
Abstract
“Immediacy” as a treatment concept has evolved over time. With the introduction of nano-modified implant surfaces, osseointegration has become faster and more predictable. This technology has allowed for the development of protocols that make immediate implant placement and provisionalization a desirable clinical reality. One of the remaining procedural obstacles for many practitioners is the fast and simple fabrication of a surgical guide and provisional restoration. New digital technology has resulted in the development of the “Genesis Guide” which incorporates both a surgical drilling guide and a temporary prosthesis in the same digitally printed appliance.
Historically, immediate implant placement pre-dates delayed placement protocols.1 Social pressures for replacement of failing teeth were reflected in patients’ desires to have an “immediate solution.”2 Early technological limitations on providing fixed crown and bridge as well as reliable tooth specific therapies, such as endodontics, led to efforts focused on developing implants with crowns that could be placed immediately in a fresh extraction socket. Modern implantology began to move away from immediacy with early implant protocols focused on implant supporting dentures.3 Individual tooth replacement protocols were hindered by implant materials and designs that did not integrate quickly or predictably in alveolar bone.4 By adopting a delayed placement paradigm with restoration after demonstrated integration of the implant, predictability and survival improved. This delayed approach also allowed for the development and implementation of both hard and soft tissue grafting techniques, which became increasingly important as edentulous sites remained unrestored.
With a better understanding of the factors that influence osseointegration and the consequent evolution of implant design, immediate implant solutions became predictable and successful. Studies have demonstrated that neither time of implant placement nor time of loading adversely affect survival when comparing immediate placement and loading with that of delayed protocols as long as certain procedural requirements were respected.5 The most important requirement is that of primary stability. It has been shown in multiple studies that at least 35 NCm of insertion torque is necessary for immediacy to be successful.6 The rational for specifying this insertion torque value is based on survival studies, some of which suggest increased integration failure rates below this number although other studies failed to support this.7 However, it must be recognized that insertion torque is a proxy for primary stability, which is a way of describing the micromotion of the implant. Orthopedic modeling has defined the amount of stress and strain that bones can tolerate before bending progresses to fracture.8 Studies starting in the 1990s sought to apply this concept to dental implants. Different experimental models examined the amount of micromotion, in the form of off-axis bending, that an implant could tolerate before failing.9 The limit was published as 140 microns; beyond this, dental implants risk failure of integration. As a functional concept in immediacy, micromotion is a valid metric and must be taken into consideration, not only as it applies to primary stability but also from a prosthetic perspective.
To provisionalize an immediately placed implant, a temporary crown that is predictably placed and easily removed must be fabricated. This necessitates screw retention as opposed to cementation. Screw retention of a prosthesis requires orientation of the implant so that the screw channel does not emerge through the incisal, facial, or interproximal areas of a crown. A second and equally important consideration is the fabrication of a temporary crown whose design will allow for incorporation in the functional occlusion in such a way to minimize loading that could exceed allowable micromotion.
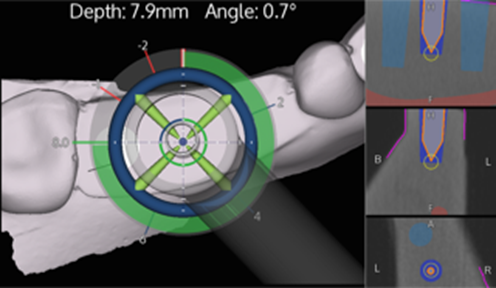
One method of ensuring that an implant is appropriately placed is through the use of guidance. Guidance is often categorized as either dynamic or static. Dynamic guidance requires the use of sophisticated surgical systems such as Nobel Biocare’s X-Guide (Fig. 1), which integrates digital imaging, planning software, and active surgical navigation through real-time high resolution displays. Static systems, by contrast, use pre-fabricated surgical guides that help guide the placement and direction of the osteotomy drills, which predetermine implant orientation. Static guides can be designed either digitally or in an analog manner using casts. The functional design of the guide can be classed as non-limited (or non-restricted), partially limited, or fully limited, which refers to the amount of restriction on drilling. In the case of fully restricted guides, each drill is indexed through a “key” which limits its angulation as well as depth.10, 11 This can be very advantageous particularly when working around sensitive anatomical structures. The inherent weakness in this approach is that if the guide is not anchored well or moves during drilling, the result is compromised. It may also limit a surgeon’s ability to make adjustments in direction and depth if unforeseen conditions are met such as unexpected bone density.12
Fig. 1A

