
Technological advancement impacts every single aspect of our lives, and has greatly benefited the dental industry, including significant evolutions in the orthodontic field. These developments incorporate treatments with removable and fixed devices that are used in a variety of cases from different age groups, following concepts from both the European and American trends in orthodontic therapy.
The Shaw Lab team began to develop a Digital Orthodontic Department and Clear Aligners workflow in 2016. Now known as PerfectSmile Aligners by Shaw, a fully Canadian clear aligner system, the team required the answer to a key question.
How can the best results be established with PerfectSmile?
The versatility of these devices allows advance planning to successfully treat a wide variety of cases with all the advantages of using removable appliances. Unlike wearing fixed braces, the aligner patient can eat all kinds of foods, can have better plaque control resulting in decreased gum inflammation, and suffers less post-treatment enamel decalcification, among other advantages.
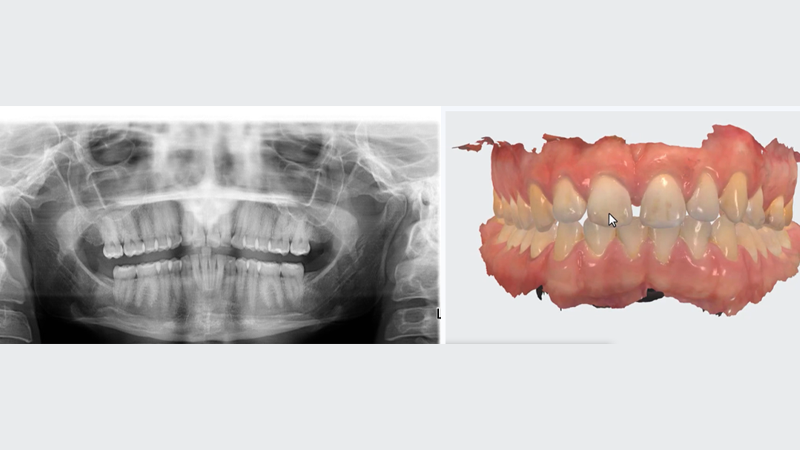
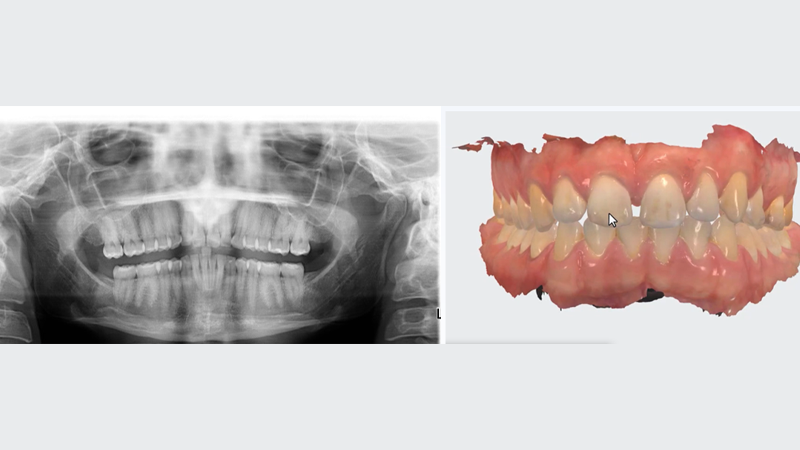
It must be remembered that aligners are a removable orthodontic force system and, as such, utilize mechanics in which those forces are applied to the teeth and periodontal structures in a discontinuous protocol, while fixed braces exert continuous, long-term forces. Thus, the mechanics of aligners must be carefully designed to function effectively and efficiently during the sequential treatment steps to maximize results. (Figs. 1, 2)
Fig. 1
Fig. 2

READ: Effectiveness and predictability of clear aligner therapy
The PerfectSmile team of orthodontic designers takes into consideration many factors that have proved to be the keys to highly successful treatment outcomes. Some of these factors are:
Full treatment design
The treatment plan is designed from the initial situation to the desired end result following the treatment goals stated in the Case Submission Form. The entire comprehensive treatment plan must be established from the very beginning.
Proper staging
The development of a sequential series of orthodontic movements in which:
- Not all the teeth move at the same time.
- The individual tooth movements do not interfere with each other.
- Any required interproximal reduction is scheduled during the treatment process to be performed with greater direct access and, preferably, without altering the anatomical features of the dentition.
Tooth anchorage value
These are coefficients based on the amount of root surface embedded in the alveolar bone and each tooth’s resistance to orthodontic movement. The aligners are designed to utilize portions of the dental arch as anchorage while other teeth in the arch are being actively moved.
Other considerations
There is an absolute need for a proper diagnosis and clearly defined realistic treatment goals for all orthodontic treatment, regardless of the technique.1 While the diagnosis reflects the assessment of the anomaly and must be quite precise, the treatment goals vary according to different circumstances. They can be established within a range from the simple improvement of the alignment of the anterior teeth to the comprehensive correction of a complex malocclusion. The treatment goals should be clearly stated when the case is submitted.
