


Abstract
Stainless steel crowns or preformed metal crowns have become the standard for the restoration of primary teeth with extensive caries; however, they remain underutilized on permanent teeth. In this paper, we review the literature on the use of these crowns on permanent molars, and with the help of a case, discuss the indications, efficacy, and longevity of these crowns on permanent molars.
Since their introduction by the Rocky Mountain Company in 1947, Stainless Steel Crowns (SSCs), also referred to as prefabricated metal crowns, have become the standard of care for multiple surface restorations in primary teeth.1-3 Indications for the use of SSCs include: 1) large multi-surface dental caries or advanced erosion, 2) ideal restoration for primary molars after pulpotomy or pulpectomy, 3) as an anticipatory restoration in patients who are at high risk for dental caries, 4) teeth with developmental defects, 5) Teeth with extensive wear, 6) fractured teeth, 7) as an abutment for space maintainers, 8) in patients with limited cooperation, and 9) as interim restorations prior to placement of ceramic crowns. Despite controversies in the pediatric dental community regarding the extent of use of SSCs4 and the availability of newer more esthetic alternatives5,6, SSCs remain a popular and highly cost-efficient posterior restoration in primary teeth.3
Application of SSCs in permanent teeth dates back to late 1970s, with case reports outlining their use as a temporary or permanent restoration for mature permanent teeth and as an intermediate restoration for young permanent teeth.7 Many of the indications for SSC’s in primary molars also apply to permanent posterior teeth. SSCs have been used for restoration of structurally compromised vital permanent teeth, as well as an intermediate restoration for endodontically treated permanent molars.1, 8-11 They have also been suggested as the restoration of choice for preservation of tooth structure and vertical dimension in children with developmental defects of the teeth such as Amelogenesis imperfecta (AI), Dentinogenesis imperfecta (DI), or Molar Incisor Hypomineralization (MIH).11, 12
The traditional placement of SSCs on permanent teeth has been based on the idea that they would be replaced by a permanent crown once the occlusion has stabilized. Therefore, little research was done into the longevity of SSCs. However, more recent literature on SSCs placed in patients with special health care needs (SHCN), has shown that SSCs can last for an extended period.9, 13, 14 Considering this new evidence there is a need to assess the overall survival of SSCs and the consequences of leaving SSCs for many years.
Despite their advantages, the use of SSCs is often restricted to pediatric dentists, with general dentists often being hesitant to use SSCs in routine practice. The most reported reasons for this are a lack of information and training.3 There has been a recent interest in literature to revisit the use of SSCs in permanent teeth. These papers have looked at not only the use in young permanent teeth and first permanent molars; but also in second permanent molars, and as a permanent restoration in individuals with special healthcare needs.
The aim of this paper is to review the current status of the use of SSCs in permanent dentition, and with the help of a case study highlight their benefits as an intermediate restorative technique in permanent teeth.
Types of stainless-steel crowns
While the terms preformed metal crowns (PFM) and stainless-steel crown (SSC) are often used interchangeably, SSC is a type of PFM. There are also crowns such as Nickel Chromium crowns (ION) which are softer. In this paper we will focus on SSCs. There are several manufacturers of SSCs for permanent teeth, but the design remains the same between different brands with emphasis on a shallow occlusal anatomy.
Technique for placement of SSCs
Step 1 – Occlusal preparation
The occlusal preparation for a stainless-steel crown can be done using either a wheel diamond or a football diamond. Although the thickness of the stainless-steel crown is less than 0.5 mm, it is advisable to have an occlusal preparation of at least 1-1.5mm with minimal cuspal inclines to match the internal anatomy of the respective SSC. This means that the reduction at the cuspal tips is much larger than that at the fissures.
Step 2 – Caries removal
Following preparation of the occlusal surface, the next step involves excavation of caries and assessment of the pulpal status. Every effort should be made to remove caries conservatively in order to avoid exposing the pulp inadvertently. This is particularly the case in young permanent teeth with significant pulpal blood flow and a high chance of healing by tertiary dentin formation.