Fig. 1B
Partially restricted guides, on the other hand, generally guide the placement and angulation of the pilot drill but not the remaining drill sequence and do not limit drilling depth. The design of surgical guides is also based to some degree on whether they will be used to guide full arch surgery or single teeth and whether an area is dentate or edentulous. In cases where there are no stable teeth available to support a guide, pin retention in bone is favored.13
Although surgical guides can be very useful in helping the implant surgeon prepare the osteotomy site for an implant based on a pre-planned approach, it does not ensure that a temporary prosthesis when fabricated can be appropriately aligned with the implant. Traditionally, in the case of a single crown for example, the temporary prosthesis is pre-made either from an analog impression, digitally printed or fabricated chair-side using a suitable denture tooth. Once the implant is placed and a temporary cylinder is mounted to the implant platform, the crown is then luted to the cylinder (picked-up) and finished to create an esthetically and functionally satisfactory temporary restoration. Although this is a generally effective approach, it is not very efficient, particularly if the angulation of the implant and the ideal screw channel position in the temporary prosthesis do not match.
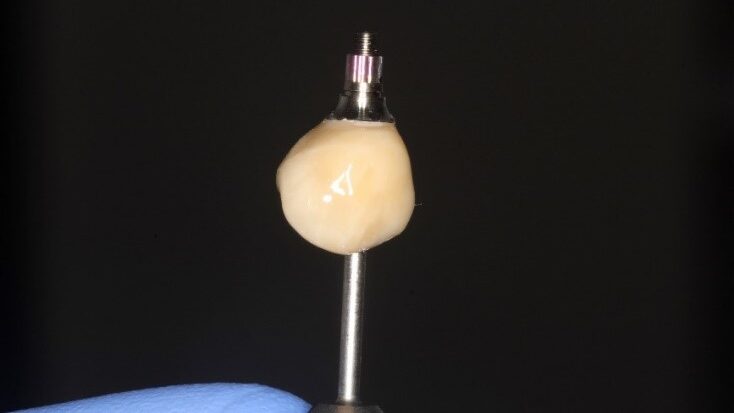
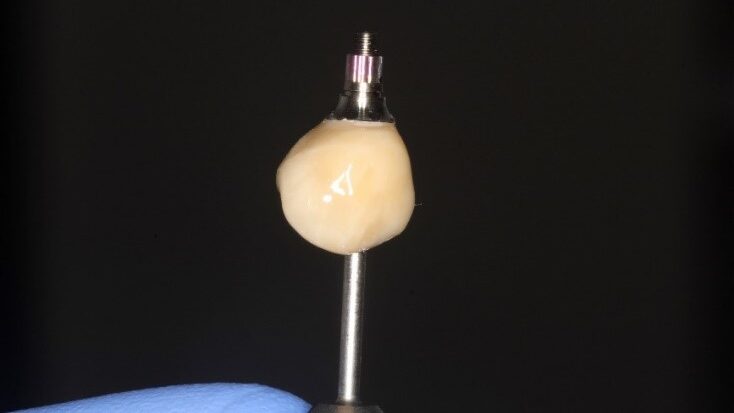
