


In 2021–2022, 58% of dying Canadian patients received palliative care or a form of palliative care.1 Palliative care dentistry has been defined as the treatment of terminally ill patients in whom the oral cavity is affected directly or indirectly by the illness, and the principle of care is symptom relief.2 The oral cavity may be affected by either the disease itself or by the side-effects of treatments and medications, and this causes additional pain and suffering which contribute to further diminish the quality of life of the patient. The oral cavity of the palliative patient is often compromised by xerostomia, opportunistic infections such as fungal and viral infections, and mucositis.3 This paper will describe the causes of oral pain in the palliative patient and the important role of the palliative care dentist in the treatment of oral pain to reduce suffering in the patient’s final days.
The oral status of all patients admitted to palliative care should be routinely assessed upon admission. The patient should be asked if they are experiencing any oral/dental pain or dryness of the mouth. This should be followed by an initial look inside the oral cavity. This can be done by a nurse or physician. The attending dentist can also perform the initial assessment or can be called in subsequently to provide care when the initial assessment shows evidence of infection, decay, or xerostomia. The healthcare team should ensure that the oral cavity is as clean as possible and should promote good oral hygiene. The patient’s family and/or caregivers, if they are agreeable, should be assistive in the provision of oral care. This will lessen the chance of potential decay and complications, and make the patient feel more comfortable and cared for. All mouth rinses should be alcohol-free to avoid desiccating the mouth.
Based on his experience treating palliative care patients, the author developed the criteria to be evaluated and applied in providing dental care to the palliative patient. These are known as “the CARE principle:”4
C: the treating dentist must evaluate the oral status of the patient and provide Comfort measures;
A: Assessment of the changing health and dental status; and
RE: REality; dictating the treatment plan based upon the patient’s life expectancy.
Related article: Informed consent in the absence of capacity: A case-based exploration
A clinical example of the application of these criteria is as follows: A palliative care patient is self-conscious about a missing central incisor and refuses to see their family members. This patient may benefit from low-cost treatments such as a “flipper” transitional denture or a tooth added to an Essix retainer versus higher priced permanent solutions such as a fixed bridge or an implant. The CARE criteria dictate that the dentist must consider the reality of the patient’s condition and dictate the choice of the low-cost treatment which will provide the desired result of improving the patient’s self-image allowing him to see his family. While the higher priced permanent fixed bridge or implant will provide the desired results, the ethics of placing these in a terminal patient is questionable.
Xerostomia is one of the most frequent side-effects associated with the analgesics administered to the terminally ill.5 The lack of saliva affects the patient’s ability to eat, swallow, and talk, and causes much pain and bleeding.
Case 1
Mrs. A. suffered from advanced cancer with metastasis to both bones and other organs. She was admitted to the palliative care unit and was examined by the author. She was being given a high dosage of opioids which caused her mouth to be extremely dry. This led to spontaneous bleeding from the corners of her mouth and to her tongue and lips “sticking” to the oral tissues (Fig. 1). Mrs. A. was treated with a water-soluble lubricant (e.g., Mukogelly®, K-Y Jelly®, Taro Gel®) using a foam toothbrush. This relieved her sensation of dryness, making her more comfortable and peaceful, and improved her quality of life in her final days.
Fig. 1

Opportunistic infections are often seen in the palliative care patient. These infections are attributable to the compromised immune systems of these patients which result from the disease process itself and/or the treatments and medications used to combat the disease.
Case 2
Mr. B., with advanced prostate cancer, complained of a terrible toothache. Clinically, tooth #47 revealed a large carious lesion. In addition, the patient had a herpes infection, both intraoral and extraoral (Fig. 2,3). The patient wanted the tooth extracted. The palliative care dentist in conjunction with the physician decided to treat the patient with an antibiotic and an antiviral prior to the extraction. The patient received amoxicillin (500 mg three times daily for 7 days), and acyclovir (400 mg 5 times daily for 7 days). To aid in pain relief a 50:50 suspension of diphenhydramine elixir with Kaopectate was applied to the lesions and a 2% viscous lidocaine rinse was also prescribed.6,7 The herpes simplex infection resolved and the tooth was extracted. The patient’s quality of life improved significantly and he spent his remaining days without oral pain.
Fig. 2

