fig. 24B

Fig. 24C

Fig. 25A

Fig. 25B

Fig. 25C

The patient returned 2 months later (due to patient scheduling delays) and the maxillary and mandibular Nexus restorations were inserted (Figs. 26A-C). Passive seating of the restorations were confirmed with the Sheffield test and radiographic confirmation. The occlusion was checked and final radiographs taken (Fig. 27).
Fig. 26A

Fig. 26B

Fig. 26C

Fig. 27
Discussion & conclusion
Full arch fixed implant restoration can be complex and demanding.2 However, there is a great need for this type of restoration.16 Fixed full arch implant restorations both improve quality of life, as well as function17 and may improve implant longevity.18
The workflow described here provides a streamlined, efficient, simplified protocol for managing full arch implant supported restoration treatment. The collection of data including the clinical exam, photos, conventional radiographs, CT scans, and intraoral scans provide comprehensive data to formulate an accurate diagnosis and complete treatment plan. The collection of this data can usually be accomplished in one patient visit (commonly the initial patient visit). Many of the clinical tasks of collecting this data can be done by the auxiliary staff which creates even more efficiencies.19
The clinicians can then share the digital data with their partner laboratory or a planning service to help create the virtual wax-up, come to a final diagnosis, make the treatment plan, create a surgical plan as well as the surgical guides and provisional restorations required. The surgery is carried out effectively using the prepared surgical plan, surgical guides, computer guided surgery and effective implant systems (including implants designed for immediate provisionalization and abutment systems with concave geometries that simplify their use with subcrestal implant placement as well as improving biological outcomes).20
Restorative solutions that utilize artificial intelligence (Nexus) that ensure accuracy in recording accurate implant positions, and build virtual models paired with precision manufacturing, produce restorations with 10–20 micron implant position accuracy.14 Creating passively seating implant supported restorations is predictable with this type of technology.21 The use of iOS impressions at the time of implant surgery with Nexus tools, workflows, and algorithms are used, allowing us to create designs and manufacture immediate provisional restorations.9 Final restorative procedures are simplified and can be accomplished in 3 patient visits.22
The general public has been exposed to the possibility of full arch implant supported restorations through social media and television. The demand for these types of restorations is growing. This type of solution makes full arch implant supported restoration more easily accessible to general restorative doctors as well as surgical and restorative specialists.
Today’s technology, tools, and workflows are able to support the growing demand for these restorations and, with the proper training, place the ability to manage this type of comprehensive treatment into the capable hands of dentists today. 
Oral Health welcomes this original article.
References
- Goodacre CJ, Goodacre BJ. Fixed vs. removable complete arch implant prostheses: a literature review. J Prosthodont. 2017;26(3):260–267.
- Gallardo, Y. N. R., da Silva-Olivio, I. R., Gonzaga, L., Sesma, N., & Martin, W. (2019). A systematic review of clinical outcomes on patients rehabilitated with complete-arch fixed implant-supported prostheses according to the time of loading. Journal of Prosthodontics, 28(9), 958-968. https://doi.org/10.1111/jopr.13104
- Auduc, C., Douillard, T., Nicolas, E., & El Osta, N. (2025). Fully Digital Workflow in Full-Arch Implant Rehabilitation: A Descriptive Methodological Review. Prosthesis, 7(4), 85. https://doi.org/10.3390/prosthesis7040085
- Joda T, Ferrari M, Gallucci GO, Wittneben JG, Brägger U. Digital technology in fixed implant prosthodontics. Periodontol 2000. 2017;73(1):178–192.
- Statistics Canada. The Daily — Oral health of Canadians, 2022. Ottawa: Government of Canada; 2024.
