


Over the past few decades, patient demand and inquiries regarding dental implants have increased significantly. Today, more than 100 commercial implant brands exist, with an estimated 12–15 million implants placed annually worldwide.1 As a result, by 2023, over 200 million patients globally were living with dental implants. According to Grandview Research, North America accounted for 38.4% of the global dental implant market in 2024.2 Canada is projected to experience the highest compound annual growth rate in the region at 8.9% between 2025 and 2030, reaching an estimated $9.62 billion USD by 2030. These figures underscore the rapid growth of implant dentistry, where the cost of a single implant-supported crown can range from $3,000 to $6,000 depending on clinical factors.
Despite the booming implant industry, regulatory structures remain limited. There is no unified framework ensuring provider qualifications, product quality assurance, or patient safety. Currently in Canada, implants are most commonly placed by oral and maxillofacial surgeons, periodontists, and general dentists, while prosthodontists and general dentists typically perform restorative work depending on complexity. Specialty training is critical, yet continuing education courses—often sponsored by implant companies—promote implant procedures among general dentists, sometimes with inconsistent quality standards. The Royal College of Dental Surgeons of Ontario was the first to regulate implant-related clinical qualifications to protect patients.3 Similarly, the European Association for Osseointegration has explored establishing a Dental Implant Register, inspired by medical registries (e.g., Swedish hip fracture and cataract surgery registries), to monitor treatment outcomes and close knowledge gaps among clinicians.1
At the intersection of two powerful forces—the ‘therapeutic concept of implant dentistry supposedly benefiting the patients’ and ‘industry-driven research and development supposedly profiting the industry’—there may be some unanswered questions among clinicians and also the patients relating the new diseases called ‘peri-implant diseases’. This term was coined by the French clinician, ‘Levignac’ in French literature but officially used in the first European Workshop on Periodontology in February, 1993.4 There have been strong evidences of more interest in this entity in clinical and research areas. This paper will review the current status and management reality in this new era of peri-implant diseases.
Definition of peri-implant health
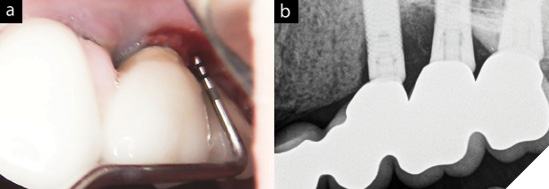
Peri-implant health is a physiological yet artistic joint operations to achieve integration of non-vital structure and host and stability among various anatomical elements such as peri-implant mucosa, connective, and bone tissues. Human studies showed the consistent dimension of the supra-crestal attachment apparatus of 3.1-3.9mm, of which 2mm is considered to be an epithelium, which is called ‘barrier epithelium’.5 Probing around the peri-implant tissue would break the seal of adhesion, but it will re-establish in 5-7 days after clinical probing, as shown in the animal studies.6 A clinician must be able to detect any deviations from the norm in this physiological architecture to define the peri-implant diseases, understanding that the probing depth can be a bit deeper by 1.0-1.5mm around peri-implant tissues compared to the gingiva around the natural teeth due to the absence of the cementum layer and orientation of collagen fibers, lacking ‘resistance of probing’. When probed with a lighter force (0.25N), healthy probing numbers should be less than 6mm and 3mm probing depths in the papilla between an implant-supported crown and a natural tooth, and between two adjacent implants, respectively, with the absence of erythema and bleeding upon probing.
Fig. 1

Diagnostic criteria of peri-implant diseases
The 2017 World Workshop established the most widely accepted definitions of peri-implant diseases, particularly through the consensus of Workgroup 4, led by Tord Berglundh.7 Prior to these, the definitions of peri-implant diseases (i.e. peri-implant mucositis and peri-implantitis) were all over the maps and were not even possible to come up with the prevalences with consistent criteria. Today, peri-implant diseases are estimated to affect 20% of patients and 10% of implants, highlighting their site-specific rather than host-specific nature.8
Peri-mucositis is confined within the soft tissue (not the marginal bone level, yet) and is assumed to precede peri-implantitis.7 Similar to gingivitis, the sites affected by peri-implant mucositis exhibit inflammation, characterized by erythema and bleeding on probing/without suppuration. Also, it may show increased probing depth not because of bone loss, but due to an edematous gingival margin and a loosened degree of the peri-implant tissue upon probing. Typical signs around the sites are plaque accumulation and the likelihood of a minimal amount or even absence of keratinized tissue.
Peri-implantitis is an inflammatory lesion initiated by plaque accumulation, triggering the inflammatory cascades involving supporting bone loss, which is active and progressive.7 Since this is pathological and biofilm-induced, the anti-infective management protocol has been found to be effective in reducing the signs of inflammation and disease progression. Clinical signs include inflammatory signs on the soft tissue, such as peri-implant mucositis (erythema, edema, B/SOP, and increase in PDs). Most importantly, there must be signs of progressive bone loss, with the understanding that the progression of bone loss may accelerate over time in a non-linear pattern.9
In the context of marginal bone loss, Albrektsson et al. suggested that a ‘steady state’ may follow the initial phase of physiologic bone remodeling, and that not all implants exhibiting marginal bone loss necessarily require treatment.10 Without this perspective, clinicians may risk overtreating implants that have already achieved a ‘foreign body equilibrium’ with the host immune system, thereby maintaining a delicate balance.
