


Abstract
The lymphatic system, though essential in fluid homeostasis, immunity, and fat absorption, has historically received minimal attention in medical and dental education. Complex Lymphatic Anomalies (CLAs) represent a rare but serious group of lymphatic disorders that carry significant morbidity and mortality. This article integrates a personal perspective with a clinical review to highlight the relevance of lymphatic disease in dental practice. Subtypes of CLAs, including Generalized Lymphatic Anomaly, Kaposiform Lymphangiomatosis, Central Conducting Lymphatic Anomaly, and Gorham-Stout Disease, are outlined with emphasis on oral and maxillofacial manifestations. Lymphatic Malformations (LMs), frequently encountered by dentists, are also described in terms of presentation, differential diagnosis, and complications. Practical dental management strategies are provided, focusing on airway risk, infection control, bleeding management, and referral guidelines. Treatment options are reviewed, ranging from surgical and sclerotherapy interventions to emerging targeted therapies, including PI3K, mTOR, and MEK inhibitors. Ultimately, the article highlights dentistry’s crucial role in the early detection and multidisciplinary management of lymphatic disease, positioning oral health professionals as key partners in enhancing patient outcomes.
Daily, the average human body circulates approximately 20-30 liters of plasma through the arterioles and into interstitial spaces. Of this volume, 90% is carried through the venules and back to the heart, comprising the blood circulatory system.1 The remaining approximately 2-3 litres is collected by a linear network of lymphatic vessels and secondary organs referred to as the lymphatic system and returned to the circulation.
As a brief review, the lymphatic system functions to:
- Assist in overall maintenance of fluid homeostasis
- Maintain immune function – by producing, transporting, and facilitating immune mediators of the adaptive immune system (lymphocytes, antigen-presenting cells)
- Absorb fats and lipophilic molecules from the upper GI tract and transport these as chyle through lymphatic vessels to eventually enter the bloodstream
Despite its critical role in basic human physiology and function, the lymphatic system has often been overlooked and regarded as secondary to blood circulation. On a personal note, during my years of post-secondary education over 20 years ago, I recall spending many hours on physiology and pharmacology courses focused on arterial and venous circulation, with very little attention given to lymph. In fact, at that time in the early 2000s, it was estimated that only about 30 minutes over a four-year medical program in the U.S. was dedicated to lymphatic education.2
Related article: The periodontal network
Unfortunately, my education in lymphatics truly began in 2019, seventeen years after graduating from dental school, when my otherwise healthy seven-year-old son was first hospitalized with suspected pneumonia. His condition quickly worsened, and he soon relied on a ventilator in the ICU to breathe. After multiple courses of IV antibiotics and bilateral chest tubes, it became clear that he was facing more than just pneumonia.
His lungs were essentially filling with a viscous, milky fluid eventually identified as chyle. After being stabilized, he went home, only to face several prolonged hospitalizations (50 days or more) due to similar pleural chylous effusions that caused episodes of life-threatening shortness of breath. Almost two years after his initial episode of chylothorax, he was finally diagnosed with a Generalized Lymphatic Anomaly, a subtype of Complex Lymphatic Anomalies (CLAs) (Fig. 1).
Fig. 1
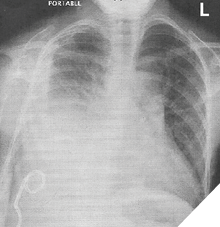
CLAs are a rare group of lymphatic disorders that involve abnormal development, structure, or function of the lymphatic system and affect multiple organs and tissues. The main subtypes of complex lymphatic anomalies are:
Generalized Lymphatic Anomally (GLA): Involves the diffuse proliferation of abnormal lymphatic vessels, and can include bone, skin, lung, and soft tissues.3 It may result in pleural and pericardial effusions, ascites, mediastinal masses, osteolysis, splenic lesions, and gastrointestinal hemorrhage.
Kaposiform Lymphangiomatosis (KLA): This is an aggressive subtype of GLA often accompanied by hemorrhagic effusions and high mortality, histologically identified by characteristic spindle cell lymphatic endothelial cell presentation.
Central Conducting Lymphatic Anomally: (CCLA) involves the malformation or obstruction of the central lymphatic channels, including the thoracic duct, causing chylous effusions and malabsorption
Gorham Stout Disease (GSD): Also known as “vanishing bone disease”, it involves progressive osteolysis resulting from lymphatic vessel overgrowth, leading to erosion of cortical bone and “vanishing” of bone on X-ray imaging.
These extremely rare disorders are often severe, associated with significant morbidity and mortality.4 In medical terminology, CLAs are classified as a form of vascular anomaly. The International Society for the Study of Vascular Anomalies (ISSVA) currently categorizes complex lymphatic anomalies as a type of slow-flow lymphatic vascular malformation.5 The available literature and classification guidelines suggest that CLAs represent an aggressive and multifocal extension of lymphatic malformation (LMs).
LMs are solitary benign lesions characterized by lymphatic vessel overgrowth. They are believed to develop due to errors in lymphangiogenesis, the process of forming new lymphatic channels. They are classified as macrocystic (formerly known as a cystic hygroma), microcystic (previously called lymphangioma), or mixed, based on radiographic and clinical features.6 They are estimated to affect approximately 1 in 4,000 to 1 in 16,000 live births and are often present at birth or develop early in childhood.7
Oral presentations of LMs
Generally benign, LMs are most relevant for dentists, as they often appear in the head and neck.
Extraoral: Soft, fluctuant, fluid-filled swellings of the neck, sometimes bluish in colour, affecting posture and appearance (Fig. 2).
Fig. 2