Step 3 – Pulpal assessment and treatment
If the extent of caries is approximating the pulpal tissue, then a pulpal protective agent containing Calcium Hydroxide or Mineral Trioxide Aggregate (MTA) should be considered. For caries excavation that does not result in a direct exposure of the pulp, the use of resin modified glass ionomer cement (e.g. Vitrebond) has also been advocated. In cases where the pulp is exposed the clinician is faced with the choice of a direct pulp cap, a partial or complete pulpotomy, or apexification if the tooth is no longer vital. Recent cost-benefit assessments have shown that in deep caries, the use of indirect pulp capping is perhaps the most cost-effective method and should be the treatment of choice to allow for continued apexogenesis. The details of pulp therapy in young permanent teeth are beyond the scope of this paper.
Step 4 – Proximal reduction
The stainless-steel crown needs minimal proximal reduction with a knife edge margin. It is important to ensure that after proximal reduction the mesial-distal width on the buccal is greater than the mesiodistal width lingually. This trapezoidal shape allows for an easier seating of the crown.
Step 5 – Buccal and lingual preparation
The buccal and lingual preparations in permanent posterior teeth are similar to the buccal and lingual bevels in primary molars, with no to minimal preparation of respective surfaces. This results in a highly conservative preparation and preservation of tooth structure.
Step 6 – Rounding off all line angles
Once the preparation of the tooth is complete, sharp margins and line angles are rounded to allow for ease of crown seating as well as elimination of high stress points.
Step 7 – Crown selection and try in
The selection of the SSC is an important step. There are different types of crowns available in the market, but broadly they may be classified as pre-contoured crowns or un-contoured (Unitek) crowns. In most cases, the gingival margins need to be trimmed with crown-cutting scissors, margins smoothed with a green stone, and margins contoured and crimped with appropriate instruments. Ideally, the crown is expected to fit with a “snap”. As the primary source of retention for an SSC is the malleability of the stainless steel, it is not necessary to eliminate all undercuts. This is particularly true for the buccal cervical bulge on the mandibular posterior teeth and the palatal bulge on the maxillary posterior teeth. Although this anatomical feature is not as prominent in permanent posterior teeth, it is still an important source of retention for SSCs.
Step 8 – Occlusion check and final cementation
Once the crown is seated the occlusion is checked. Given the soft nature of stainless-steel, multiple bites or biting down hard on a band-seater can help settle the bite. Once the patient is comfortable with the bite, the crown can be removed and cemented with a conventional glass ionomer cement. It is imperative to ensure the crown is not over-seated and potentially impinging on the biological width.
Case report
A 14-year-old patient presented with a large caries lesion on tooth #47, which was only partially erupted (Figs. 1A & 1B). This caries lesion and its rapid progression was most likely associated with a developmental defect in the tooth. Due to limited access and deep caries in this immature permanent molar, it was treated by conservative excavation of the lesion followed by indirect pulp therapy (IPT) using a Resin-modified Glass Ionomer Cement (Vitredond, 3M ESPE), and covered by an interim therapeutic restoration (ITR) with a conventional Glass-Ionomer Cement (Ketac Cement, 3M ESPE). The tooth was followed up regularly during recare visits (Figs. 2A and 2B). Following further development and eruption, the tooth was cleaned by second-stage caries excavation, and IPT (Vitrebond, 3M ESPE) placed, and restored with an SSC (Space Maintainers Laborary) cemented with Ketac Cement (3M ESPE), to provide optimal seal of all gingival margins (Figs. 3A & 3B). This was intended to be an interim restoration in this young patient, until further maturation of the pulp as well as completion of orthodontic treatment and facial growth. Figures 3 to 7 demonstrate the progressive stages of development and maturation of tooth #47. In this case, the patient elected to leave the SSC on tooth #47 as opposed to proceeding with crown lengthening and placement of lab-fabricated crown. Figure 7A is the most recent photo of this case, 21 years after the initial IPT and ITR treatment, and 16 years after the placement of the SSC on tooth #47. This case demonstrates the high capacity of pulpal healing in a young permanent tooth treated with conservative caries removal, IPT, ITR, as well as the longevity of SSC’s in patients with little to no attrition.
Fig. 1A

