


Orthodontics has always aimed to create aesthetically pleasing smiles and functional occlusions, but today, we strive for even more. Modern orthodontic care emphasizes not only straightening teeth and correcting malocclusion, but also optimizing facial balance, smile aesthetics, airway development, and long-term stability. Early orthodontic treatment, typically initiated between the ages of 7 and 10, is not about starting braces sooner, but about taking advantage of growth to guide development and lay the groundwork for more ideal outcomes later. As orthodontists, we are increasingly focused on proactive, strategic interventions that improve both the process and the final result of a patient’s orthodontic journey. For referring dentists, recognizing the signs that warrant early evaluation is key to ensuring each child receives the right care at the right time. The following clinical scenarios highlight some of the most common reasons for early orthodontic referrals and the rationale behind timely intervention.
1. Narrow maxilla with posterior crossbite
Rapid palatal expansion is most effective in younger patients, especially when the mid-palatal suture remains patent, typically before age 10. A narrow maxilla often presents clinically as a posterior crossbite (Fig. 1) and serves as a classic indication for early expansion. Posterior crossbites are frequently associated with functional mandibular shifts, which can contribute to asymmetric mandibular growth if left untreated.
Fig. 1

2. Narrow maxilla without posterior crossbite
A narrow maxilla does not always manifest with a crossbite. Instead, clinicians may observe compensatory lingual tipping of the lower posterior teeth and a steep Curve of Wilson (Figs. 2a and 2b). These findings suggest underlying transverse maxillary deficiency and may also indicate the need for early expansion to normalize occlusal relationships and arch coordination.
Fig. 2A

Fig. 2B

3. Severe crowding
When severe crowding is identified in the mixed dentition (Fig. 3), interceptive expansion may be warranted. Increasing arch circumference in younger patients is more predictable and stable and can reduce the likelihood of requiring extractions in the permanent dentition to relieve crowding. Additionally, in cases of extreme crowding, a serial extraction protocol may be necessary to guide proper eruption and alleviate space deficiency.
Fig. 3

4. Anterior crossbite of dental origin
A dental anterior crossbite occurs when a maxillary incisor erupts lingually and becomes “trapped” behind its opposing mandibular incisor during occlusion (Fig. 4). This misalignment can be highly traumatic to the mandibular incisors, potentially leading to rapid gingival recession and increased tooth mobility. To prevent any gingival complications, prompt orthodontic intervention is strongly recommended to minimize irreversible periodontal damage.
Fig. 4

5. Anterior crossbite of skeletal origin (Class III)
An anterior crossbite can also arise from a skeletal discrepancy, where the length of the maxilla is shorter than that of the mandible (Fig.5). Early orthodontic intervention, often using an orthopedic appliance such as a facemask, is typically recommended to facilitate forward growth of the maxilla. This appliance is most effective in patients under the age of 8 and can reduce the likelihood of requiring orthognathic surgery in the future.
Fig. 5

6. Protruded maxillary incisors
Protruded upper incisors (Fig.6) are particularly susceptible to trauma, often being the first teeth injured in facial accidents. Such injuries may lead to root canal therapy, restorative treatment, or even prosthetic replacement. Early orthodontic retraction of these teeth to a more protected position can reduce the risk of future trauma.
Fig. 6

7. Excessive overjet of skeletal origin (Class II)
A Class II malocclusion is often the result of a mandible that is underdeveloped relative to the maxilla (Figs. 7a and 7b). The use of early functional appliances to stimulate mandibular growth remains debated and likely not clinically significant. However, a well-documented effect of these appliances is the distalization of the maxillary dentition, which may occur more effectively when used before the eruption of the maxillary second molars. Additionally, early maxillary expansion can help eliminate transverse constraints and create space for the mandible to posture and potentially grow more forward, in line with the “shoe and foot” principle. These early interventions are generally more effective during the mixed dentition phase.
Fig. 7A

