


The goal of endodontics is to remove a multispecies biofilm from the root canal system to treat apical periodontitis. Historically this was done with a series of hand files that were prone to procedural mishaps, inefficient, and potentially more problematic for patients.1,2 An obvious way to eliminate the potential for iatrogenic issues with hand files is to eliminate their use all together. In recent years, a variety of mechanical instrumentation systems have incorporated a mechanical glide path file utilizing either rotary or reciprocating movements. These mechanical glide path instruments potentially increase efficiency and cleanliness of the root canal system resulting in a better outcome for both clinicians and patients. However, until recently these instruments were designed to be used in combination with hand files adding more complexity to the root canal procedure.
Reciprocation with modern endodontic instruments was introduced in 2008.3 WaveOne (DentsplySirona), the first reciprocating system followed shortly thereafter in 2011, and the metallurgy was updated in 2015 to WaveOne gold. The WaveOne technique has proved to be a safe and efficient method to enlarge and disinfect the root canal system. Although a single WaveOne file is commonly utilized to create the final shape, an enhanced glide path is needed prior to final shaping. Reciproc blue (DentsplySirona) is a recently introduced reciprocating file system that acts as an orifice shaper, mechanical glide path instrument and simultaneous finishing file. A true stand-alone single-file endodontic solution with no glide path management needed in a large percentage of cases (Fig. 1). Although this is a new option for North American clinicians, this technology has been available in other parts of the world for nearly a decade ensuring the technique has been scientifically evaluated and validated with hundreds of studies.
Fig. 1A

Fig. 1B

Fig. 1C

Reciproc blue is available in three sizes (Fig. 2). The most commonly used file is the R25 and will be the focus of this paper. It has a tip diameter of 0.25 mm and a taper of 8% in the apical 3 mm of the file. The taper percentage decreases up the file to preserve root dentin in the coronal half of the canal. The R40 has a tip diameter of 0.40 mm and an apical taper of 6% while the R50 files has a tip size of 0.50 mm and a taper of 5 % in the apical 3 mm. As with the R25, the R40 and R50 also have regressive tapers to preserve coronal dentin. The reciprocation motion is identical to that of WaveOne gold. The file rotates 150 degrees counterclockwise to cut dentin and then reciprocates back 30 degrees clockwise. This results in a net rotary motion that serves to remove debris from the root canal system. The longer cutting motion and the shorter reverse motion mean that the instrument is centred better in the canal and the reverse motion releases the stress on the instrument reducing the likelihood for a file fracture.4,5,6
Fig. 2

Although the degrees of reciprocation are identical to that of WaveOne, the rate of reciprocation with Reciproc blue is different. As a result, it is important to match the file system with the correct motor setting on the X-smart Pro+ motor (DentsplySirona) to maximize safety and efficiency of the files. WaveOne gold reciprocates with 350 cycles per minute while Reciproc blue reciprocates at a rate of 300 cycles per minute. In spite of this subtly slower rate of movement, Reciproc blue is an efficient instrument because the S-shaped cross section of results in efficient cutting of dentin and prevents taper lock of the instrument, while allowing room along the file to bring debris coronally.7
Recommendations for use when canal is visible radiographically:
If the canals are visible on a preoperative radiograph, there is a high probability that no specific orifice opening or glide path management will be needed prior to using the R25. It is not wrong to complete orifice opening and glide path enhancement, but these steps are likely unnecessary and increase the amount of work needed to complete instrumentation while providing no benefit.
- Following access, the chamber is flooded with sodium hypochlorite (NaOCl) to begin the disinfection process and provide solution to dissolve the dentin debris that is removed from the canal wall. The R25 is introduced into a canal and several short amplitude (1-3mm) pecking motions are made to allow the file to advance with light apical pressure. As the file moves apically a simultaneous lateral brushing motion of the R25 against the canal wall while moving coronally will serve to remove the dentin triangle and center the canal over the root.
- At this point, debris will have accumulated in the NaOCl and on the file. To prevent the risk of pushing debris apically and to maximize cutting efficiency of the R25 rinse with a 30-guage side vented ProRinse (DentsplySirona) irrigating needle and remove debris from the file with an alcohol-soaked gauze or sponge. It is very important to irrigate regularly with copious amounts of NaOCl.
- Continue with the “peck down, brushing out” steps to enhance the glide path while simultaneously instrumenting the final shape of the root canal system. Light apical pressure is used and the amplitude is again in the 1–3 mm range, but no more than 4 mm. The shape and length of the root will determine how many cycles will be needed. As debris accumulates and the file loses cutting efficiency continue to rinse with NaOCl and clean the file with the gauze.
- As estimated working length is approached the X-smart Pro+ motor doubles as an electronic apex locator and working length canal be determined dynamically with the R25 while reciprocating. This will require a precise amount of NaOCl in the canal, but caution is needed to prevent interference from metal restorative materials in the chamber. If the dynamic reading is inconsistent then it is recommended to use a 10-K file with the X-smart Pro+ to measure and confirm the exact length of the canal.
- Following determination of working length, the R25 is used at the working length with a lateral brushing out motion away from the furcation to create the final shape, but care should be taken to not linger at the apex to prevent any potential for over-enlargement.
- A final irrigation protocol is used to maximize the disinfection and remove smear layer.
- Reciproc size matched paper points and gutta percha are used to dry and obturate the root canal system.
Recommendations for use when canal is not visible radiographically or the R25 stops advancing in the canal:
- After the canals are located the steps for instrumentation are very similar if the canal is radiographically visible or not. In the great majority of cases if a 10-K file will enter the canal so will the R25. If the canal is severely constricted then orifice opening is always an option, but as stated previously this is most likely unnecessary.
- Gauging the canal with a 10-K file and alternating the R25 with the 10-K file is a safe and predictable way to measure how far into the canal the R25 will advance. There is no significant hand filing with this technique. A 10-K file is tapped into the canal until it no longer advances and the R25 is taken 1 mm less than the depth of the 10-K file to prevent any potential to bind the R25 or create a ledge. This will open the canal coronally and allow the 10-K file to incrementally advance to the apex, as the apex is considerably larger than 0.10 mm. This method of alternating the 10-K file and R25 is then repeated until working length is achieved.
- If the R25 fails to advance an R-pilot (DentsplySirona) can be used to enlarge the glide path. The R-pilot is a reciprocating mechanical instrument designed to be used with the same pecking motion and 1 -3 mm amplitude strokes as with the R25. The motor settings for the R-pilot and R25 are identical. The S-shaped cross section results in a similar feel and cutting action as the R25. The R-pilot has a tip dimension of 0.125 mm and a constant taper of 4 %. The R-pilot utilizes M-wire to maximize the cutting efficiency while maintaining flexibility to negotiate small canals (Fig. 3).
Fig. 3