Fig. 1B

Fig. 2A

Fig. 2B

Fig. 3A

Fig. 3B

Fig. 4A
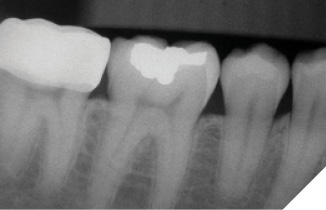
Fig. 4B

Fig. 5A

Fig. 5B

Fig. 6A
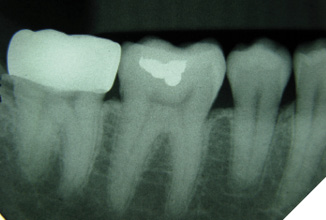
Fig. 6B

Fig. 7A

Fig. 7B

Discussion
Restoration of the young permanent teeth present unique challenges, primarily due to the fact that the pulp is still in a very immature state and that the occlusion is not yet fully established.4, 15 It is often suggested that the use of a permanent full coverage restoration be delayed until the occlusion is stabilized.16 There are several benefits to using permanent SSCs in these cases. SSCs offer a reliable full coverage restoration of teeth, especially endodontically treated teeth, reinforcing remaining tooth structure.12, 13, 17 They also offer an excellent option for teeth that have significant structural breakdown due to enamel hypoplasia or hypomineralization.11
The placement of SSCs requires an understanding of the concepts of how they are retained. The preparation of teeth for SSCs is fundamentally different from the preparation of the teeth for lab-fabricated crowns.15 SSCs require minimal preparation of the tooth, with a focus on preservation of tooth structure.1, 4, 15 SSCs are retained primarily by the mechanical locking of the crown to the undercuts on the tooth. The malleability of stainless-steel is responsible for the ability of the SSC to adapt to the shape of the tooth and to be inserted over undercuts. A pronounced cervical bulge is present on primary teeth, which is responsible for the characteristic “snap” fit of these crowns. Even though the respective bulge is significantly less prominent in permanent teeth, it is still important to preserve the buccal and lingual undercuts to optimize the fit of SSC’s. One exception to this rule is the presence of a large cusp of Carabelli on the maxillary permanent molars. The Carabelli cusp may need to be reduced to accommodate the shape of the crown and its fit over the tooth.
Longevity of SSCs in permanent dentition has been an area of interest in the dental community.2 Traditionally, SSCs were intended to serve as an intermediate restoration, allowing the occlusion to stabilize.2 However, there has been much published in recent literature about the use of SSCs as a permanent restoration for individuals with special healthcare needs under general anesthesia. There have been reports of these crowns lasting for several years, and recent literature suggests that, depending on patient’s dietary habits and occlusal forces, SSC’s placed in adults can be expected to last for up to 10 years.14, 16
In conclusion, whether used as an intermediate restoration in children and young adults, or as a permanent restoration in adults, SSCs can serve as a useful and durable restoration in several cases. SSCs in permanent teeth remain underutilized and it is important for dental practitioners to familiarize themselves with the technique for their placement. 
Oral Health welcomes this original article.
References
- Randall RC. Preformed metal crowns for primary and permanent molar teeth: review of the literature. Pediatr Dent 2002;24(5):489-500.
- Seale NS, Randall R. The use of stainless steel crowns: a systematic literature review. Pediatr Dent 2015;37(2):145-60.
- Uhlen MM, Tseveenjav B, Wuollet E, et al. Stainless-steel crowns in children: Norwegian and Finnish dentists’ knowledge, practice and challenges. BMC Oral Health 2021;21(1):190.
