


This paper is written from my perspective as a “wet-fingered” GP engaged fully in private practice. As dentists, our technical excellence involving hand-eye coordinated skills is highly valued and therefore often our primary focus throughout the educational process and in daily practice. This is one foundational pillar for efficacious care. A second pillar is a dentist-patient relationship based on honesty. It is a core feature of healthcare. Our governing bodies dictate with great specificity how we are to conduct ourselves. However, the honest conduct from the patient goes unregulated. Here I am not concerned with paying fees on time or keeping appointments, or making claims of improved hygiene homecare when clinical findings suggest the contrary. Instead, I wish to focus on the patient’s honesty, or accuracy, in reporting of symptoms and histories, on which we as dentists are to formulate and provide treatment.
Efficacious treatment requires an accurate diagnosis. Without it, treatment is worthless at best if it is noninvasive or dangerous at worst once we pick up a drill or scalpel. Critical to defining an accurate diagnosis are honest and accurate statements reported by the patient. I will not dwell on patients that are lying volitionally, such as those seeking drugs. After a few go-arounds, we can typically spot these bad actors. Case 1 focuses on a patient who reports pain or discomfort which they believe is “real”, but may in fact be rooted in a psychiatric disorder. A second case will focus on confusions due to odd and poorly-defined manifestations of an organically-based neuralgia that was mismanaged by this author, me. A third case is presented which combines both aspects: The presence of neurogenic pain, coupled with a psychosomatic contribution. It is important to bear in mind that pain and discomfort of psychosomatic origin is as real as it gets for the patient and cannot be dismissed as being somehow pretended! However, oftentimes when such complex cases present, their identification, which hopefully would lead to successful treatment, can seem to be almost impossible! Some such cases are broadly classified as Somatization Disorders (SD), in which Somatic Symptom Disorder (SSD) is grouped. Thus, the title, “SD-SSD: Treating the Untreatable”.
I stress to the reader that I possess no formal training in neurology, psychology or psychiatry. Hence my use of psychological and psychiatric terminology and classifications may be lacking appropriate rigour. These are case reports that I have “fallen into”. Those of you having similar experiences will appreciate that “fallen into” is an appropriate description. The first indication of such cases is when “things just don’t add up” in a typical manner. Dental problems are not vast in number. We typically triage obscure presentations as to those of dentoalveolar origin or not and hope it is the former for which we have solutions and treatment. If it is the latter, then we are in an arena where important questions not asked or subtle clues not recognized can result in a failure to diagnose accurately. For these reasons, it is best to refer these cases to those better trained and motivated to solve mysteries. Unfortunately, these clinicians are a rarity as they “must love a mystery”. Here is an example.
CASE 1
A middle-aged female presents with numerous cutaneous and mucosal lesions, that appear to be erosive, accompanied by itching and burning sensations. (Fig. 1-6)
Fig. 1