Table 1: Case Definitions proposed by the 2017 World Workshop11
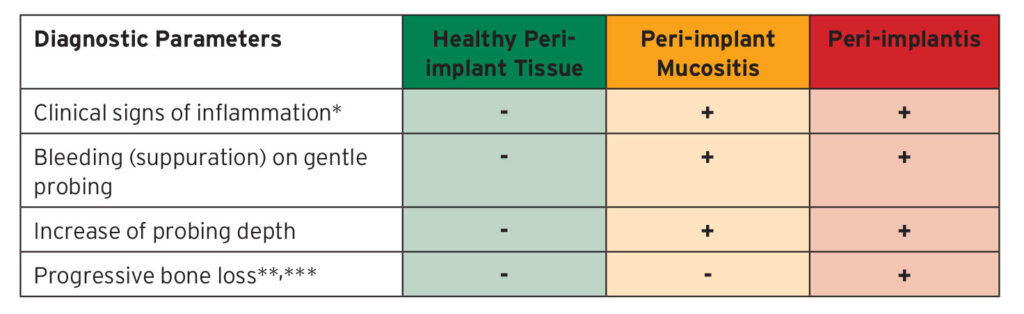
- In the absence of sufficient baseline data to determine the progression of clinical parameters, clinicians are advised to use the following diagnostic criteria: Presence of B(S)OP on gentle probing
- Probing depths of 6mm or up
- Bone levels is more apical of the most coronal portion of the intraosseous part of the implant by 3mm or more
Fig. 2
Investigation of ‘primary etiology’
A critical aspect of this discussion is identifying the underlying causes of peri-implant disease. The debate remains controversial, as the condition arises from the presence of a foreign body placed in one of the most complex environments of the human body. For long-term success, both hard and soft tissues must remain healthy around this non-vital structure without exhibiting signs of inflammation. At the same time, the peri-implant environment must withstand constant microbial challenge. The oral cavity naturally harbors diverse microbial communities, as bacteria are essential residents of its ecological system. Given its nutrient-rich, warm, and moist conditions, the human mouth provides an ideal environment for bacterial growth, which can, under dysbiotic conditions, jeopardize peri-implant health.12 The peri-implant diseases are known to be more likely, biofilm-induced, with substantial evidence.7 Understanding the etiologies and risk factors of peri-implant disease requires awareness of how biofilms form and function. These microorganisms are not inherently harmful; rather, the peri-implant environment inadvertently provides an ideal niche that enables them to organize into resilient communities (biofilms) for survival and proliferation. The diverse morphologies of these biofilms have been clearly demonstrated through scanning electron microscopic analyses of failed and explanted implants.13
Fig. 3
![Radiographic images of a set of implants removed due to severe bone loss. These implants represent different thread type (aggressive [a], regular [b, c, e, f] or mild [d]), surface characteristics (oxidized [a–c, f] or SLA [d, e]), level of placement (bone [a–c, e, f] or tissue level [d]) and abutment fit (butt joint [b–d, f] or platform-shifting [a, e]) and splinted (b and f) and nonsplinted (d and e) adjacent implants. SLA, Sand-blasted, large grit, acid-etched. (Extracted from Chang et al.(2021))13](https://media.oralhealthgroup.com/uploads/2025/10/Chang-fig_3.png)
Fig. 4
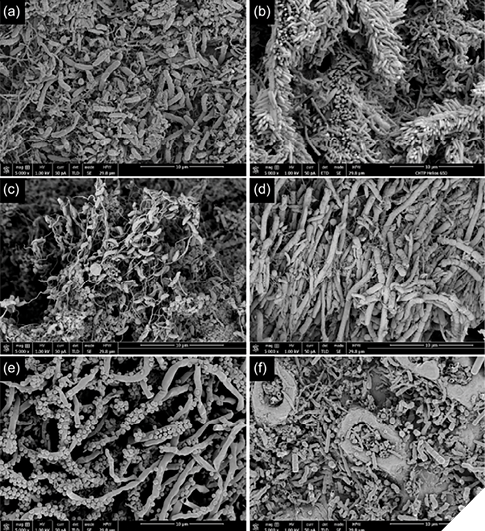
As illustrated in Figure 4, diverse bacterial morphologies were observed on the surfaces of implants that ultimately required removal (Fig. 3). These bacteria are organized into biofilms that are particularly difficult to eliminate, especially on rough implant surfaces, and are largely resistant to systemically administered antibiotics. Within peri-implant pockets, biofilms embed deeply into cracks and surface irregularities, triggering host immune responses that drive progressive bone loss as the colonies expand. Ultimately, the only definitive solution may be the removal of contaminated surfaces or the complete eradication of biofilm layers adhering to rough implant surfaces—a goal that remains clinically challenging and often nearly impossible to achieve consistently.
The presence of biofilm on exposed implant surfaces driven by progressive bone loss and dominated by keystone pathogens, represents a critical tipping point in disease progression.14 There may be the additional sources of the threats of biofilm around the implant-abutment junctions(IAJ) and the restorative margins proximal to the crestal bone due to short distance in the gingival height of abutments violating the supra-crestal attachment apparatus(i.e. biological width). These crowns often cemented on to the stock abutment in the lab without quality check of the restorative margin. A clinician must be mindful of any micro-gaps created in placement of implant and fabrication of prosthesis because of those micro-gaps will eventually be harbored by biofilm and result in the opening up the road for the biofilm infiltration and proliferation being the final nail in the coffin (Fig. 5).
