


Silver diamine fluoride (SDF) has been used in caries prevention since the 1800s and has gained relevance in private practice since its FDA approval in the United States in 2015.1 While it is FDA approved for dentinal hypersensitivity, clinicians have been using SDF off-label for caries prevention and treatment, as it has been shown to stabilize early caries and to halt the process of progression of caries. Moreover, it has been shown to provide profound antimicrobial and remineralization properties on surfaces where it has been placed.2 An adverse effect of SDF is the staining of carious tooth structure, which clinically will appear to be stained a dark brown to black color.3 Healthy tooth structure does not stain. The discolored tooth structure aids the clinician in diagnosing active caries and visualization for evaluation of stabilization. While it has been revered for these characteristics, cosmetic dentists proceed with trepidation on esthetically demanding patients or on anterior teeth, as staining carious tooth structure in highly visible areas may result in an unaesthetic outcome or displeased patients.3 It seems to have received widespread acceptance in pediatric dentistry4 and geriatric dentistry;5 two aspects of dentistry where function and tooth preservation tend to supersede aesthetics. However, SDF can successfully be implemented in cosmetic and restorative private practices. The purpose of this article is to describe the use of SDF in a restorative private practice. The use of SDF will be described using case examples from a preventive-forward restorative private dental practice.
Case 1 – The incipient lesion: Prevention of caries progression on a patient for life
Patient 1 presented for a routine dental hygiene visit where multiple incipient caries lesions were detected upon evaluation of bitewing radiographs (Fig. 1). Caries management recommendations included diet and at-home hygiene modifications. Topical products were dispensed to the patient for at-home use. In-office applications of SDF and fluoride varnish were additionally suggested. Each lesion that was detected radiographically was treated with SDF (Advantage Arrest, Elevate Oral Care in USA/Oral Science in Canada) for one minute. Interproximal lesions may be particularly challenging to access. Assessing the available interproximal space will help the clinician determine the method for application.
Fig. 1
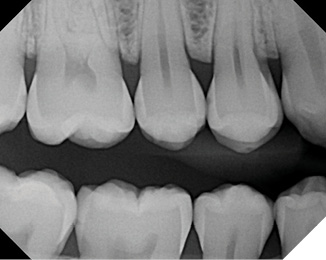
To ensure proper application of SDF to an interproximal caries lesion, the use of a small microbrush that can fit interproximally may be used. Moreover, soaking a section of Superfloss (Oral-B) and threading it interproximally is another strategy for interproximal placement. Fluoride varnish was additionally applied to increase the contact time of SDF with the early caries lesions and for caries risk minimization on the other tooth surfaces. A shorter recall frequency was recommended for careful monitoring, reinforcement of caries management protocols and applications of SDF and fluoride varnish.
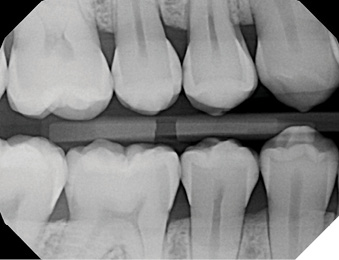
Life happens. This patient moved and sought dental care closer to her new home. Her new dentist recommended 8-10 class II composite restorations. The patient returned to my practice for a second opinion, with the hopes of managing these lesions with SDF, fluoride varnish, and risk management protocols. The patient has made the trip for this approach to her care ever since. Figure 2 depicts the patient’s most recent radiograph from 2023 (Fig. 2).
Fig. 2
Case 2 – Caries stabilization on pit and fissure caries on a fearful young patient
Have you ever had to break the news to a child and his parent that you have detected a carious lesion, and the news provokes a look of pure terror, coupled with a teary outburst? Clinical caries was detected on the occlusal surface on this patient’s maxillary primary molar (Fig. 3). To gain trust and to reduce anxiety on this fearful child, caries stabilization was suggested. SDF has been shown to increase mineral density and tooth surface hardness, reduce the depth of a caries lesion, and inhibit proteins that degrade collagen within dentin. Moreover, silver ions have been shown to lyse membranes, denature proteins, and inhibit DNA replication in cariogenic bacteria.6 Caries can be stabilized with success on pit fissure and smooth surface caries lesions, but this protocol differs from that of Patient 1, as these caries lesions have greater visibility. This protocol includes the following:
- Isolate the tooth.
- Clean and remove debris from the tooth surface. This can be accomplished with air polishing or with pumice in a rubber prophylaxis cup.
- Apply SDF for one minute. SDF can be transferred to the tooth and additionally applied with a small brush.
- Excess SDF can be suctioned or removed with a cotton pellet.
- Increase contact time with SDF and the affected tooth by applying a fluoride varnish or Vaseline.
Fig. 3

This protocol is repeated weekly for 3 weeks or, for convenience, 3 times over the course of one month. If the caries is active, the carious tooth structure will appear dark brown-black (Fig. 4). Follow up includes clinical and radiographic evaluation and possibly the utilization of caries-detection technology. Careful, gentle palpation with an explorer can be useful, but it is vital to avoid poking the pits and fissures with excessive pressure, as this can damage7 the tooth structure that is under repair.
Fig. 4