Fig. 2

Fig. 3

Fig. 4

Fig. 5

Fig. 6

The patient reports no other systemic findings, but did present with a small plastic bag which contained samples of skin tissue that she peeled away. In my long career, I have come across various forms of muco-cutaneous lesions involving autoimmune and/or hematological disorders. I feared these might be present and hence referred the patient to an oral pathologist in a hospital setting. Before COVID, it was possible to have a patient seen quickly. Within days, I received a call from the oral-pathologist. “She has Ekbom’s Disorder”. Here, I boast that I received an A-grade in pathology from Dr. James Main (department head) back in the mid 70’s, but I fail to recall hearing about Ekbom’s. I recall names such as “Ehlers-Danlos”, and vaguely know it as some connective tissue disease. That is to say, I recall being exposed to rare pathoses at school and continuing educational seminars, but not Ekbom’s. “What is it?” I ask. “Delusional parasitosis” is the reply. These unfortunate patients are convinced that they are infected with parasites originating from under the skin, hence they pick and scratch and “excoriate” skin, and in this case, the oral mucosa.
From Wikipedia…Nearly any marking upon the skin, or small object or particle found on the person or their clothing, can be interpreted as evidence for the parasitic infestation, and individuals with the condition, commonly gather such “evidence” to present to medical professionals. This presentation is known as the “matchbox sign”, “Ziploc bag sign” or “specimen sign”, because the “evidence” is frequently presented in a small container, such as a matchbox. The matchbox sign is present in five to eight out of every ten people with DP.
A thorough discussion of Ekbom’s Disorder is beyond the scope of this paper. The point I stress is that I missed the “Ziploc bag sign” because I was unaware of it. In my third decade of practice, I was totally caught off guard. As dentists, we are well trained and practiced to detect disease in teeth and gums, but poorly trained to detect paranoias and the vast array of other psychiatric manifestations that affect our ability to obtain an accurate diagnosis in these cases.
There exists a philosophical truism: The incorrigibility of first-person reports of sensation. Here, incorrigibility means the inability to verify with certitude a statement made by an individual when they report a felt “sensation”. Ironically for us, it is often explained in dental terms and goes something like this:
Mr. Smith reports a sensation: “I (first person) have an excruciating pain in my right lower jaw”. How can this report be verified, given the fact we do not have direct access to Mr. Smith’s mind? To appreciate this fully, I ask the reader to ponder the following: With respect to the contents of your own mind, it can only be reached by you. You share your thoughts with others by way of verbal and written language and forms of non-verbal communications; perhaps tears and grimacing when a severe toothache is present. A child may whimper. Thus, when someone claims publicly “I feel pain”, we understand that although there may be deception or self-deception, that person does have the last word on their experiencing pain.
This brings me to another guiding principle of providing care. A patient must always be given the benefit of the doubt when reporting sensations. The case above is obviously an exception to this rule, but her distress is “real” and not faked. It may be based in brain chemistry gone awry. There are times when sources of discomfort are obscure or neurological, or referred, or not readily resolvable with imaging and we clinicians are initially uncertain of the source. In those instances, we must always ask ourselves, “What am I possibly overlooking”? These cases will require a second or third review and perhaps a second set of eyes. As dentists, we must be keenly aware of our knowledge limitations and refer to appropriate specialists. Even with this in mind, it is not difficult to “fall into a problem case” with the best of intentions. Here is an example of my doing so.
CASE 2
In 1998, a patient of record presents with a typical complaint we hear every day: “I have intermittent discomfort in the right side of my mouth, along with some sensitivity to cold”. At that time, I was in my 19th year of practice and my clinical experience supported a self-confidence in my ability to pick an offending tooth in obscure situations and successfully provide endodontic therapy.
The radiograph (Fig. 7) shows heavily restored teeth in the first quadrant. My records reveal several appointments of varying length, which transpired before selecting tooth 15 for pulpectomy. The patient returned shortly stating discomfort was reduced, but still pain to cold. Endo was started for tooth 14 and both bicuspids were completed. The patient reported she felt better, but still not totally asymptomatic. Some weeks later, the patient returned once again with a similar complaint to cold and ill-defined discomfort. At this point, I recalled a lecture by Dr. Main. “One day you will provide endodontics for what appears to be thermal cycling problems and succeed in reducing discomfort. Then another tooth, and another one and after all the teeth have been endodontically treated, the problem will still be present. At that point, you will realize a neuralgia of some form is present.” I informed the patient of this story prior to initiating further treatment. I asked if she had the classical presentation I was aware of … trigger points on the face innervated by this nerve. She claimed no, just an issue with vague pain of varying intensity made worse by cold water. Furthermore, she expressed anxiety about having a neuralgia and we agreed to do endodontics for the first molar and sure enough the last molar as well.
Fig. 7

I wish to stress the following point. I recall a mental struggle within myself. “I wanted the endodontic therapy to relieve the symptoms not only for reasons of vindicating my skills, but because I hoped to spare her the experience of the “neurological treadmill”. This consists of attending numerous specialists, undertaking various imaging, finding nothing definitive and ending up on drugs that potentially result in one feeling wonky for most of the day. Thus my statement; even with the best of intentions, one can “fall into a problem”.
Please appreciate that treatment was done not out of ignorance or monetary greed. Endodontics was done based on mutual hope shared with the patient to solve a problem mechanically; a dentist’s treatment bias.
After a time, the patient returned complaining that cold was no longer a stimulant to pain. The discomfort was now more frequent with spontaneous onset. I informed her it was time to meet Dr. Main. Arrangements were made for an appointment and Dr. Main graciously agreed that I could be present, in that I might learn by observation. What had I missed? What tests are required? What questions did I not ask? His one request is that I sit quietly in the corner and say nothing until he was done. During their conversation, I thought the patient answered a question incorrectly and I spoke up. Dr. Main turned to me, glowered, pointed his finger at me and gave me a stern “Shush!” (which evidently is burned into my memory).
There came the realization I had not considered or interpreted more correctly, the answers from the patient that are referenced to guide more probing questions to suggest the correct diagnosis. Furthermore, I realized that a clinician must be immersed in these sorts of problems in order to tease out all the subtleties of neurological conditions. As general practitioners, we must determine if discomfort is demonstrably dentoalveolar in origin. This can be difficult as pain perception and appreciation are an exceedingly complex phenomena and it is easy for both dentist and patient to be fooled.
The patient did encounter the “neurological treadmill” as stated above, that included medications to help with control of pain with varying degrees of efficacy. Finally, a successful outcome was achieved neurosurgically by wrapping a Teflon barrier around a vascular structure that was impinging on the Trigeminal Nerve as it exited the foramen ovale. Hearing was lost on the affected side, and yet the patient was most pleased to be rid of the pain that eventually had become unbearable, along with the classical trigger-points of jolting pain. The patient’s honesty and co-operation was paramount in providing treatment.
Above are images of the endodontically treated teeth with crowns placed 25 years ago. (Fig. 8 & 9) This brings me to another foundational tenet of patient care: All treatment must be carried out to a high standard. Particularly in this case, which was initially misdiagnosed. First, because treatment should not cause secondary problems. And second, our governing College may hopefully be more lenient should a complaint arise.
Fig. 8