A new and innovative approach is the “Genesis Guide.” This surgical guide was developed to enhance concordance between the implant position and temporary prosthesis by making the removable prosthetic crown part of the guide. It is designed using digital planning software, which allows the integration of ideal implant placement based on CBCT and temporary prosthesis design aided by intra-oral scanning. (Fig. 2) The guide is tooth-borne to provide stability and has a pilot hole in the temporary crown which correlates to the ideal position of the screw channel and, therefore, implant placement. (Fig. 3) After the pilot hole is drilled with guidance, the remaining drilling sequence is free-hand. Once the implant is placed and the temporary cylinder is attached, the pilot hole in the temporary crown must be enlarged to accommodate the diameter of the cylinder. With the temporary crown still attached to the guide, it is luted to the cylinder with a flowable composite resin. The temporary cylinder is then unscrewed from the implant and removed with the guide. (Fig. 4) The crown-cylinder interface is then reinforced, allowing the sprues attaching the crown to the guide to be cut. The temporary crown can then be contoured, stained, and polished as desired. The crown/cylinder complex can then be screw retained to the implant platform and the occlusion adjusted to prevent overloading. (Fig. 5)
Fig. 2A
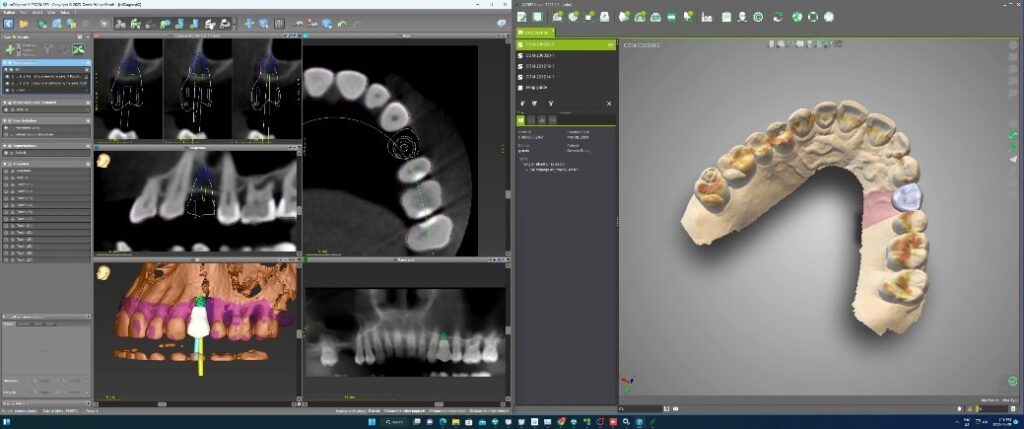
Fig. 2B
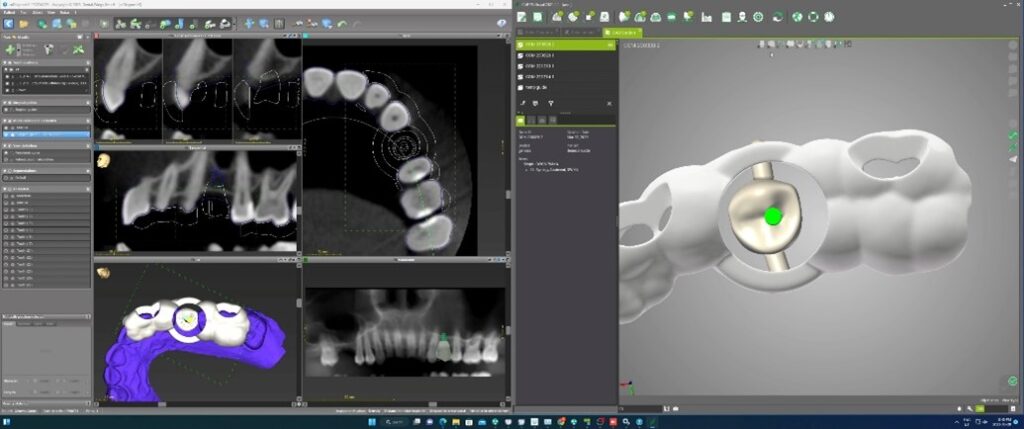
Fig. 3A