Conclusions
The focus of this discussion was on the R25 and management of standard and small canals. However, the R40 and R50 are excellent alternatives for larger canals in younger patients allowing the Reciproc family of files to shape most root canal anatomies encountered in a general practice setting (Fig. 4). The use of a mechanical file prior to scouting with a hand file is considered high risk by many clinicians. This is likely the result of antiquated teaching methods and a lack of understanding about modern file design and metallurgy. The heat treatment and file design of Reciproc increase flexibility and fatigue resistance while maintaining excellent cutting efficiency and torque strength. Reciproc blue provides clinicians with a simplified and predictable technique for enlarging the root canal system without the use hand files or glide path enlargement in the majority of cases. The reciproc system allows dynamic working length determination with the X-smart Pro+ motor potentially decreasing chair time. Size matched paper points and gutta percha yield a predictable way to dry and fill the canal in three dimensions prior to permanent restoration (Fig. 5).
 Fig. 4A
Fig. 4A
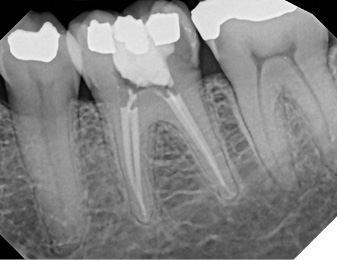
Fig. 4B

Fig. 4C
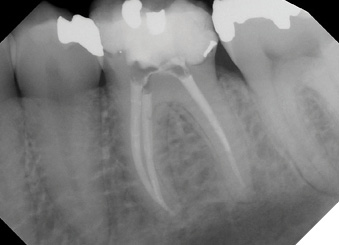
Fig. 4D

Fig. 5A

Fig. 5B

Fig. 5C

Oral Health welcomes this original article.
References
- Jafarzadeh H, Abbott PV. Ledge formation: review of a great challenge in endodontics. J Endod. 2007 Oct;33(10):1155-62.
- Pasqualini D, Mollo L, Scotti N, Cantatore G, Castellucci A, Migliaretti G, Berutti E. Postoperative Pain after Manual and Mechanical Glide Path: A Randomized Clinical Trial. J Endod 2012;38:32-6.
- Yared G. Canal preparation using only one Ni-Ti rotary instrument: preliminary observations. Int Endod J. 2008 Apr;41(4):339-44.
- Bueno CSP, Oliveira DP, Pelegrine RA, Fontana CE, Rocha DGP, Bueno CEDS. Fracture Incidence of WaveOne and Reciproc Files during Root Canal Preparation of up to 3 Posterior Teeth: A Prospective Clinical Study. J Endod. 2017 May;43(5):705-708.
- Kim HC, Kwak SW, Cheung GS, Ko DH, Chung SM, Lee W. Cyclic fatigue and torsional resistance of two new nickel-titanium instruments used in reciprocation motion: Reciproc versus WaveOne. J Endod. 2012 Apr;38(4):541-4.
- Silva EJNL, Vieira VTL, Hecksher F, Dos Santos Oliveira MRS, Dos Santos Antunes H, Moreira EJL. Cyclic fatigue using severely curved canals and torsional resistance of thermally treated reciprocating instruments. Clin Oral Investig. 2018 Sep;22(7):2633-2638.
- Bürklein S, Hinschitza K, Dammaschke T, Schäfer E. Shaping ability and cleaning effectiveness of two single-file systems in severely curved root canals of extracted teeth: Reciproc and WaveOne versus Mtwo and ProTaper. Int Endod J. 2012 May;45(5):449-61.
About the authors

Dr. David Landwehr earned his DDS at the University of Minnesota. He also received an MS degree and certificate in oral and maxillofacial pathology from Ohio State University and specialty training in endodontics from the University of Michigan. He was the Chief of Endodontics for the Meriter Hospital general practice residency for more than ten years.

Dr. Gary Glassman lectures globally on endodontics, is on staff at the University of Toronto, Faculty of Dentistry in the graduate department of endodontics. He maintains a private practice, Endodontic Specialists in Toronto, Ontario, Canada. His personal/professional website is www.drgaryglassman.com.