Fig. 9

I relay the above case to highlight a quote by the late Dr. Simon Weinberg, a highly respected oral and maxillofacial surgeon and educator.
“Good judgment comes from clinical experience. However, good clinical experience comes from bad judgment.”
A most eloquent way of saying we learn best from our mistakes. My clinical judgement improved as a result of these cases, as I hope the reader’s does vicariously, which is the point of these clinical reports.
Now consider combining aspects of both these cases into one. Reports of protracted and ill-defined sensations of pain, coupled with patient reports that are at times, incomplete, inaccurate and possibly confabulated due to some psychological contribution.
CASE 3
Recall my description of “falling into a problem”. Sometimes, we are pushed. I returned this past February from my first vacation since COVID. The second day back, I receive a phone call from a colleague asking for a favour. “Paul, I hate to ask this of you and apologize for doing so, but I will be away for a month and need you to look after a patient. He has severe pain from possible trigeminal neuralgia. He has seen “Every Big Name” in the city and no one has been able to help him. I am worried about him as he has lost 40 pounds of weight because he cannot chew food due to the excruciating pain. If he calls you, just give him a mandibular block on the right side so he can eat a meal. Are you willing help?”
Those that know me, appreciate I will never say no. A brief history is relayed to me along with the details of dental and medical facilities and specialists previously involved in this case, some of whom I know. I asked my colleague to send clinical records, to best prepare myself. (Unfortunately, this was not done). My colleague ended the call with, “hopefully he won’t call”. That was on a Wednesday. On Friday morning, the patient’s wife called (the patient was in too much pain to speak) and an appointment was scheduled during lunch, as the day was booked. A call was made to the referring office for any records or images, but that office was closed. Attempts to contact the previous specialists proved unsuccessful. I realized I must “go in blind”.
My initial goal was as follows: Treatment must be underpinned and directed by an accurate diagnosis. I have been asked to provide local anaesthetic, which is invasive treatment. Before this is to be done, I need to satisfy myself, and possibly our College one day that some due diligence was carried out to determine if the injection of local anaesthetic was indeed justifiable. Hence some examination must be undertaken. An 80-year-old gentleman presented, tall and thin, unshaven, messy hair and looking quite frail. His wife attended in the operatory claiming her husband could not speak due to pain and that she would answer for him. It was their understanding that I am to administer local anaesthesia.
I am in my 45th year of full-time solo practice. My eyes have seen much and I am no longer surprised or intimidated by anything unusual and have learned to keep calm during stressful situations which allow me to carefully observe body language. Such observations as the degree of eye contact while conversing, the grimacing of lips, the clenching of hands, overall body posture, complexion and dress, are non-verbal clues that add to what is spoken. These subtle clues are not listed in textbooks or formalized treatment flowcharts, but are gleaned by decades of treating patients with every imaginable malady. We are supplied with sense data every moment when we engage with a patient; the key is attentive observation. I care not about a missed lunch, or running late or inconvenienced staff or time spent for which I may not be remunerated. The goal is to miss nothing.
On the flipside, we should pause and be mindful as to the body language we as healthcare providers are projecting to the patient. Do we make eye contact? Are we sitting at the edge of our seat, seemingly ready to bolt? Is one’s speech calm and measured, as opposed to rushed and frustrated? Are staff constantly interrupting? Patients are affected by our non-verbal cues as well. My intention is to project the following: “Dear patient, you have my full and undivided attention”.
I asked him if he wished his wife to remain with us. He gave a noncommittal, almost agitated wave of the hand, which I noted. He then pulled out a crumpled sheet of paper with poorly handwritten notes. I read scattered lines. “15 years living with pain”, “Trigeminal Neuralgia suspected”, “losing weight”, “need local so I can eat”, along with other short statements that were all confusing as there was no associated chronological order. His writing became hastened and illegible. I provided the patient with a clean sheet of paper on clipboard and a pen. I stated that I will ask questions that he is to answer. I asked his wife to leave the operatory on the pretense of “taking X-rays”. Alone, I was now able to focus solely on the patient. I asked the typical questions.
Q: Where is the pain coming from?
A: All over.
Q: Both right and left?
A: Yes, but mostly right.
Enquires were made on duration, intensity, spontaneity, etc. As previously stated, I lack formal training in oral pathology. I record his answers, but this is secondary. My primary intent was to establish an interpersonal connection with The Man. I wanted him to sense that I am competent, thorough and empathetic, as after all, I was about to stab him with a needle in an area that he claimed is too painful to allow for speaking. At some point, he may have reached a moment of frustration as he stopped writing answers and started speaking. How is it that at one moment, speech was impossible and now it is the opposite? I missed nothing.
During our conversation, he claims to have had an endodontic consultation with Dr. Gary Glassman (an editor of this journal), where imaging was undertaken. I interrupted the patient and called Dr. Glassman from a phone in the operatory as I intentionally wanted the patient to witness this. Mercifully I get a live receptionist straight away. She is informed of my need to get information as expeditiously as possible and I asked to speak with Dr. Glassman. Unfortunately, he was demonstrating at the Faculty of Dentistry at the University of Toronto. I instructed her to send records immediately to my office and to Dr. Glassman, with a note to call me ASAP as the patient is in the chair. Within minutes I received a few radiographs and a 3D radiology report giving me some clue of his dentition, as up to this point, I had made no attempt to touch the patient’s face.
Most importantly, Dr. Glassman did call me from the faculty in short order as requested. He recently consulted with the patient in order to assess a possible endodontic contribution. None was found. Via a voice conversation, he offered additional insight on patient management and for this, I remain forever grateful.
The patient appeared to be no longer grimacing in pain and spoke without difficulty. Physically, he appeared more relaxed. I asked him if I might take a peek at his teeth and gained consent. As I approached his lips on right side with a mirror, his head moved away which I interpreted as non-verbal communication…”Please don’t hurt me”. Finally, I get a mirror in and pry his lips apart as gently as possible and discover a full dentition covered in a thick accumulation of debris for lack of tooth-brushing.
The marginal gingiva is inflamed and bleeds easily on gentle probing (Figs. 10, 11 & 12). His eyelids are squeezed shut and his hands are clenched. The mirror is removed and he is informed that I will administer local anaesthetic before investigating further. The patient is shown a cotton swab and this time when I parted his lips, his eyes, head and hands are more relaxed than before. I surmised that if pain while speaking was a trigger, then the jab of the needle tip would be far worse. I slowly inserted the tip of the needle and noticed no bodily reaction; not even a small flinch that might be expected from an average patient. I missed nothing.
Fig. 10