Fig. 3B
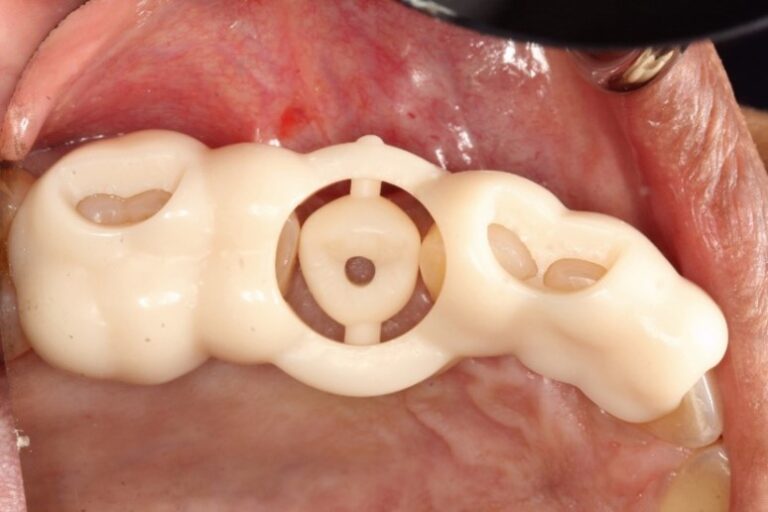
Fig. 4A

Fig. 4B
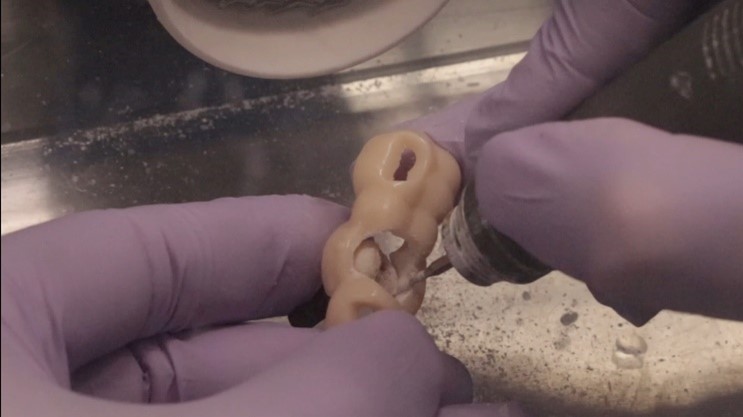
Fig. 4C

Fig. 4D

Fig. 5A
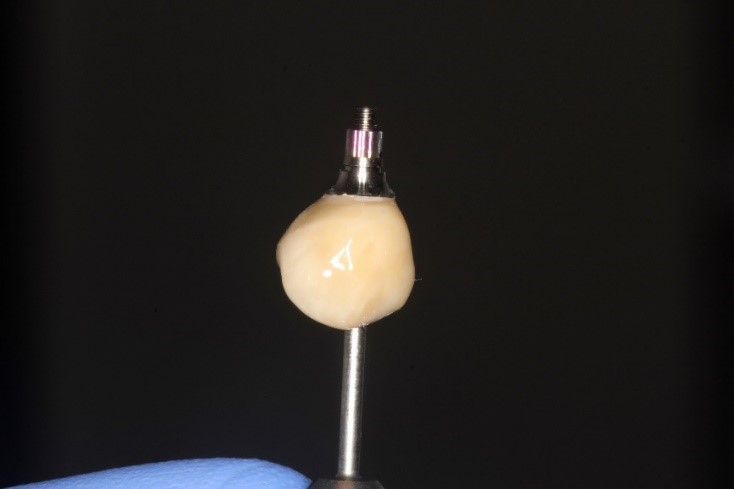
Fig. 5B

The advantages to this type of surgical splint is that it combines ideal implant placement with a custom pre-fabricated, although unfinished, temporary restoration. However, the Genesis Guide does have limitations. Most of these are self-evident during the planning stage. If there is insufficient bone to place an implant which will allow the axis of the implant to align with the proposed ideal screw channel position, then a tilted implant with a stock angled abutment may need to be used to reconcile the difference. Like most tooth-borne surgical guides that are fabricated for use in the posterior region, limited opening may complicate the instrumentation of the osteotomy. This is a potential problem for all types of tooth-borne surgical guides.
The Genesis Guide is a partially restricted surgical guide, meaning that it is intended only provide effective guidance for the position and angulation of the pilot drill. Thereafter, the osteotomy becomes free-hand. For implant surgeons who desire a guide that provides accurate guidance in terms of depth and angulation for all drills in the sequence, the Genesis Guide will not suffice. Similar to other partially restricted surgical guides, it can be successfully used in both arches and in both the anterior or posterior areas. Given its partially restricted design, it does not require absolute stability unlike fully restricted guides. For cases where the anatomy of the implantation site is tolerant of minor deviations from the planned axis of insertion and the surgeon is comfortable continuing with a freehand osteotomy preparation once the pilot hole has been established, the Genesis Guide can save a considerable amount of time in provisionalization. Another significant advantage of the Genesis guide is the ability to better manage soft tissue contours in immediate extraction and implantation cases, particularly in the esthetic zone. By defining the initial shape and contours of the temporary prosthesis during the planning stage and in conjunction with the planned implant placement, soft tissue support can be more predictably achieved. This is accomplished through the development of a desirable emergence profile which is contingent on the dimensions of the prosthetic crown and the depth of placement of the implant. By coordinating these parameters virtually, then printing the crown as part of the surgical guide, favorable esthetics are more predictably achieved.
Conclusion
There are a number of different types of surgical guides available to the implant surgeon. The innovative approach of the Genesis Guide, specifically combining the temporary prosthesis with the printed guide, allows for the placement and angulation of the pilot osteotomy using a pre-drilled screw channel in the prosthetic temporary crown. By using the pre-planned screw channel in the prosthetic crown as the “guide-hole,” accurate implant placement can be achieved. The temporary prosthesis can then be separated and when attached to the implant, which provides a well aligned immediate prosthetic implant solution. 
Oral Health welcomes this original article.
References
- Pasqualini U, Pasqualini ME. Treatise of Implant Dentistry: The Italian Tribute to Modern Implantology. Carimate (IT): Ariesdue; 2009 Oct. Chapter I, THE HISTORY OF IMPLANTOLOGY. Available from: https://www.ncbi.nlm.nih.gov/books/NBK409631/