Intraoral: Most common on the anterior two-thirds of the tongue, but also seen on the lower lip, buccal mucosa, and floor of the mouth. They appear as clustered vesicles resembling “frog’s eggs” or “tapioca pudding,” and are soft, compressible, and non-pulsatile (Fig. 3).
Fig. 3

Functional complications: Macroglossia, interference with taste and speech, malocclusion, and risk of airway obstruction. Larger lesions may impair breathing or swallowing (Fig. 4).
Fig. 4

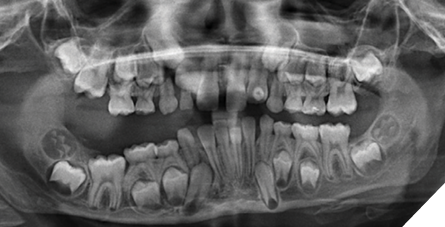
Radiographic distinction: In CLAs, osteolysis may be present. Importantly, GSD destroys cortical bone, whereas GLA does not (Fig. 5).
Fig. 5
Importantly, patients with LMs are also susceptible to secondary infections, which can cause swelling of cystic lesions and pain, especially during systemic illness.
Dental management considerations
Patients with LMs and CLAs may face unique risks during routine dental care. As these conditions can affect oral anatomy, function, and systemic health, dentists play an essential role in early detection, prevention, and appropriate referral.
1. Risk assessment and initial evaluation
History taking: Always ask about previous diagnoses of LMs, episodes of swelling, airway involvement, or systemic disease. Record how often infections or hospital stays occur.
Clinical examination: Carefully evaluate lesion size, location, and compressibility. Note any macroglossia, airway encroachment, or swelling that could complicate intubation or sedation.
Radiographic assessment: If osteolysis is suspected, panoramic or CBCT imaging can help differentiate between GSD (cortical destruction) and GLA (medullary bone involvement without cortical loss).
2. Procedural risks in dentistry
Airway compromise: Enlarged tongue or floor-of-mouth lesions can block the airway during sedation or positioning. Office-based sedation must be avoided if there is a significant risk to the airway.
Bleeding and infection: LMs are low-flow but delicate. Even minor trauma during restorative or periodontal procedures may cause ongoing bleeding or post-operative infection.
Functional limitations: Macroglossia or lip lesions may impact prosthetic fit, orthodontic appliance stability, and ability to maintain oral hygiene.
3. Modifications to dental care
Preventive focus: Emphasise prevention measures such as fluoride therapy, sealants, and meticulous oral hygiene to decrease the necessity for invasive procedures.
Conservative surgical approach: Extractions, biopsies, or periodontal surgery should be performed cautiously, ideally after consulting with hematology or ENT specialists.
Restorative care: Rubber dam placement can be challenging in patients with macroglossia. Alternative isolation methods might be necessary.
Prosthodontics/orthodontics: Appliances should be designed with consideration of soft tissue bulk; stability may be compromised by tongue or lip enlargement.
Pain and infection control: Acute LM enlargement may be caused by infection. Prompt recognition and medical referral are necessary; antibiotics can be supportive, but systemic care is often required.
4. Interprofessional collaboration
Multidisciplinary team: Dentists should collaborate with hematologists, interventional radiologists, geneticists, paediatricians, and surgeons when managing patients with known CLAs.
Medical therapies: Recognising that patients may be undergoing PI3K inhibitors, mTOR inhibitors, or MEK inhibitors is crucial. Dentists should watch for side effects such as mucositis, delayed healing, or immunosuppression. Additionally, GSD and GLA patients with bone involvement might be treated with bisphosphonates like zoledronic acid to slow osteolytic progression.
5. Referral guidelines
Dentists should promptly refer patients to a specialist or tertiary care center if:
- Lesions are rapidly enlarging or recurrently infected.
- There are signs of airway obstruction, difficulty swallowing, or changes in speech.
- Radiographic evidence of progressive osteolysis is present.
- Oral findings coexist with systemic symptoms such as pleural effusions, unexplained pain, or fatigue.
6. Clinical pearls for daily practice
- Intraoral LMs often resemble vesicular clusters (“frog’s eggs”) and can easily be mistaken for mucoceles or hemangiomas.
- A child with recurrent swelling of the lower lip or tongue should be considered for LM in the differential diagnosis.
- Macroglossia is not only a cosmetic concern but can also affect occlusion, speech, and airway patency.
- Early detection and prompt referral are the dentist’s most valuable roles in decreasing morbidity among these patients (Table 1).
Table 1: Differential diagnosis of oral lesions with vesicular or cystic appearance
| Lesion/Condition | Clinical Appearance | Typical Sites | Distinguishing Features |