Fig. 11

Fig. 12

Three carpules of 4% Articaine containing 1:100,000 epinephrine were administered in the upper right quadrant from cuspid to second molar. After a few moments the patient claimed all his pain was gone, both right side and left side, all to my surprise. I was under the assumption that pain from a central neurological source is not typically alleviated by local anaesthetic. Also note that I had forgotten that the referring dentist asked for a block injection for the lower arch, whereas I administered infiltration in the upper arch because of the ease of doing so. I had planned on a lower block, but concluded why bother if this infiltration sufficed. The patient has been historically focused on pain coming from two previously endodontically-treated teeth in the lower arch, 46 and 45. With the local anaesthetic in place, he claimed that pain was currently not present. Large composite resin fillings are present in teeth 47 and 48. A strong blast of air and water elicited no pain response, nor did percussion of any of the teeth and biting on a cotton roll.
As noted, there was no longer any pain from the left side after the right side injection. This finding is important from a neurological perspective as pain does not refer from the left to the right side. Simply put, never treat a tooth on the left side to alleviate pain on the right side. This finding alerted me to a possible psychosomatic contribution. Or in hindsight, he may have initially claimed pain from “everywhere” out of frustration of being asked this question countless times in the past. As stated in the opening remarks, everything reported by a patient must be considered, particularly confabulations, to aid in solving confusions. Now absent discomfort, consent was gained to obtain films and photographs. The patient was most comfortable and in fact became quite chatty: A complete 180 from moments before.
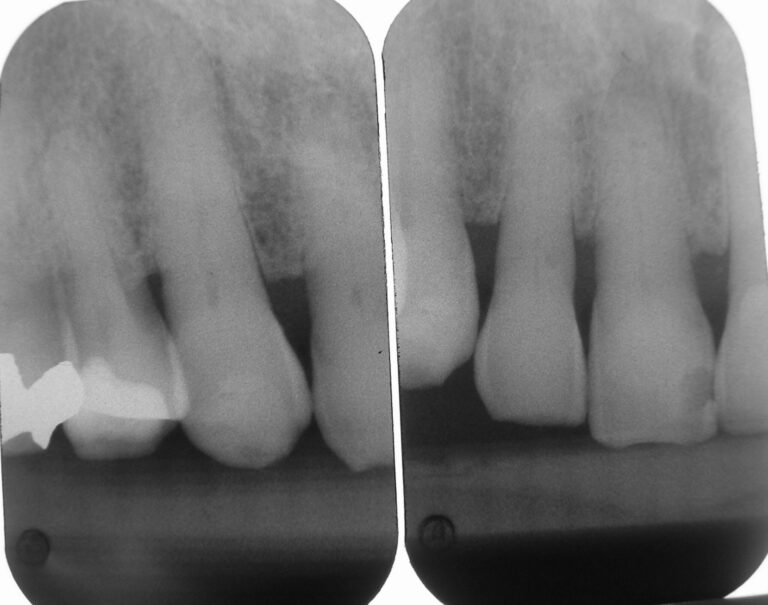
The films revealed an intact dentition with several restorations, all seemingly serviceable. All the teeth not anaesthetized were tested with prolonged air-water spray and proved unresponsive. The films (Figs. 13-18) revealed no periapical disease; except for a possible lesion over tooth 27, which was confirmed by the aforementioned 3D scan. Biting and percussion tests were negative and probing depths did not indicate a root fracture. Photographs were taken and reviewed with the patient. He was informed of the accumulation of plaque and consented to dental prophylaxis. To accomplish this, lips are stretched and pulled. I intentionally polished aggressively with a dry rubber cup to generate some heat on certain teeth with large restorations to test for discomfort to heat. Throughout treatment, he remained totally comfortable, co-operative and pleased. Something I did not anticipate on initial presentation.
Fig. 13