- Pinkham JR. Intraprofessional controversies: reflections on the stainless steel crown situation. ASDC J Dent Child 2001;68(5-6):292-3.
- Guduk OF, Sivrikaya EC, Yilmaz N, Baygin O, Tuzuner T. Is zirconium or stainless steel the most suitable crown material for less dentin stress in endodontically treated teeth? Technol Health Care 2022;30(5):1199-207.
- Lopez-Cazaux S, Aiem E, Velly AM, Muller-Bolla M. Preformed pediatric zirconia crown versus preformed pediatric metal crown: study protocol for a randomized clinical trial. Trials 2019;20(1):530.
- Croll TP, Castaldi CR. The preformed stainless steel crown for restoration of permanent posterior teeth in special cases. J Am Dent Assoc 1978;97(4):644-9.
- Kontham UR, Tiku AM, Damle SG, Kalaskar RR. Apexogenesis of a symptomatic mandibular first permanent molar with calcium hydroxide pulpotomy. Quintessence Int 2005;36(8):653-7.
- Discepolo K, Sultan M. Investigation of adult stainless steel crown longevity as an interim restoration in pediatric patients. Int J Paediatr Dent 2017;27(4):247-54.
- Bandeira Lopes L, Machado V, Botelho J. A Four-Year Follow-Up Case Report of Hypomineralized Primary Second Molars Rehabilitated with Stainless Steel Crowns. Children (Basel) 2021;8(10).
- Bandeira Lopes L, Machado V, Botelho J, Haubek D. Molar-incisor hypomineralization: an umbrella review. Acta Odontol Scand 2021;79(5):359-69.
- Alfarraj JH, Alsaeed AA. Clinical Management of Molar Incisor Hypomineralization Affected Molars in a Pediatric Patient Including Endodontic Treatment, Case Report and Review of the Literature. Clin Cosmet Investig Dent 2022;14:183-89.
- Munoz-Sanchez ML, Linas N, Decerle N, et al. Radiological Evaluation of Stainless Steel Crowns Placed on Permanent Teeth in Patients Treated under General Anaesthesia. Int J Environ Res Public Health 2021;18(5).
- Chaipattanawan N, Chompu-Inwai P, Nirunsittirat A, Phinyo P, Manmontri C. Longevity of stainless steel crowns as interim restorations on young permanent first molars that have undergone vital pulp therapy treatment in children and factors associated with their treatment failure: A retrospective study of up to 8.5 years. Int J Paediatr Dent 2022;32(6):925-37.
- Croll TP. Preformed posterior stainless steel crowns: an update. Compend Contin Educ Dent 1999;20(2):89-92, 94-6, 98-100 passim; quiz 06.
- Sigal AV, Sigal MJ, Titley KC, Andrews PB. Stainless steel crowns as a restoration for permanent posterior teeth in people with special needs: A retrospective study. J Am Dent Assoc 2020;151(2):136-44.
- Grizzo IC, Bisaia A, Di Leone CCL, et al. Revisiting the use of stainless steel crowns for treatment of molar-incisor hypomineralization: a case series. Gen Dent 2022;70(5):62-66.
About the Authors

Dr. Nouri is a Certified Specialist in Pediatric Dentistry and works at PDG Pediatric Dental Group in Vancouver and Delta, British Columbia. He is a clinical associate professor at the Faculty of Dentistry at the University of British Columbia. He has authored several papers on clinical pediatric dentistry and is focused on the transfer of scientific principles to clinical practice.

Dr. Pani is a Certified Specialist in Pediatric Dentistry, and the current president of the Canadian Society for Disability and Oral Health. He practices in London, Sarnia, and Port Elgin, Ontario. He has over 50 peer-reviewed publications in pediatric and special care dentistry.