Fig. 5

At this stage, host immune defenses are compromised, and once immune surveillance is impaired, rapid dysbiosis ensues. This dysbiotic state initiates a vicious cycle of marginal bone resorption at the crest, which in turn creates additional space for bacterial colonization and further exacerbates disease progression.
An important consideration is that the bacterial profile found in peri-implantitis closely resembles that of periodontal pockets, with no unique microorganisms identified as specific to peri-implant disease in either immunological or microbiological terms.7 When combined with the findings of Quirynen et al. on intra-oral translocation,15 this suggests that periodontal pathogens can compromise peri-implant tissue health over the long term. These organisms appear to act opportunistically, sharing similar microbial profiles between periodontal and peri-implant diseases, and thereby perpetuating risk across both conditions.15
Risk factors/indicators – potential to be the secondary etiologies
Risk factors are conditions or characteristics that increase the likelihood of peri-implant disease, supported by evidence from longitudinal studies, whereas risk indicators are features identified primarily through cross-sectional research without long-term validation. In implant dentistry, the scarcity of well-designed longitudinal studies limits the ability to distinguish clearly between these categories, creating inevitable overlap. Clinicians should therefore recognize that the boundary between risk factors and indicators can be blurred. Current clinical and research evidence consistently highlights biofilm formation and host dysbiosis as the primary etiologic drivers of peri-implant disease. With this in mind, clinicians must evaluate how and where implant-supported prostheses may harbor biofilm capable of triggering host immune responses. Multiple contributing factors and their interactions can lead to similar clinical manifestations, including erythema, edema, bleeding or suppuration on probing, and, in some cases, progressive marginal bone loss. Accordingly, clinicians must carefully assess patient-level characteristics, surgical sites, implant placement, prosthetic design, and maintenance protocols for potential or unforeseen risk factors and indicators. Such vigilance is essential to prevent post-therapy complications and undesirable clinical outcomes. Local factors have been included in this discussion because, given the opportunistic nature of these diseases, they may act as secondary etiologies over the long term.
a. Systemic health and medications
- Smoking (current, history of)16
- Diabetes mellitus (both Type I and II) – glycemic control17, 18, 19
- Osteoporosis/Osteopenia20, 21
- Anti-resorptive medications22,23
- Cardiovascular diseases – association of Epstein-Barr virus18
- Obesity and high systolic blood pressure24
- Reported Medications lists relating to peri-implantitis25
- Steroid
- Organ transplant medications
- Anti-neoplastic medications
- Proton-pump inhibitors
- Antacids
- Androgen-deprivation therapy
- Selective serotonin reupdate inhibitors
- Penicillin-allergy (self-reported)26
b. Patient’s factors27,28,29,30
- Poor oral hygiene
- History of periodontitis
- Parafunctional activity (bruxism, clenching)
- Lack of peri-implant maintenance therapy
c. Local factors and site-specific conditions31,32
- Inadequate bone quality – D3, D4
- Insufficient bone quantity – A minimum of 1.5-2.0mm thickness
- Traumatic occlusion
d. Surgical errors33
- Improper implant placement – angulation/position
- Poor GBR pre, intra and post-implant placement
- Timing of surgery post GBR
- Lack of robust soft tissue profile during surgical phase
e. Restorative conditions34,35,36
- Poor prosthetic design – contour, contact, violation of supra-crestal attachment apparatus (i.e. biological width)
- Premature loading
- Improper occlusal scheme resulting in occlusal overload
- Cement-induced marginal bone loss
- Inaccessible/uncleanable implant abutment junction or restorative margin i.e. micro-gaps
f. Soft tissue profile37
- Lack/minimal of keratinized gingiva around the neck of prosthesis in both dimension: vertical and horizontal
- Lack/minimal of attached tissue around the neck of prosthesis in both dimension: vertical and horizontal
- Shallow vestibule
The potential risk factors and indicators for peri-implant disease are complex and multifaceted, and the body of evidence continues to grow. Clinicians must therefore remain up to date with emerging research and evolving clinical guidance. It is equally important to interpret the current evidence cautiously, as much of it is derived from case reports, cross-sectional studies, or short-term cohorts that offer only limited strength of evidence. Despite these limitations, clinicians should remain mindful of these risks and communicate them appropriately during informed consent and treatment planning to ensure patients are fully informed.
The current management: ‘Non-surgical’ vs. ‘surgical’ interventions
There are numerous approaches to managing peri-implant diseases, and no single method can be considered universally superior. This is largely due to the inherent variability of implant therapy and the differences in how implant-supported prostheses are planned and executed. When faced with a failing or ailing implant, clinicians must adopt a systematic approach: establish an accurate diagnosis, identify the primary and secondary etiologic factors, address them appropriately, and then select from the available non-surgical or surgical treatment options as indicated.