Fig. 7B

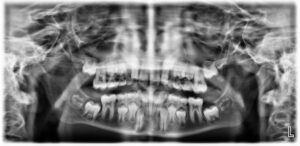
8. Poor eruption path of permanent canines
When the permanent canines develop, they are guided into position by the distal surface of the lateral incisors. Radiographic examination should reveal no overlapping between the canines and incisors; any such overlap indicates that the canines are diverging from the proper path of eruption (Figs. 8a and 8b), putting them at risk for impaction. Depending on the extent of the overlap, early intervention is often necessary to decrease the likelihood of canine impaction. Treatment may involve the extraction of the primary canines and early orthodontic treatment to create a broader path for the canines to descend into position.
Fig. 8A

Fig. 8B
9. Premature loss of primary teeth with need for space regaining
Severe crowding can frequently lead to the premature loss of primary teeth, commonly affecting the primary canines when there is insufficient space for the permanent lateral incisors to erupt (Figs. 9a and 9b). This condition leaves inadequate space for the future eruption of the permanent canines. Interceptive orthodontic treatment is often recommended to create space for the blocked-out canine, allowing it to erupt through attached gingiva and reducing the risk for subsequent gingival recession.
Fig. 9A

Fig. 9B

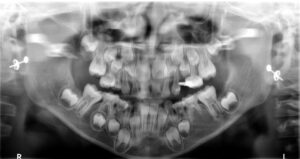
10. Delayed eruption of permanent teeth
Delayed eruption of a tooth is often attributed to obstructions such as supernumerary teeth, insufficient space, or underlying pathology (Figs. 10a and 10b). Early orthodontic intervention is frequently required to help bring an impacted tooth into position.
Fig. 10A

Fig. 10B

11. Need for space maintenance
When a primary tooth is prematurely extracted (Figs. 11a and 11b) due to extensive decay or infection, it is essential to use a space maintainer to preserve the space for the emerging permanent tooth. Without such space maintenance, the erupting tooth may lack adequate space, increasing the risk of impaction or crowding.
Fig. 11A

Fig. 11B

12. Anterior tongue thrust or digit sucking habit
Persistent oral habits, including thumb sucking and tongue thrusting (Fig.12), can contribute to bite discrepancies such as anterior open bite and excessive overjet. While many children discontinue these habits naturally, those that persist into the period of permanent tooth eruption often require orthodontic intervention. Early correction is advised, as these habits can progressively cause more harm and become more challenging to eliminate with age.
Fig. 12

13. Ectopic eruption of permanent first molars
Ectopic eruption of the permanent first molars is a developmental anomaly in which the tooth deviates from its normal path of eruption, often becoming impacted against the distal aspect of the primary second molar (Fig. 13). This can result in premature root resorption and early loss of the primary molar. If not addressed in a timely manner, ectopic molars may lead to arch length deficiency, increased crowding, a Class II molar relationship, and ectopic eruption or impaction of the second premolars. Early orthodontic intervention, typically involving distalization of the first molar, can help preserve arch integrity and reduce the risk of developing more complex malocclusions.
Fig. 13
As orthodontic care continues to evolve, our emphasis remains on achieving the most aesthetic, functional, and stable outcomes possible. Early treatment allows us to use growth to our advantage, reduce treatment complexity, and intervene before problems become more severe or irreversible. For dentists, the ability to recognize key indicators and refer at the appropriate time plays a critical role in the success of a patient’s overall orthodontic journey. By working together and referring patients at an appropriate time, we can deliver results that go beyond straight teeth, contributing to a lifetime of confident smiles, optimal function, and long-term oral health. 
Oral Health welcomes this original article.
About the author

Dr. Bruce Tasios is a board-certified orthodontist dedicated to achieving exceptional orthodontic results for patients of all ages. He earned his Doctor of Dental Surgery from the University of Toronto, followed by a General Practice Residency at Mount Sinai Hospital in Toronto. Dr. Tasios then completed his orthodontic specialty training and Master of Dental Science at Rutgers University—an experience that also allowed him to live in his favourite city, New York City. He currently practices in Toronto and is the founder of Tasios Orthodontics (tasiosortho.com) and Kids Dental Studio (kidsdentalstudio.ca).