- Felton DA. Edentulism and comorbid factors. J Prosthodont. 2009;18(2):88–96.
- Awad MA, Locker D, Korner-Bitensky N, Feine JS. Measuring the effect of intra-oral implant rehabilitation on health-related quality of life. J Dent Res. 2000;79(9):1659–1663.
- Joda T, Brägger U. Digital vs. conventional implant prosthetic workflows: a cost/time analysis. Clin Oral Implants Res. 2015;26(12):1430–1435.
- Gelb, D. A., Klein, M., & Tuckman, M. (2023). Immediate implant placement, immediate load with same-day fully digital fabrication of a screw-retained provisional implant prosthesis. Compendium of Continuing Education in Dentistry, 44(5),
- Kauling AE, et al. Integration of virtual prosthetic planning and surgical guides for implant dentistry. Int J Prosthodont. 2019;32(2):171–179.
- Bedrossian EA, et al. “Use of an optical jaw-tracking system to record mandibular motion for treatment planning and designing interim and definitive prostheses: A dental technique.” J Prosthet Dent. 2024.
- Klein, M., Waltuch, A., & Lehrfield, L. (2022). A digitally programmed technique to simplify sequential extraction implant treatment. Compendium of Continuing Education in Dentistry, 43(3), March 2022.
- Klein, M., & Waltuch, A. (2025, April 1). Converting a complete denture into an implant-supported provisional restoration: Simplified technique significantly reduces the time and expertise required and results in stronger, more esthetic prostheses. Inside Dentistry, 21(3), 20.
- Osteon Medical. (2020). Full Mouth Digital Implant Impressions – A new novel approach [White Paper].
- Auduc, C., Douillard, T., Nicolas, E., & El Osta, N. (2025). Fully Digital Workflow in Full-Arch Implant Rehabilitation: A Descriptive Methodological Review. Prosthesis, 7(4), 85.
- Straumann AG. 10 global trends in full-arch treatment and the opportunities they offer for you. 2020. Available from: Straumann website
- Legg, A., Kappatos, N., McCabe, J. F., & Barclay, S. (2023). Immediately loaded full arch implant rehabilitation and oral health-related quality of life: A retrospective cohort study from primary dental care. Clinical Implant Dentistry and Related Research, 25(6), 1103-1111. https://doi.org/10.1111/cid.13254
- Lan, R., Gul, M., Jiang, X., Wu, Y., & Wang, F. (2025). Long-Term Comprehensive Results of Four-Implant-Supported Overdentures and Fixed Complete Dentures: A Systematic Review and Meta-Analysis. International Journal of Oral & Maxillofacial Implants. Advance online publication. doi:10.11607/jomi.
- Lively, Terri. Digital Workflow: Staff Roles in a Digital Practice. Dental Products Report, September 13, 2022.
- Koutouzis, T., Ali, A., & AlRubaie, M. (2023). Clinical and radiographic peri-implant tissue changes for implants restored with convex or concave abutment shapes: A 3-year randomized controlled trial. Clinical Oral Implants Research, 34(7), 675-683. https://doi.org/10.1111/clr.14077
- Klein, M., Tuminelli, F. J., Sallustio, A., Giglio, G. D., Lerner, H., Berg, R. W., & Waltuch, A. (2023). Full-arch restoration with the NEXUS IOS® system: A retrospective clinical evaluation of 37 restorations after one year of follow-up. Journal of Dentistry, 139, 104741. https://doi.org/10.1016/j.jdent.2023.104741
- Giglio GD, Giglio AB, Tarnow DP. A Paradigm Shift Using Scan Bodies to Record the Position of a Complete Arch of Implants in a Digital Workflow. Int J Periodontics Restorative Dent. 2024;44(1):115-126. doi: 10.11607/prd.6733. PMID: 37552170
About the authors

Dr. Klein was a Clinical Associate Professor at New York University College of Dentistry in the Department of Periodontology and Implantology for 17 years. Dr. Klein is a Diplomate of the American Board of Oral Implantology/Implant Dentistry. He has pioneered the technology used in computer guidance for dental implant surgery and holds multiple patents for this technology.

Dr. Waltuch maintains an Implant & Restorative Practice in Cedarhurst, NY. His practice is focused on comprehensive digital workflows, fully guided surgeries and comprehensive digital full-arch restorations. He lectures and mentors on full-arch digital implant technologies and restorative techniques.