A. Non-surgical treatment for peri-implant diseases
- Mechanical debridement – Ti curettes, Specialized cavitron tip
- Antimicrobial Photodynamic therapy(aPDT)38,39
- Antimicrobials(Local adjunct: Metronidazole Minocycline oinment,40 Hyaluronic acid41, Chlorhexidine chips,42 systemic MTZ43*
- Lasers – Er:YAG,44 Diode45
- Erythritol(or Glycine) air abrasion devices46
- Chitosan brush47
- Polymer micro-brushes48
- Pulsed Electromagnetic field therapy49
*not recommended as routine
B. Surgical treatment for peri-implant diseases50
- Access flap for infected surface disinfection
- Surface disinfection
- Mechanical
- Ti-curettes/Cavitron with a special tip
- Air-abrasion (Airflow)
- Implantoplasty
- Ti-brush
- Polymer brush
- Chitosan brush
- Chemical/local antibiotics
- Chlorhexidine gel
- Hydrogen peroxide (3%)
- Tetracycline/Doxycycline
- Citric acid
- Laser surface decontamination –
- Antimicrobial PDT
- Electrochemical – Galvosurg
- Resective approach – osteoplasty/ostectomy – for pocket reduction purposes
- Regenerative approach – Guided bone regeneration
- Biomaterials: Alloplast, Xenograft, Allograft (FDBA/DFDBA), Autograft with/without non-resorbable/resorbable membranes, Enamel-matrix derivatives
- Adjunct therapy of concentrates of growth factors (PRP, PRGF, PRF)
- Peri-implant phenotype modification(CTG, FGG)51
- Combination of the above
An important aspect of peri-implant disease management is its time-sensitive nature. Once disease is initiated, it tends to progress without spontaneous resolution. From a microbiological perspective, this is logical: pathogenic biofilms established on implant surfaces continue to expand their colonies, intensifying the infection and leading to further marginal bone loss. This vicious cycle underscores the challenge of controlling the disease. Notably, the European Federation of Periodontology (EFP) S3-level clinical practice guideline describes peri-implantitis as ‘stable peri-implantitis’ even following successful treatment, reflecting the chronic and persistent nature of the condition.52 Furthermore, retrospective studies by Chang et al. demonstrated that early diagnosis of peri-implantitis enables timely non-surgical intervention, which in turn helps preserve marginal bone levels and maintain implant survival.53
Fig. 6

Secondly, the surgical management of peri-implantitis must be tailored to the extent, severity, and morphology of the osseous defect. The evidence base for these interventions varies in strength, making definitive conclusions difficult. Systematic reviews of four randomized controlled clinical trials and one longitudinal comparative study with 2–5 years of follow-up reported some degree of positive outcomes across surgical approaches. However, the results were heterogeneous, reflecting mixed efficacy among different surgical techniques and underscoring the need for further high-quality research in this area.54
Thirdly, the potential benefits of submerged versus non-submerged healing warrant consideration in the surgical management of peri-implant diseases. In some cases, removal of the prosthesis and disconnection of the implant–abutment junction may be necessary even during non-surgical treatment of peri-implant mucositis to allow improved access for thorough debridement and disinfection. In surgical interventions for peri-implantitis, complete coverage of the surgical site with primary closure is generally more advantageous, as it promotes undisturbed regeneration of intraosseous defects around the implant fixtures. Experimental evidence from animal studies demonstrated that submerged healing achieved superior outcomes compared to non-submerged approaches.55 More recently, a prospective controlled study of 30 implants in 22 patients by Wen et al.56 reported predictable reconstruction of intraosseous peri-implant defects. In that study, surface detoxification was achieved using implantoplasty, glycine air-abrasion, and topical tetracycline (250 mg applied for 5 minutes). Defects were then grafted with a composite material (60% FDBA-cortical, 20% xenograft, 20% autograft), covered with a perforated d-PTFE membrane secured with fixation screws, and closed with a periosteal-releasing incision. Primary closure and undisturbed healing were identified as key factors contributing to the favorable regenerative outcomes.