Fig. 3

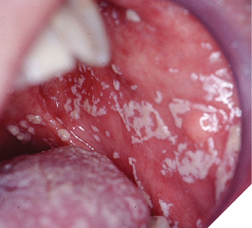
Fungal infections occur frequently in palliative patients.8 Fungus infection causing organisms, such as Candida albicans, are normally found in the oral microbiome of healthy patients; however, their numbers are kept in check due to the competition for growth by other coexisting organisms and by the mouth’s immune system. In medically compromised patients, the eubiosis or delicate balance of the oral microbiome is upset, thus allowing the fungus causing organisms to multiply rapidly. There are multiple contributory factors for the prevalence of fungal infections in the palliative patient including the disease itself, the immunocompromised status and xerostomia resulting from radiation treatments and/or the medications used to treat the patient (Fig. 4). Treatments for fungal infections include the use of local agents such as nystatin rinses (swish 100,000 IU 5 ml every six hours then swallow or expectorate for 1-2 weeks), and clotrimazole troches (10 mg three times a day for 1-2 weeks). Troches may not be as effective in a patient with xerostomia as they will not easily dissolve due to the lack of saliva. Systemic agents such as fluconazole should be used with extreme caution as they affect the metabolism of many medications, including but not limited to midazolam and fentanyl, leading to toxic levels. In a denture-wearing patient, in addition to treating the mouth, the dentures should be scrupulously cleaned and soaked in a nystatin solution to decrease the fungi present in the acrylic of the denture.4
Fig. 4
Chemotherapy and/or radiotherapy, initially prescribed for a non-surgical treatment of cancer, may be extended during the palliative care process to decrease pain or improve function. Both chemotherapy and radiotherapy negatively affect the tissues of the mouth and cause mucositis.9 Mucositis is associated with ulceration of the oral tissues and infection by opportunistic pathogenic organisms. Patients with head and neck cancers are at a high risk of developing mucositis.9 A key element in mucositis prevention is to keep the mouth moist and clean. Oral care can minimize the incidence of mucositis by preventing or minimizing secondary infections.10 Topical anaesthetic agents may be used to alleviate pain but are not well tolerated as these agents may affect the gag reflex and cause distress to the patient. The discomfort caused by mucositis may be so severe that it may affect the patient’s ability to eat and swallow, and this, in turn, may lead to increases in opioid dosing. Unfortunately, increasing the opioids will worsen the patient’s xerostomia. It is essential therefore to maintain good oral hygiene and keep the mouth lubricated. An alternative non-opioid treatment for the pain associated with mucositis is using honey to coat the oral tissues.11
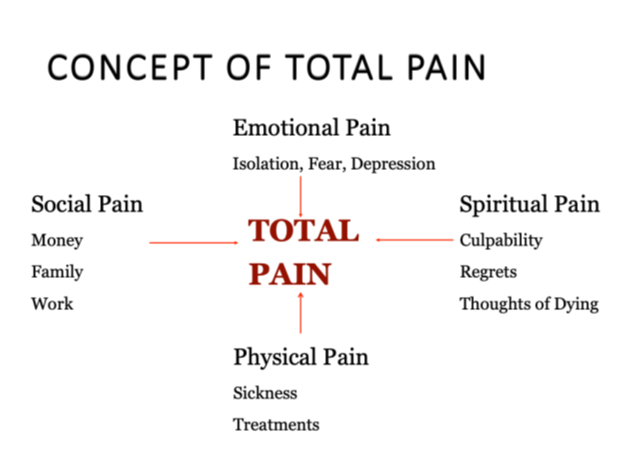
In providing care, the treating dentist must consider the whole patient and his/her subjective pain. It is important for the dentist to understand the emotional dynamics of total pain. As described by Dame Cicely Saunders, “Total pain is a combination of physical pain, social pain, emotional pain, and spiritual pain.”12 (Fig. 5) The dentist must be prepared and know how to deal with a patient’s emotions, whether it be anger or sadness and tears. An example of treating total pain is outlined in Case 3.
Fig. 5
Case 3