Fig. 14

Fig. 15
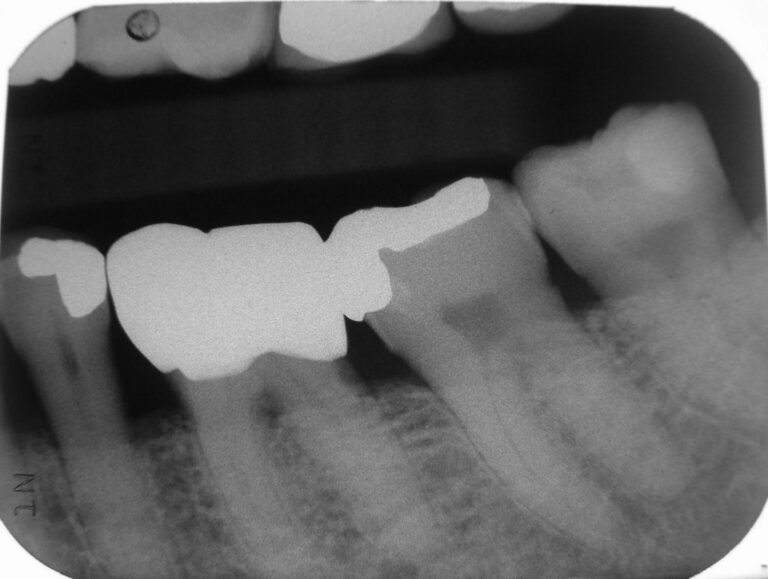
Fig. 16
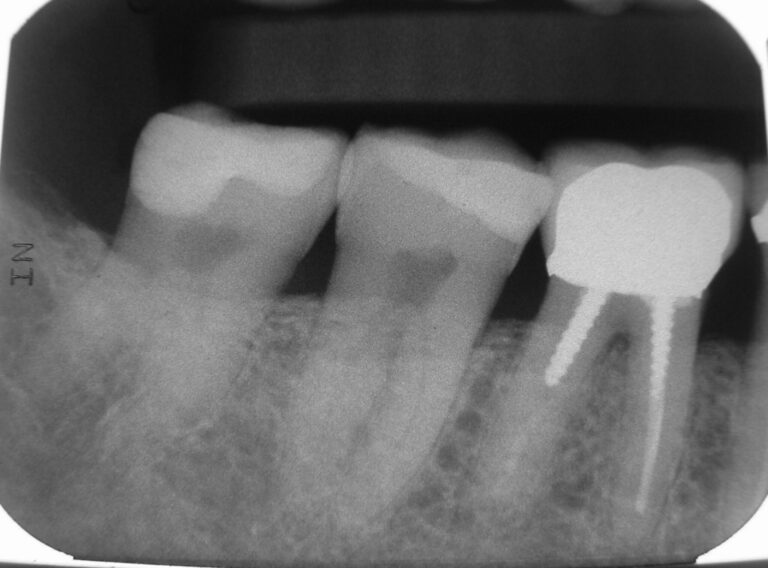
Fig. 17
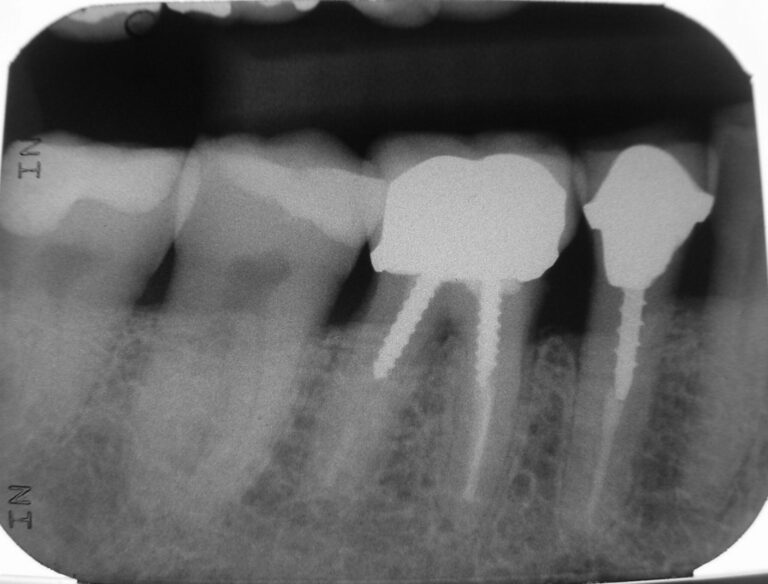
Fig. 18
I informed the patient of his inflamed gums and applied Prevora, a topical coating of 10% chlorhexidine that is to remain on the teeth for a couple of days and thus instruction was given to not brush for the next 2 days, which he claimed is a no-brainer as the act of brushing was painful. This high concentration chlorhexidine (10%) coating is a most effective antimicrobial agent that can be most efficacious in patients who cannot carry out proper homecare as a result of physical disability or mental challenges (e.g., dementia related).1,2,3,4 In this particular case, these are not present, but the struggle to avoid pain posed an obstacle to routine brushing.
Up to this point, I had spent 90 minutes with this gentleman and one hour had passed since local was administered. From all appearances, we seemed to have connected and he was quite comfortable to continue reviewing possible causes for his unbearable pain these past 15 years. I informed the patient that I am 30 minutes late for my next patient and his time was up. Another couple of carpules of local were given, which should have allowed enough time to have an uneventful lunch. In addition he was given my personal cell, which every one of my patients have and is instructed to call 24/7 should the need arise. He was rescheduled on the next Friday for reapplication of Prevora, as 3 coats one week apart, is the accepted protocol. In addition, he was informed that I hoped to have information from the other clinicians he has seen in order to gain more insight. On departing, he gives me a lopsided smile (due to the local), a long handshake and gracious thanks, all with direct eye contact. We connected.
During the remainder of the day, while treating routine problems, my brain was free to dwell on this case. I have encountered cases in my 45 years where psychosomatic problems were a contributing factor and classify these as fascinating and frustrating with equal measure. Fascinating, because the intricacies of pain perception and pain appreciation are complex and mysterious. Unfortunately, this mysteriousness frustrates both patient and clinicians in providing treatment. Before Friday’s end, came the realization that I have homework on the ensuing weekend.