Modification of the peri-implant soft tissue phenotype is a critical component of treatment. Whether performed prior to surgical intervention or following non-surgical therapy aimed at reducing bacterial load and inflammation, ensuring robust and healthy soft tissue is essential to improving treatment outcomes. Common clinical indicators of successful peri-implant therapy include reductions in probing depth and clinical attachment loss, absence of bleeding or suppuration on probing, radiographic evidence of bone gain within intraosseous defects, and stabilization of marginal bone levels. Dalago et al., in a three-year prospective study of 23 patients, demonstrated that simultaneous subepithelial connective tissue grafting significantly improved peri-implant health.57 Additionally, Giannobile et al. concluded that soft tissue augmentation enhances peri-implant health by increasing the width of keratinized mucosa, thereby facilitating plaque control, and by augmenting mucosal thickness, which contributes to improved esthetics around implant-supported crowns.58
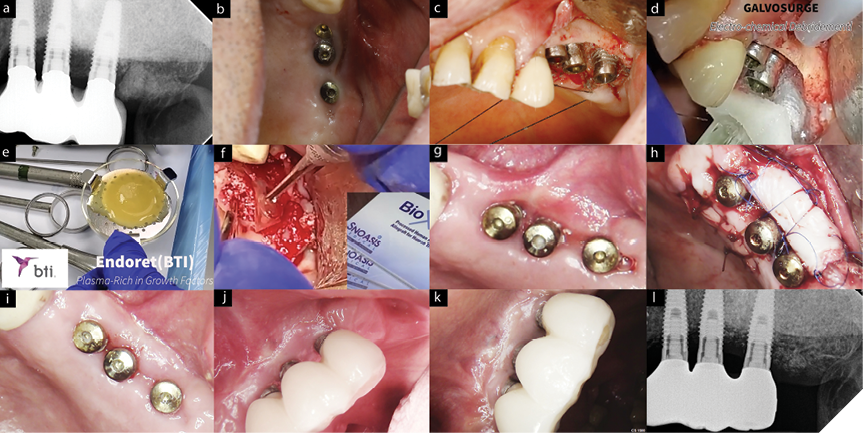
Fig. 7A-K
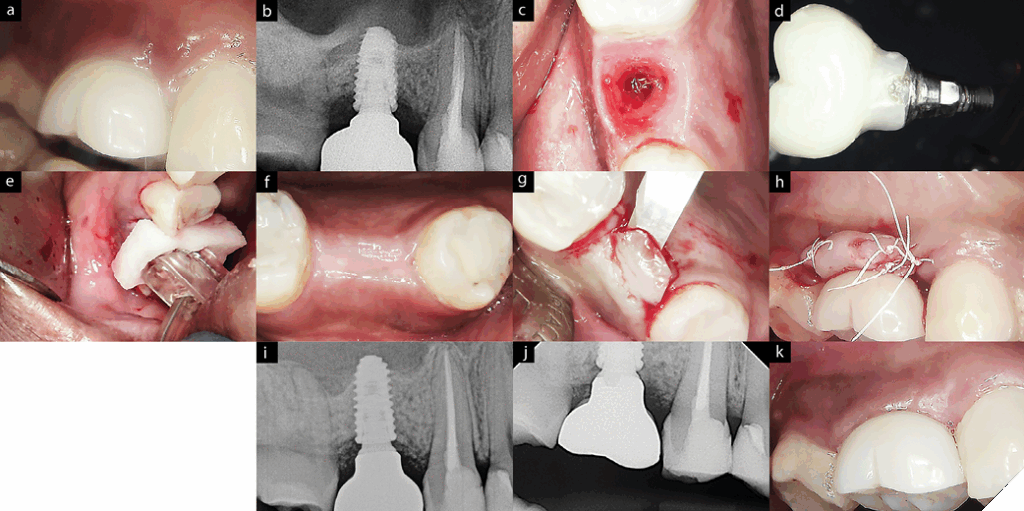
ematous internal gingiva with bleeding is evident upon removal of the crown. D. Screw-retained crown with discrepant restorative margin. E. ‘Galvosurg ‘was utilized for implant surface disinfection. F. Submerged healing protocol. G. After 4 months, second stage performed with apically positioned flap to position palatal keratinized tissue to buccal side of the crown. H. The same crown was inserted after disinfecting the crown margin (Remake of a new crown recommended but denied by the patient). I. 6-months post-op radiograph shown ‘crestal bone stability’ with bone fill materials. J. 1-year post-op clinical presentation with absence of BoP and stable peri-implant tissue. K. 1-year post-op BW showing stable marginal bone level on #16.
Fig. 7L
Fig. 8
Elephant in the room: ‘Patient-centred perspectives’
Opportunities and information in implant dentistry continue to expand rapidly for both clinicians and patients. Yet, the burden of peri-implant diseases remains the ‘elephant in the room.’ Despite the growing prevalence of these conditions, awareness among patients is strikingly low. Insua et al. reported that 74% of patients had no knowledge of peri-implant pathology, underscoring a major gap in patient education.59 Given the prevalence of peri-implant diseases and the unpredictable nature of their management, these findings should be alarming to every implant clinician. The data suggest that the dental implant community has not devoted sufficient effort to educating patients and the public about these conditions. Among those affected, 64% expressed worry or concern, and 32% described living with peri-implant disease as a terrible experience.59
Clinical Implications of the dental implant loss due to peri-implantitis
Once a clinician places an implant and fabricates a supporting prosthesis, it must be carefully maintained to avoid the ultimate endpoint of implant loss. Bone loss associated with implant failure due to peri-implantitis is typically extensive, involving severe osseous destruction and compromised soft tissue quality. As a result, subsequent implant placement is often complex and may require additional guided bone regeneration.60 Furthermore, bacterial infiltration from or into adjacent teeth can extend the infection and jeopardize the health of neighboring sites
Lastly, and perhaps most importantly, implant loss carries significant psychological consequences. Concerns about appearance, combined with the additional financial burden of retreatment, can be distressing for patients and may also compromise trust in the clinician–patient relationship.59
Conclusion
It is important to shed light on this clinical phenomenon—whether described as ‘complications,’ representing a continuation of treatment, or as ‘diseases,’ reflecting a newly acquired condition—given the overwhelming number of implants and patients already affected, or likely to be affected, in contemporary implant dentistry. Across the disciplines of dentistry, there comes a point at which a tooth, or in some cases the entire dentition, is deemed to have reached its endpoint: extraction or clearance. The same caution must apply before declaring the endpoint of implant therapy, particularly when subsequent treatment may involve further implant placement. At present, there is insufficient evidence to support predictable management of peri-implant disease without considering implant removal. This reality introduces a new clinical endpoint for patients with ailing or failing implants: implant loss. In 2024, Lindhe et al. emphasized that while peri-implantitis may resemble periodontitis, it is a distinct condition whose unique nature remains poorly understood.61 He further noted that there appears to be a reluctance within the profession to openly discuss peri-implantitis, raising concern that the condition may be under-reported. At the crossroads of clinical decision-making, before declaring extraction as the endpoint, every clinician must recognize two critical realities. First, peri-implant diseases are highly site- and patient-specific. Second, once peri-implant diseases have been initiated, the successful management of peri-implant disease becomes considerably less predictable. Therefore, prevention and the early recognition of the peri-implant diseases and interventions may be a paramount of successful management. 