Post-care recommendations include maintaining a more frequent dental hygiene recall schedule, with applications of SDF and fluoride varnish at every visit, coupled with meticulous at-home oral hygiene habits with prescribed tools and products.
This protocol can be employed for patients that present with dentinal hypersensitivity, root exposure in high-risk patients, or any areas where early caries are detected.
Case 3 – Caries stabilization/ prevention around crown margins
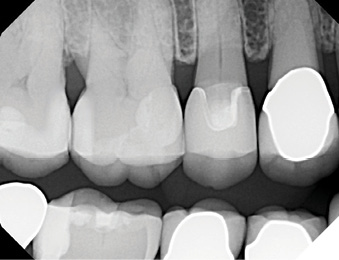
Patient 3 presented to my practice with a full-mouth reconstruction with tooth-supported crowns that were completed in another practice. She was referred to our office because caries was detected underneath one of her crowns by her periodontist. Her chief complaint of a crown replacement was completed, and the patient decided to pursue all preventive services in my practice. During a comprehensive evaluation of her dental conditions, caries was detected around multiple full-coverage restorations (Fig. 5). The patient was informed and requested to treat any necessary teeth one at a time. As a precaution, all crown margins were treated with SDF and fluoride varnish. This approach is intended to stabilize the caries process until each tooth can be treated, and to prevent new caries from developing. To date, the most reliable predictor for future caries disease is the presence of caries or a past history.
Fig. 5

Case 4 – Hindsight is 20/20, but hopefully we can prevent caries recurrence and learn from past errors
This patient presented with areas of root exposure. A caries risk assessment identified the following factors that increased the risk for the development and progression of caries: xerostomia-inducing medications, smoking, greater than 10 restored surfaces, and inadequate biofilm removal.
Biofilm can be identified via the use of a disclosing agent (TriPlaque ID, GC America) so the clinician can identify the characteristics of each patient’s biofilm (Fig. 6) and educate, and ultimately motivate the patient to perform an improved at-home hygiene regimen.
Fig. 6

Caries management and a more frequent hygiene schedule were recommended at all recall appointments, but the patient was not initially receptive, due to a lack of perceived value. When numerous interproximal caries lesions were discovered on bitewing radiographs (Fig. 7), the patient became more accepting of these recommendations, since multiple teeth required restorations (Fig. 8).
Fig. 7
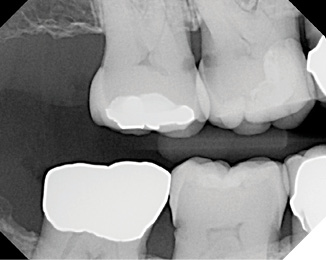
Fig. 8
When patients present with multiple risk factors, but no obvious caries lesions, it is vital to educate and motivate patients to prioritize health.
From a restorative perspective, there are many options to minimize the risk of recurrence of disease. The use of glass hybrid restorative materials can be utilized in conjunction with SDF to create a caries-resistant interface between the tooth and the restoration. Glass hybrid restorative materials can be used under a composite restoration via the open or closed-sandwich techniques. Moreover, glass hybrid restoratives can be used as definitive restorations. Advantages of utilizing glass hybrid restoratives (with or without the additional benefit of SDF) include the ability to be less invasive with preparations (including incomplete caries removal), minimal to no post-op sensitivity and caries resistance.8
Summary
It is the best practice to provide caries and periodontal risk assessments on patients at every recall appointment. New risk factors can be identified and risk category classifications can change. There are many strategies to minimize the risk of caries, including the application of SDF, and should be considered on all patients on an individualized basis. There are many indications for the use of SDF in clinical practice and it can be successfully and efficiently employed in any clinical practice, including those that prioritize cosmetic, esthetic, and reconstructive dentistry. After all, don’t you want your restorations to last a lifetime? 
Oral Health welcomes this original article.
References
- Peng, JJ-Y., Botelho, MG., Matinlinna, JP. Silver compounds used in dentistry for caries management: A review. J Dent. 2012; 40(7): 531-41.
- Zhao, IS., et al. Mechanisms of silver diamine fluoride on arresting caries: a literature review. Int Dent J. 2018 Apr; 68(2): 67-76.
- Asghar, M., et al. Approaches to minimize tooth staining associated with silver diamine fluoride: a systematic review. J Esthet Rest Dent. 2023 Jan; 35(2): 322-32.
- Carlı, C., & Seymen, F. (2023). Silver Diamine Fluoride in Pediatric Dentistry. European Journal of Research in Dentistry, 7(1), 47-53.
- Hendre, AD., et al. A systematic review silver diamine fluoride: Effectiveness and application in older adults. Gerodontol. 2017 Dec; 34(4): 411-9.
- Horst JA, Ellenikiotis H, Milgrom PL. UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride: Rationale, Indications and Consent. J Calif Dent Assoc. 2016 Jan;44(1):16-28. PMID: 26897901; PMCID: PMC4778976.
- Hamilton, James C. et al. Should a dental explorer be used to probe suspected carious lesions? JADA. 136(11); 1526 – 1532
- de Lima Navarro, MF., et al. Consensus on glass-ionomer cement thresholds for restorative indications. J Dent. 2021; 107. 10369. Epub 2021 Feb 18.
About the Author

Dr. Maragliano-Muniz was a dental hygienist before earning her DMD from Tufts and her certificate in Advanced Prosthodontics from UCLA. She is a prosthodontist, Chief Editor for Dental Economics, co-host of the podcast Dentistry Unmasked, Chief Development Officer for Cellerant Consulting Group and maintains a private practice in Salem, MA. In 2010, Dr. Maragliano-Muniz was awarded the Adult Preventive Care Practice of the Year by the American Dental Association.