I was able to share this case with colleagues having more experience with fascinating and frustrating cases. The mystery in my mind was: can there be an organic cause for constant excruciating pain, claimed both left but predominately right, that is completely alleviated by an injection in the 03 sextant? Is some neuralgia present that can cause some “true” level of discomfort for the past 15 years that the patient now over-exaggerates to the point that it has overtaken his life? A suggestion is put forth to pretend an injection, or better yet, inject saline – to try a placebo injection. On the following Monday, the patient’s wife called again. Another injection is requested and again during our lunch hour. Prior to the patient coming in, I received a follow-up call from the patient’s physician working in a pain clinic. I was given additional valuable information. Imaging suggested a trigeminal neuralgia was suspected but not conclusive. Or it may be conclusive, but treatment options were less so. I informed the MD that I planned to try a placebo injection. He himself provides anaesthetic injection, but over the past 4 years that he has been attending to this patient, he has not done so. I asked why not? What have you done for this individual? He claimed the patient comes in frustrated with paper notes in hand and they talk for a bit. Suggestions are made with regards to medications and possible surgical intervention and the patient leaves claiming he will think about it. This sounded eerily similar to my appointment. The physician asked that I report back with results of the placebo injection.
At lunch, the patient presented and requested local anaesthetic so he can eat lunch comfortably. Without much fanfare, topical anaesthetic was applied and a carpule containing saline is injected over teeth 15 and 16. This is followed by a quarter of a carpule of Carbocaine Plain over teeth 12 and 13 in order to promote a feeling of numbness in the upper lip and the few drops were dripped on the tongue to reinforce the experience of receiving true local anaesthetic. Several minutes passed and a claim is made that the pain is much reduced. I asked if I might prophy the teeth once again to apply Prevora and gained consent. I addressed the upper left quadrant first and then the lower left. As I approached the midline, the patient started to squirm ever so slightly. I asked if pain is present and he claimed “a bit”. I informed the patient that he may need a follow-up injection and administer 2 carpules of 2% lidocaine 1:100,000 epinephrine. Within some minutes I resumed prophylaxis of the teeth without any discomfort. The conclusion I drew was that there may be an underlying organic reason for pain perception but there is a significant psychosomatic contribution to his pain appreciation.
Additional photographs were taken with lip retractors and large mouth mirrors without any complaints. Figures 19, 20, 21 and 22 show that the biofilm is much reduced along with the level of gingivitis. He claims to have tried to brush more frequently as he had undergone periodontal surgery some years ago.
Fig. 19