Oral Health welcomes this original article.
References
- Klinge B, Lundström M, Rosén M, Bertl K, Klinge A, Stavropoulos A. Dental Implant Quality Register—A possible tool to further improve implant treatment and outcome. Clin Oral Implants Res. 2018;29(April):145-151. doi:10.1111/clr.13268
- Research. GV. Dental Implants Market Size, Share & Trends Analysis Report By Implant Type (Zirconium, Titanium), By Region (North America, Europe, Asia Pacific, Latin America, MEA), And Segment Forecasts, 2023–2030.; 2022.
- RCDSO. Educational Requirements & Professional Responsibilities for Implant Dentistry. 2013;(May):1-16.
- Chang JW. New Era of the Peri-Implant Diseases. (In Oral Health – A Comprehensive Guide to Clinical Insights, Best Practices and CI, ed.). IntechOpen.; 2025. doi:https://doi.org/10.5772/intechopen.1009264
- Araujo MG, Lindhe J. Peri-implant health. J Periodontol. 2018;89(August):S249-S256. doi:10.1002/JPER.16-0424
- Etter TH, Håkanson I, Lang NP, Trejo PM CR. Healing after standardized clinical probing of the perlimplant soft tissue seal: a histomorphometric study in dogs. Clin Oral Implant Res. 2002;Dec;13(6):
- Berglundh T, Armitage G, Araujo MG, et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89(March):S313-S318. doi:10.1002/JPER.17-0739
- Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol. 2015;42(S16):S158-S171. doi:10.1111/jcpe.12334
- Derks J, Schaller D, Håkansson J, Wennström JL, Tomasi C, Berglundh T. Peri-implantitis – Onset and pattern of progression. J Clin Periodontol. 2016;43(4):383-388. doi:10.1111/jcpe.12535
- Albrektsson T, Canullo L, Cochran D, De Bruyn H. “Peri-Implantitis”: A Complication of a Foreign Body or a Man-Made “Disease”. Facts and Fiction. Clin Implant Dent Relat Res. 2016;18(4):840-849. doi:10.1111/cid.12427
- Berglundh. T. Peri-implant health, peri-implant mucositis, and peri-implantitis: European Federation of Periodontology; Guidance for clinicians. 2018:06.
- Alberts B, Johnson A, Lewis J et al. Introduction to Pathogens. In: Molecular Biology of the Cell. 4th editio. New York: Garland Science; 2002. doi:Available from: https://www.ncbi.nlm.nih.gov/books/NBK26917/
- Chang JW, Bi J, Owen G, et al. Scanning electron microscopic analysis of adherent bacterial biofilms associated with peri-implantitis. Clin Exp Dent Res. 2023;9(4):586-595. doi:10.1002/cre2.741
- Hajishengallis G, Korostoff JM. the Unknowns in Periodontal Host Response Forty Years Later. 2017;75(1):116-151. doi:10.1111/prd.12181.Revisiting
- Quirynen M, De Soete M, Dierickx K, Van Steenberghe D. The intra-oral translocation of periodontopathogens jeopardises the outcome of periodontal therapy: A review of the literature. J Clin Periodontol. 2001;28(6):499-507. doi:10.1034/j.1600-051x.2001.028006499.x
- Martinez-Amargant J, de Tapia B, Pascual A, et al. Association between smoking and peri-implant diseases: A retrospective study. Clin Oral Implants Res. 2023;34(10):1127-1140. doi:10.1111/clr.14147
- Javed, F.; Romanos GE. Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: A systematic literature review. J Periodontol.:1719–1730.
- Turri, A.; Rossetti, P.; Canullo, L.; Grusovin, M.; Dahlin C. Prevalence of peri-implantitis in medically compromised patients and smokers: A systematic review. Int J Oral Maxillofac Implant.
- Wagner, J.; Spille, J.H.; Wiltfang, J.; Naujokat H. Systematic review on diabetes mellitus and dental implants: An update. Int J Implant Dent. 2022;8, 1.
- Alsadi, W.; AbouSulaiman, A.; AlSabbagh MM. Association of dental implants success in bone density classification of postmenopausal women with osteoporosis—A clinical and radiographic prospective study. J Indian Acad Oral Med Radiol. 2021;33:428–434.
- LaMonte, M.J.; Hovey, K.M.; Genco, R.J.; Millen, A.E.; Trevisan, M.; Wactawski-Wende J. Five-year changes in periodontal disease measures among postmenopausal females: The buffalo osteoperio study. J Periodontol. 84, 572–58.
- Yip, J.K.; Borrell, L.N.; Cho, S.; Francisco, H.; Tarnow DP. Association between oral bisphosphonate use and dental implant failure among middle-aged women. J Clin Periodontol. 39,:408–414.