Mrs. C was a 77-year-old patient admitted to the palliative care unit around Christmas time. The author was called in to perform an initial assessment of her oral status. During the assessment she mentioned that she regretted not being able to make Christmas cookies. Since he had no other patients scheduled, the author went to the hospital kitchen and brought up the ingredients to make the cookies. He then assisted the patient in making the cookies which were baked in the oven. The patient suffered from loss of appetite and anorexia, which at this phase of her terminal illness are very common. The cookies brought much joy to the patient. Her husband relayed that all weekend long she only talked about the cookies, and all weekend long, all she ate were the cookies. She died before Christmas, but her husband sent the author a card thanking him for making the last weeks of his wife’s life meaningful.
The dentist plays an important role in contributing to improve the quality of life of patients in palliative care. Dental treatment and preventive therapies should not come to an end when a patient receives a terminal diagnosis. Dental treatment (including extractions if required to reduce pain) should be provided, but must be modified to meet the patient’s needs. Xerostomia, oral fungal infections, and mucositis all cause additional significant pain to patients who are already suffering tremendous pain. The aim of all dental treatments in palliative care dentistry is to reduce oral pain, thereby improving the patient’s quality of life. The dentist must understand the emotional dynamics of the patient’s total pain and communicate effectively to help alleviate the patient’s anxiety and oral pain. By treating the palliative patient’s oral pain, the dentist contributes to the improvement of the patient’s quality of life, enabling the patient to eat, drink, speak and finally kiss their loved-ones good-bye. 
Oral Health welcomes this original article.
References
- https://www.cihi.ca/sites/default/files/document/access-to-palliative-care-in-canada-2023-report-en.pdf
- Wiseman M. Palliative care dentistry. Gerodontol 17:49-51, 2000.
- Sonis ST, Sonis AL, Lieberman A. Oral complications in patients receiving treatment for malignancies other than of the head and neck. JADA 97:468-72, 1978.
- Wiseman M. Palliative Care Dentistry. In: Geriatric Dentistry: Caring for Our Aging Population (ed. Paula K Friedman) pp 17-28, 2014 Wiley Blackwell, Ames Iowa.
- Jobbins J, Bagg J, Finlay IG et al. Oral and dental disease in terminally ill cancer patients. BMJ 304:1612- 1992.
- Ajar AH, Chauvin PJ. Acute Herpetic Gingivostomatitis in Adults: A Review of 13 Cases, Including Diagnosis and Management. J Can Dent Assoc 68(4):247-51, 2002.
- Hopper SM, Babl FE, McCarthy M, Tancharoen C, Lee KJ, Oakley E. A double blind, randomised placebo-controlled trial of topical 2% viscous lidocaine in improving oral intake in children with painful infectious mouth conditions. BMC Pediatr. 11:106-13, 2011.
- Astvad K, Johansen HK, Hoiby N, Steptoe P, Ishoy T. Oropharyngeal Candidiasis in Palliative Care Patients in Denmark. J Palliat Med. 18(11):940-4, 2015.
- Anderson, C, Saunders, D. Oral Mucositis in Head and Neck Cancer Patients. Semin Radiat Oncol. 35(2):271-277, 2025.
- Sonis S, Kunz A. Impact of improved dental services on the frequency of oral complications of cancer therapy for patients with non-head-and-neck malignancies. Oral Surg Oral Med Oral Path 65:19-22, 1988.
- Anshasi H, Abufarsakh B, Alkhawaldeh JM, Halalmeh SA. Honey for managing oral mucositis induced by cancer therapies: An overview of systematic reviews. Complement Ther Med. 92:103197, 2025.
- Saunders C. The evolution of palliative care. Patient Educ Couns 41:7-13, 2000
About the author

Dr. Michael Wiseman completed his dental degree in 1985 at McGill University. He presently is a part-time Clinical Associate Professor at McGill University Faculty of Dental Medicine and Oral Sciences. He has a full-time practice, and additionally provides care at a variety of long-term hospital centres in Montreal. He is the Founder of the McGill Outreach Program which provides free care to the needy of Montreal. Dr. Wiseman has lectured nationally and internationally and has published many peer reviewed papers and book chapters.