Fig. 20

Fig. 21

Fig. 22

On this day he was more animated; we traded old comedic jokes and one-liners in our shared Mother Tongue. I understood the pain relief I provided is transitory in nature, but at least he gets a few hours of reprieve before the anaesthetic solution dissipates. I mentioned that a shave and haircut might be in order. This initiated his stories of his old barbers and how he misses them, as do I. This was not a conversation I would have expected from someone claiming to be in excruciating pain. At a subsequent appointment, he arrived looking better shaved and hair combed. Trust is affirmed and he leaves happier than when he arrives: Minor victories.
He was seen a week later for third application of Prevora and the administration of local anaesthetic. The appointment is short and sweet and his gingival tissue remains much improved. However he claims his pain is ever present to varying degrees.
Later, a report is received of an MRI taken a couple of years ago. It states the “The right superior cerebellar artery exerts mass-effect on the root entry zone of the right trigeminal nerve.” So indeed, there is imaging to support trigeminal neuralgia (TN). Reports filter in from the “Big Names” that have attended to this gentleman. These reveal a clearer history that various medications recommended for TN have been tried several times by several different clinicians; starts and stops. He has been offered surgery, but as of yet, has declined due the various risks and lack of a guarantee that his symptoms will be alleviated. In fact, they may be worsened. It may be that these prior clinicians have become frustrated with a patient that procrastinates on decision-making and fails to follow advice.
SOMATIC SYMPTOM DISORDER (SSD)
What is lacking from the reports I have in hand, are comments of possible psychological/psychiatric repercussions on pain appreciation -ideation of pain, by 15 years of chronic pain that has been sensed – real pain stimulus.
I have had the misfortune of treating others with psychosomatic issues that were downright mean and abusive. In these instances, a caregiver must demonstrate calm composure which is difficult at first, but easier with experience. One must realize that a suffering individual may become irrational at any point. Contrary to this, I truly enjoy this patient’s company thus far and hope his level of co-operation remains a constant.
“Psychosomatic” is a very broad term we dentists may use to label someone with a problem we think is “in their head”. There is a more exact term I wish to introduce. I have dealt with patients suffering Somatic Symptom Disorder. Here is a brief description from psychiatry.org:
Somatic Symptom Disorder is diagnosed when a person has a significant focus on physical symptoms, such as pain, weakness or shortness of breath, to a level that results in major distress and/or problems functioning. The individual has excessive thoughts, feelings and behaviors relating to the physical symptoms. The physical symptoms may or may not be associated with a diagnosed medical condition, but the person is experiencing symptoms and believes they are sick (that is, not faking the illness). A person is not diagnosed with somatic symptom disorder solely because a medical cause can’t be identified for a physical symptom. The emphasis is on the extent to which the thoughts, feelings and behaviors related to the illness are excessive or out of proportion.
In treating this kind gentleman, I must consider whether SSD is a contributing factor. Not because I am able to provide “a cure” so to speak, but to be supportive and empathetic while providing dental-care. Ideally, I desire to somehow have him realize that some form of mental health counselling would be beneficial, without reinforcing a false narrative that the pain is “all in his head”. Making this false claim will assuredly destroy the trust I have laboured to establish.
Here is more from psychiatry.org5 (emphasis supplied):
- Treatment for somatic symptom disorder is intended to help control symptoms and to allow the person to function as normally as possible.
- Treatment for somatic symptom disorder typically involves the person having regular visits with a trusted health care professional. The physician can offer support and reassurance, monitor health and symptoms and avoid unnecessary tests and treatments. Psychotherapy (talk therapy) can help the individual change their thinking and behavior, and learn ways to cope with pain or other symptoms, deal with stress and improve functioning.
- Antidepressant or anti-anxiety medications can be useful if the person is also experiencing significant depression or anxiety.
I stress once again that I am not an oral pathologist, neurologist, or psychologist-psychiatrist – only a caring GP dentist. In my long career, I have witnessed family, friends and patients deal with obscure illnesses. I have witnessed a family member being told by a neurologist that their symptoms of not “feeling-self” and dizziness were due to anxiety and given the perfunctory scrip for Valium, only to be diagnosed with MS some years later when symptomatology became more pathognomonic. From these experiences, I have developed compassion to deal with these unfortunate individuals. Here is where I define my place in these cases. In the above treatment for SSD outlined from psychiatry.org, I had made bold face some statements that I will now discuss.
A trusted health care professional: This is first and foremost in my dealings with any patient. Trust is delicate. It may take a moment to acquire, but it takes a life-time of constant effort to keep, yet can be lost in an instant, sometimes by events or actions remote from us. I need this gentleman to trust me. Possibly he feels a need to grant trust. This is foundational in a caregiver-care recipient relationship. It took me near 30 minutes before he would allow me to peek past the lips. For the life of me, I could not demand: “Your dentist wants me to freeze your mouth … now open wide and don’t move, because it’s my lunchtime.”
Avoid unnecessary tests and treatments: I am under no illusion that providing treatment and guidance for neuralgia is well beyond my paygrade. From case #2, I have learned caution. The application of Prevora is to help reduce the gingival inflammation present that might be a contributing factor to pain stimulus in this case with a low pain threshold. The injections may somehow downregulate the initiation of pain (was told this by my “brain-trust” colleague and the patient’s pain physician). If nothing else, there is the intent to reduce the biofilm that promotes periodontal breakdown and tooth decay, because the last thing this patient needs is invasive dental treatment. So dear reader, I did have a method from the outset.