- Lee, C.Y.; Suzuki JB. Medication-related osteonecrosis of the jaws from once per year intravenous zoledronic acid (reclast): Report of 4 cases. Implant Dent. 24,:227–231.
- Alves, L.B.; Coelho, T.d.R.C.; de Azevedo, R.A.; Dos Santos, J.N.; Neves, F.S.; Cury PR. Systemic risk indicators for peri-implant diseases in individuals with implant-supported fixed prostheses: A cross-sectional study. Int J Oral Implant.
- Romanos, G.E.; Vaglica M. S. A. Drug-associated bone resorption with potential dental and implant implications. Periodontol 2000. (90, 236–246.).
- French D, Noroozi M, Shariati B LH. Clinical retrospective study of self-reported penicillin allergy on dental implant failures and infections. Quintessence Int. 47(10):861.
- Ting, M.; Craig, J.; Balkin, B.E.; Suzuki JB. Peri-implantitis: A comprehensive overview of systematic reviews. J Oral Implant. 44,:225–247.
- Lombardo, G.; Signoriello, A.; Pardo, A.; Romero, X.Z.S.; Sierra, L.A.V.; Tovar, L.A.; Marincola, M.; Nocini PF. Short and ultra-short (<6-mm) locking-taper implants supporting single crowns in posterior areas (part II): A 5-year retrospective study on periodontally healthy patients and patients with a history of periodontitis. Clin Implant Dent Relat Res. 24,:455–467.
- Roccuzzo, M.; Bonino, F.; Gaudioso, L.; Zwahlen, M.; Meijer HJ. What is the optimal number of implants for removable reconstructions? A systematic review on implant-supported overdentures. Clin Oral Implant Res.:229–237.
- Derks, J.; Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol.:S158—-S171.
- Misch, C.E.; Suzuki, J.B.; Misch-Dietsh, F.M.; Bidez MW. A positive correlation between occlusal trauma and peri-implant bone loss: Literature support. Implant Dent. 2005;14,:108–116.
- Misch CE. Misch’s Contemporary Implant Dentistry: Misch’s Contemporary Implant Dentistry E-Book; Amsterdam, The Netherlands,: Elsevier Health Sciences:
- Roccuzzo A, Imber JC, Salvi GE, Roccuzzo M. Peri-implantitis as the consequence of errors in implant therapy. Periodontol 2000. 2023;92(1):350-361. doi:10.1111/prd.12482
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti A., Pikos MA. et al. Implant success, survival, and failure: The international congress of oral implantologists (icoi) pisa consensus conference. Implant DentDent.
- Staubli, N.; Walter, C.; Schmidt, J.C.; Weiger, R.; Zitzmann NU. Excess cement and the risk of peri-implant disease—A systematic review. Clin Oral Implant Res. 28,:1278–1290.
- Giovannoli, J.-L.; Roccuzzo, M.; Albouy, J.-P.; Duffau, F.; Lin, G.-H.; Serino G. Local risk indicators—Consensus report of working group 2. Int Dent J. 69 (Suppl.
- Stefanini M, Marzadori M, Sangiorgi M, Rendon A, Testori T, Zucchelli G. Complications and treatment errors in peri-implant soft tissue management. Periodontol 2000. 2023;92(1):263-277. doi:10.1111/prd.12470
- Rahman B, Acharya AB, Siddiqui R, Verron E, Badran Z. Photodynamic Therapy for Peri-Implant Diseases. Antibiotics. 2022;11(7):1-17. doi:10.3390/antibiotics11070918
- Chambrone L, Wang HL, Romanos GE. Antimicrobial photodynamic therapy for the treatment of periodontitis and peri-implantitis: An American Academy of Periodontology best evidence review. J Periodontol. 2018;89(7):783-803. doi:10.1902/jop.2017.170172
- Park SH, Song YW, Cha JK, et al. Adjunctive use of metronidazole-minocycline ointment in the nonsurgical treatment of peri-implantitis: A multicenter randomized controlled trial. Clin Implant Dent Relat Res. 2021;23(4):543-554. doi:10.1111/cid.13006
- Soriano-Lerma A, Magán-Fernández A, Gijón J, et al. Short-term effects of hyaluronic acid on the subgingival microbiome in peri-implantitis: A randomized controlled clinical trial. J Periodontol. 2020;91(6):734-745. doi:10.1002/JPER.19-0184
- Machtei EE, Romanos G, Kang P, et al. Repeated delivery of chlorhexidine chips for the treatment of peri-implantitis: A multicenter, randomized, comparative clinical trial. J Periodontol. 2021;92(1):11-20. doi:10.1002/JPER.20-0353
- Blanco C, Pico A, Dopico J, Gándara P, Blanco J, Liñares A. Adjunctive benefits of systemic metronidazole on non-surgical treatment of peri-implantitis. A randomized placebo-controlled clinical trial. J Clin Periodontol. 2022;49(1):15-27. doi:10.1111/jcpe.13564
- Ramanauskaite A, Fretwurst T SF. Efficacy of alternative or adjunctive measures to conventional non-surgical and surgical treatment of peri-implant mucositis and peri-implantitis: a systematic review and meta-analysis. Int J Implant Dent.