| Lymphatic Malformation (LM) | Clustered vesicles, translucent, compressible | Tongue (ant. 2/3), lip, buccal mucosa, floor of mouth | Non-pulsatile, may swell with infection, systemic associations (CLAs) |
| Mucocele | Dome-shaped, bluish, solitary lesion | Lower lip (most common) | History of trauma/lip biting, often self-resolving |
| Hemangioma/Vascular Malformation | Reddish-blue, compressible, blanching on pressure | Tongue, lip, buccal mucosa | Pulsatile, diascopy positive (blanching), unlike LM |
| Vesiculobullous Disorders | Painful vesicles/ulcers | Gingiva, palate, lips, buccal mucosa | Ulcerate, recur, systemic association |
Treatment and emerging therapies
Treatment of larger symptomatic LMs depends on the site. While some clinicians regard surgical excision as the “gold standard,” it is often not feasible due to proximity to vital structures. Treatment frequently involves sclerotherapy, where a sclerosing agent such as bleomycin or OK-432 is injected into the cystic space to cause the growth to collapse. Additionally, laser therapy may be employed to treat individual lesions, although recurrence remains a possibility.
Due to the multifocal and extensive nature of CLAs, a purely surgical approach is usually not feasible unless it is necessary to manage acute symptoms. Treating patients with CLA requires a multidisciplinary approach. Hematologists, surgeons, interventional radiologists, geneticists, and immunologists are all essential for effectively managing the complexity of these cases.
Several advances in imaging techniques, increased availability of animal models, and improvements in genomic testing have enabled newer treatments for patients with CLAs, including recent use of drug-based therapeutic interventions.
Most cystic LMs (>80%) and some GLA patients have been identified with somatic mutations in the PIK3CA gene, which encodes the p110 subunit of PI3K.8 The PI3K/AKT/mTOR pathway is a key intracellular signalling pathway that regulates the cell cycle. Inhibitors of PI3K (alpelisib) and mTOR (rapamycin) have been repurposed from their original use in cancer treatment and are now being used to help treat CLA patients with some success.9 Additionally, the RAS-MAPK pathway has also been implicated, with somatic mutations found in NRAS and ARAF genes in KLA and CCLA patients. The MEK inhibitor Trametinib has recently been successfully used to remodel and improve symptoms of lymphatic disease in some of these patients.10 While promising, the long-term safety of these drugs for treating complex lymphatic anomalies is not yet well understood.
Future directions
Lymphatic disease and dysfunction have recently been linked to CNS disorders such as Alzheimer’s, autoimmune conditions like Rheumatoid Arthritis and Multiple Sclerosis, digestive issues, as well as disorders of the cardiac and renal systems.11 Lymphatic research is considered a new frontier in precision medicine. It has recently been suggested that inducing lymphangiogenesis and activating the lymphatic vasculature during inflammation may serve as a powerful therapeutic strategy.12 Such an approach could potentially benefit the dental management of periodontal disease and have other important applications in dentistry.
Conclusion
Although relatively rare, LMs and CLAscan manifest in the oral cavity, affect craniofacial structures, complicate dental management, and influence healing responses. Dentists play an important role in the early detection of these conditions, especially in children, enabling timely referrals. Ongoing research into these rare lymphatic diseases not only drives the development of new therapies but also offers insights into the complex and still underappreciated role of the lymphatic system in wound healing, inflammation, and systemic disease. My son’s personal journey continues to inspire our family and community, reminding us daily that progress in lymphatic research is not only about science, but about the lives it touches. Special thanks to the multidisciplinary efforts of Sick Kids and the generosity from Novartis and Pfizer. Without their involvement, my son would not be looking forward to enjoying Grade 8 and his upcoming hockey season. 
Oral Health welcomes this original article.
About the author

Dr. Kevin Boyce is a practicing dentist in St. Catharines, Ontario (boycedentistry.com). He and his wife, Jennifer, launched a Foundation in 2022 both to raise awareness and promote multidisciplinary collaborative care for Complex Lymphatic Anomalies patients in Canada. The foundation is currently raising funds to help establish a Pediatric Lymphatic Disease Center within the Hospital for Sick Children in Toronto, Ontario. Please visit www.willspower.org to find more information.