Talk therapy: This is coextensive with gaining trust. The more one talks, the deeper the trust. The deeper the trust, the more one talks. My intent during this first meeting with the patient was to establish open lines of communication in order to harvest as much information as possible on which to rule in or rule out possible pathologies on which to plan treatment. My conversations with the patient will never touch upon possible psychological-psychiatric issues. From nearly half a century ago I recall the words of Dr. James Main: “The clinician best suited to provide a diagnosis of illness is the one that will treat it”. This was in relation to cancer. As dentists, we may make a mistake. Even with a conclusive pathology report in hand, the dentist is ill-equipped to guide a patient through a difficult diagnosis and treatment options that will be asked by a distraught individual. This applies to psychological-psychiatric issues, of which we may have strong suspicions, but we are not experts in this field. My advice to a patient that I believe is suffering from ideational problems is to have them discuss their symptoms with their physician and investigate if counselling of a sort might be beneficial. I will then transfer my specific concerns to the physician separately. I never mention Somatization Disorder to a patient as I am not the one who will diagnose or treat it.
CLOSING THOUGHTS
So there you have it, “Treating the Untreatable”. For those like myself with no special training is this field, there are no great hidden pearls to offer other than the following.
At first, if things just don’t add up, stop and endeavour to not provide irreversible treatment. Openly discuss confusions that are present before you act. Prior to acting, these are viewed as valid reasons for difficulties. Afterwards they appear as poor excuses.
- Slow down and set aside a sufficient amount of time.
- Seek help from more experienced clinicians.
- If a referral is made, stay involved with the case, even at arm’s length. This will add to your clinical experience the next time around.
- Recall the incorrigibility of first person reports of sensation. A patient must always be given the benefit of the doubt on their reports of symptoms.
- With Somatization Disorders, the appreciated pain is real for the patient.
Our task is to attempt to somehow verify these symptoms and to acknowledge them as opposed to being skeptical of their presence. Worse is demonstrating a dismissive attitude, which results in the loss of trust and the patient. Then again, some may see this as a successful strategy to divest oneself of a problematic patient, but not one I would support. It is demeaning and grossly unprofessional.
Take time to establish trust as best as possible. My clinical experience informs me that a patient is more likely to forgive missteps if trust is present. For young clinicians, be patient as this skill develops with maturity and clinical experience.
Remain supportive of the patient. Recall, “there but for the grace of god, go I”.
Practice with a good measure of Compassion and Humanity.
I end with a graphic courtesy of Dr. Brian Darvell. (Fig. 23)
Fig. 23
It attempts to convey the three foundational aspects of healthcare. First there is Science, which defines core principles and protocols of healthcare that are based on evidence-based knowledge. This is readily available to us all. Second is Art, the skill and dedication to detail a clinician demonstrates in carrying out the Science of their given field of endeavour. This in some regard is less egalitarian, given the genetics involved in manual dexterity and hence some are more “gifted” than others. Nevertheless, one can choose to perform to the best of one’s abilities by continual vigilance and effort. There is also the Art of nontechnical skills, such as diagnosis and patient management and communication, which improves with experience if one is mindful of it. Third is a concept rarely discussed in technical papers; the Humanity of dental care, which is a measure of the degree of compassion a dentist demonstrates while undertaking the Science and Art of their discipline. In this particular case, compassion was demonstrated by a willingness to devote time, regardless of inconvenience, to connect personally with a suffering patient (not client!) and thus provide some assurance that the guy in the white clinical gown cares for their wellbeing, despite being puzzled by the clinical complexities of treatment. And finally, I am under no illusions. I realized that this patient may only attend sporadically, as constantly seeking new caregivers out of frustration is habitual in those dealing with psychosomatic issues. I will remain consoled by knowing that I provided care as best I as I could.
Compassion was also demonstrated by two colleagues, whose participation in this case I wish to acknowledge.
First is Dr. Howard Tenenbaum for his ample and gracious guidance on matters relating to neurological disorders, periodontal disease management, as well as matters relating to psychosomatic disorders.
Second is Dr. Glassman who did call me ASAP as I had requested. It has become increasingly rare for anyone to pick up a phone and actually speak into it. Seemingly there is unlimited time to text half sentences with emojis, yet no time for verbal communication so that a complex issue might be discussed quickly and thoroughly. I assume that he realized the difficulties I was about to encounter and called to lend a colleague a much needed helping hand. For Dr. Glassman’s demonstration of compassion, I have written this case report at his suggestion.
All three of us hope that these case reports represent a valuable learning tool. 
Oral Health welcomes this original article.
References
- Banting DW et al. 2000. The effectiveness of 10% chlorhexidine varnish treatment on dental caries incidence in adults with dry mouth. Gerodontology, 17, #2, 67-76.
- Symington JM et al. 2014. Efficacy of a 10% chlorhexidine coating to prevent caries in at-risk community dwelling adults. Acta Odont Scand., 72 #7497-501.
- Nguyen QV. 2021. Use of high-concentration chlorhexidine (Prevora) for reduction in need for surgery in patients with chronic periodontitis. University of Toronto Master’s Thesis.
- DiNardo J, Tenenbaum H, Perry R. 2018. Preventing poor oral health in older clients with multiple chronic conditions: the experience of the Gleam S,ile Centre. CDHA Oh Canada, summer, 21-25.
- https://www.psychiatry.org/patients-families/somatic-symptom-disorder/what-is-somatic-symptom-disorder
About the Author

Paul Belzycki graduated from UofT faculty of Dentistry in 1979. He enthusiastically provides dental-care as a solo practicing GP in Toronto. In many regards, he considers dentistry a hobby. As such, he has authored several video presentations for CDA Oasis focused on clinical dentistry as well as case-report articles. Out-of-the-office hobbies are skeet & trap shooting and running after 5 adorable grandchildren and two wonderful daughters.