- Alqahtani F, Alqhtani N CS. Efficacy of Nonsurgical Mechanical Debridement With and Without Adjunct Low-Level Laser Therapy in the Treatment of Peri- Implantitis: A Randomized Controlled Trial. J Oral Implant. 46(5):526-.
- Hentenaar DFM, De Waal YCM, Stewart RE, Van Winkelhoff AJ, Meijer HJA, Raghoebar GM. Erythritol air polishing in the surgical treatment of peri-implantitis: A randomized controlled trial. Clin Oral Implants Res. 2022;33(2):184-196. doi:10.1111/clr.13881
- Khan SN, Koldsland OC, Roos-Jansåker AM, et al. Non-surgical treatment of mild to moderate peri-implantitis using an oscillating chitosan brush or a titanium curette—A randomized multicentre controlled clinical trial. Clin Oral Implants Res. 2022;33(12):1254-1264. doi:10.1111/clr.14007
- Daubert D, Lee E, Botto A, Eftekhar M, Palaiologou A, Kotsakis GA. Assessment of titanium release following non-surgical peri-implantitis treatment: A randomized clinical trial. J Periodontol. 2023;94(9):1122-1132. doi:10.1002/JPER.22-0716
- Mayer Y, Khoury J, Horwitz J, et al. A novel nonsurgical therapy for peri-implantitis using focused pulsed electromagnetic field: A pilot randomized double-blind controlled clinical trial. Bioelectromagnetics. 2023;44(7-8):144-155. doi:10.1002/bem.22481
- Acar B, Guncu GN. Current status and management of peri-implantitis: A systematic review. Prim Dent J. 2024;13(4):77-92. doi:10.1177/20501684241270111
- Tavelli L, Barootchi S, Avila-Ortiz G, Urban IA, Giannobile WV WH. Peri-implant soft tissue phenotype modification and its impact on peri-implant health: A systematic review and network meta-analysis. J Periodontol. 2021;Jan;92(1):
- Herrera D, Berglundh T, Schwarz F, et al. Prevention and treatment of peri-implant diseases—The EFP S3 level clinical practice guideline. J Clin Periodontol. 2023;50(S26):4-76. doi:10.1111/jcpe.13823
- Chang HY, Park SY, Kim JA, Kim YK, Lee HJ. Early radiographic diagnosis of periimplantitis enhances the outcome of peri-implantitis treatment: A 5-year retrospective study after non-surgical treatment. J Periodontal Implant Sci. 2015;45(3):82-93. doi:10.5051/jpis.2015.45.3.82
- Wijesundara S, A. Sharma L, Alavi SE, Sharma A. applied sciences Peri-Implantitis Therapy Using Surgical Methods : Mdpi. 2023;13(5):1-18.
- Schwarz F, Jepsen S, Herten M, Sager M, Rothamel D, Becker J. Influence of different treatment approaches on non-submerged and submerged healing of ligature induced peri-implantitis lesions: An experimental study in dogs. J Clin Periodontol. 2006;33(8):584-595. doi:10.1111/j.1600-051X.2006.00956.x
- Wen SC, Barootchi S, Huang WX, Wang HL. Surgical reconstructive treatment for infraosseous peri-implantitis defects with a submerged healing approach: A prospective controlled study. J Periodontol. 2022;93(2):195-207. doi:10.1002/JPER.21-0161
- Dalago HR, Perrotti V, Torres de Freitas SF, Ferreira CF, Piattelli A, Iaculli F BM. Prospective longitudinal comparison study of surgical therapies for peri-implantitis: 3-year follow-up. Aust Dent J. 2019;Sep;64(3):
- Giannobile W V., Jung RE, Schwarz F. Evidence-based knowledge on the aesthetics and maintenance of peri-implant soft tissues: Osteology Foundation Consensus Report Part 1—Effects of soft tissue augmentation procedures on the maintenance of peri-implant soft tissue health. Clin Oral Implants Res. 2018;29(November 2017):7-10. doi:10.1111/clr.13110
- Insua A, Monje A, Wang H, Inglehart M. Patient‐Centered Perspectives and Understanding of Peri‐Implantitis. J Periodontol. 2017;88(11):1153-1162. doi:10.1902/jop.2017.160796
- Anitua E, Montalvillo A, Eguia A, Alkhraisat MH. Clinical outcomes of dental implants placed in the same region where previous implants failed due to peri-implantitis: a retrospective study. Int J Implant Dent. 2021;7(1):1-7. doi:10.1186/s40729-021-00392-1
- Lindhe J, Romandini M. Periodontology: The Past, the Present, the Future. J Periodontal Res. 2025;60(1):1-5. doi:10.1111/jre.13370
About the author

Dr. Chang is a dentist with experience of 25 years in Etobicoke. He graduated from the Faculty of Dentistry, University of Western Ontario in 2000. Starting in 2002 with Dr. George Zarb’s residency at the University of Toronto, he completed master of oral implantology, J.W. Goethe University (Germany) in 2015 and pursued full-time ‘Periodontics’ specialty training at the University of British Columbia in 2018. He holds a fellow status with the RCDC and a diplomate status with ABP/ICOI. He is involved with ITI as Director of Toronto Study Club/Academy editor. He has a periodontics clinic in Etobicoke. www.etobicokeperio.ca