The patient’s expectations for the treatment outcome must be considered in the context of the treatment goals. Some of these expectations may be related to their current perception of esthetics, cultural environment and the heavy impact of advertising and social media. These expectations need to be thoroughly discussed with the provider as they may not be compatible with biology, not realistic, and potentially, not fully attainable.
A set of foundational principles should apply to guide the workflow.
Primum non nocere: First do no Harm
This strong message teaches that “First, do not harm” or “Above all else, do not harm”.2 In other words, before doing anything to a patient, be certain that the treatment is not making matters worse. (This injunction, often attributed to Hippocrates, is actually not in the Hippocratic Oath, but is believed to have been derived from it. It is attributed to an English physician, Thomas Sydenham.)
Individuality
Rather than setting strict protocols for the treatment design of specific anomalies, the aligner team must follow general guidelines as moderated by the individual characteristics of each case. Humans differ in age, gender, skeletal structure, tooth shape and size, patient biotype, dental bone discrepancy, etc., and all these factors must be considered in the treatment planning with an eye on the requested treatment goals. These guidelines, formulated by the scientific foundations of orthodontic concepts, drive the aligner designers to adjust the mechanics for each individual case.
As an example: the facial biotype is defined by skeletal structure and mandibular growth patterns, and it determines a completely different approach for the aligner design depending on whether the case is Brachyfacial or Dolichofacial. These two biotypes exhibit differences in masticatory musculature, bite force, skull and mandibular shape, in their tendency to present certain anomalies and their prognosis.3,4 Therefore, their response to designed mechanics such as extrusive dental movements, dental-alveolar expansion, pro inclination, etc. will be also different.5,6,7
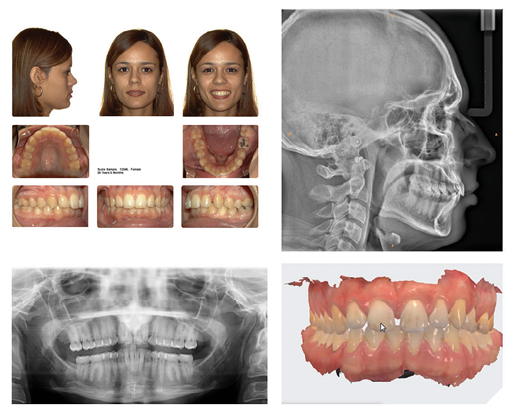
It clearly shows why it is so important that all the patient’s orthodontic records or as many of them as possible, must be submitted to the aligner team at the dental laboratory. This information includes facial and intraoral photos, panoramic and lateral cephalogram radiographs, etc. (Fig. 3).
Fig. 3
The ultimate objective is to create a team consisting of the dental provider and the aligner designers to explore the patient’s existing condition, clinical possibilities, and design a treatment plan to accomplish the treatment goals. This coordination requires a diagnostic process, a detailed prescription, a knowledgeable designer team, and the utilization of the latest technologies in software, 3D printing, processing, and manufacturing with the best materials. Clear and continuous communication among the team members will greatly contribute to the quality and success of the orthodontic treatment plan. 
Oral Health welcomes this original article.
Disclosure: Dr. Manay is a PerfectSmile Orthodontic Consultant for Shaw Lab Group, North York, Ontario.
References
- Facial morphology and malocclusions. Christian Bittner, Hans Pancherz. American Journal of orthodontics and Dentofacial Orthopedics Vol 97, Issue 4 April 1990
- Origin and uses of Primum non nocere-above all, do not harm. Cedric Smith. J Clin Pharmacol. 2005 Apr;45(4):371-7
- Association between transverse collapse of the maxilla and facial biotype by Cone Beam tomography. Carlos Adrian Escobedo- Camacho, Guillermo Perez Cortez and others. EAS Journal of Dentistry and Oral Medicine Volume 5 Issue 6 Nov. Dec 2023
- Lower incisor inclination in relation to facial Biotype in Skeletal Class I patients. Rafael Mora Hurtado, maria Eugenia Vera Serna, Eileen Uribe -Querol. Revista Mexicana de Ortodoncia. 2016; vol 4 Issue 3 pages e157-e 162
- The influence of extraction and non-extraction orthodontic treatment on Brachyfacial and Dolichofacial growth patterns. L Klapper, S F Navarro, D bowman, B Pawlowski. Am J Orthod Dentofacial Orthop. 1992 May:101(5):425-30
- Analysis of the association between facial biotype, overbite and overjet in the permanent dentition. Liz Chite-Quispe, Marco Sanchez- Tito J Clin Exp Dent 2023; 15(5):376-81
- Effects of premolar extraction and orthodontic treatment in adolescents- a retrospective cephalometric study. Maria Ekstam, Mikael Sonesson, Kristina Hellen-Halme. Acta Odontol Scand, 2024 Mar 26:83:92-100.
About the author

Dr. Manay graduated with a DDS from the University of Uruguay where he received his Post Grad training in Orthodontics and Dental Maxilla Facial Orthopedics and was a Tenured Assistant Professor in Orthodontics. Formerly Head of Dentistry, Ministry of Public Health, Uruguay, he is Co-author of Fundamentals & Principles, Dental-Maxilla-Facial Orthopedics, and has lectured in Canada, Uruguay, Italy, Argentina, Brazil and Ecuador.