- Abraham CM. A brief historical perspective on dental implants, their surface coatings and treatments. Open Dent J. 2014 May 16;8:50-5. doi: 10.2174/1874210601408010050. PMID: 24894638; PMCID: PMC4040928
- Brånemark PI. Osseointegration and its experimental background. J Prosthet Dent. 1983 Sep;50(3):399-410. doi: 10.1016/s0022-3913(83)80101-2. PMID: 6352924.
- Abraham CM. A brief historical perspective on dental implants, their surface coatings and treatments. Open Dent J. 2014 May 16;8:50-5. doi: 10.2174/1874210601408010050. PMID: 24894638; PMCID: PMC4040928.
- Ortega-Martínez J, Pérez-Pascual T, Mareque-Bueno S, Hernández-Alfaro F, Ferrés-Padró E. Immediate implants following tooth extraction. A systematic review. Med Oral Patol Oral Cir Bucal. 2012 Mar 1;17(2):e251-61. doi: 10.4317/medoral.17469. PMID: 22143704; PMCID: PMC3448306.
- Esposito M, Grusovin MG, Maghaireh H, Worthington HV. Interventions for replacing missing teeth: different times for loading dental implants. Cochrane database of systematic reviews. 2013(3).
- Darriba I, Seidel A, Moreno F, Botelho J, Machado V, Mendes JJ, Leira Y, Blanco J. Influence of low insertion torque values on survival rate of immediately loaded dental implants: A systematic review and meta‐analysis. Journal of Clinical Periodontology. 2023 Feb;50(2):158-69.
- Martin AD, McCulloch RG. Bone dynamics: stress, strain and fracture. Journal of Sports Sciences. 1987 Jun 1;5(2):155-63
- Kohli, N., Stoddart, J.C. & van Arkel, R.J. The limit of tolerable micromotion for implant osseointegration: a systematic review. Sci Rep 11, 10797 (2021). https://doi.org/10.1038/s41598-021-90142-5
- Nulty, A. A literature review on prosthetically designed guided implant placement and the factors influencing dental implant success. Br Dent J 236, 169–180 (2024). https://doi.org/10.1038/s41415-024-7050-3.
- Dioguardi M, Spirito F, Quarta C, Sovereto D, Basile E, Ballini A, Caloro GA, Troiano G, Lo Muzio L, Mastrangelo F. Guided Dental Implant Surgery: Systematic Review. J Clin Med. 2023 Feb 13;12(4):1490. doi: 10.3390/jcm12041490. PMID: 36836025; PMCID: PMC9967359.
- D’Souza KM, Aras MA. Types of implant surgical guides in dentistry: a review. J Oral Implantol. 2012 Oct;38(5):643-52. doi: 10.1563/AAID-JOI-D-11-00018. Epub 2011 Sep 9. PMID: 21905915.
- Ramasamy M, Giri, Raja R, Subramonian, Karthik, Narendrakumar R. Implant surgical guides: From the past to the present. J Pharm Bioallied Sci. 2013 Jun;5(Suppl 1):S98-S102. doi: 10.4103/0975-7406.113306. PMID: 23946587; PMCID: PMC3722716.
About the Authors

Dr. Brian Freund practices as an Oral and Maxillofacial Surgeon at the Chrysalis Dental Centre in Toronto with special interests in immediately loaded implant rehabilitation.

Dr. Steven Bongard is the founder and clinical head of Chrysalis Dental Centre in Toronto, a dental implant only facility focused on “same day” dental implant solutions.

Dr. Alex Bongard has extensive surgical and restorative experience in both full arch and single tooth implant dentistry practicing at Chrysalis Dental Centre.

Dr. John P. Zarb earned his DDS at the University of Detroit Mercy in 1995, followed by graduate prosthodontic training at the University of Toronto, earning his MSc in 2002. Dr. Zarb is a staff prosthodontist at Mt Sinai Hospital in Toronto, and a Clinical Assistant Professor at the University of Rochester, Eastman Institute for Oral Health.

Mr. Dino Vlahavas has over 15 years of expertise in Implantology and digital dentistry workflows.