


Abstract
This article describes the orthodontic management of an adult patient with mandibular asymmetry, maxillary occlusal canting, and a functional mandibular shift. The patient had previously undergone comprehensive orthodontic treatment but was dissatisfied with the outcome. A thorough diagnostic with cone-beam computed tomography (CBCT) allowed detailed assessment of occlusal plane canting and skeletal asymmetry. This report highlights the importance of an accurate differential diagnosis, the critical role of CBCT in evaluating skeletal and dental discrepancies, and the application of temporary anchorage devices (TADs) to enable non-surgical orthodontic treatment in a borderline Class III case.
Facial asymmetry and maxillary occlusal canting represent challenging dentofacial discrepancies with significant implications in facial esthetics and functional occlusion.1,2 In many cases, a functional mandibular shift—often caused by occlusal interferences—can exaggerate the apparent severity of the malocclusion when the patient is evaluated in Centric Occlusion (CO), potentially leading to diagnostic inaccuracies and inappropriate treatment decisions.2 Assessment in Centric Relation (CR) is critical to distinguish true skeletal discrepancies from functional adaptations.3 This diagnostic approach allows clinicians to recognize anatomical limitations, determine the suitability of compensatory orthodontic treatment versus orthognathic surgery, and formulate a more individualized and effective treatment plan.
The use of CBCT supports precise three-dimensional assessment of skeletal morphology, occlusal plane inclination, and temporomandibular joint position.4,5 It enhances diagnostic accuracy and guides biomechanical planning, particularly in complex or borderline cases. When combined with the strategic use of TADs, certain borderline Class III cases can be managed non-surgically while achieving stable, functional and esthetic results.6
This case report highlights how comprehensive diagnosis, supported by CBCT imaging and TAD assisted biomechanics, facilitated the successful non-surgical management of an adult patient with mandibular asymmetry and maxillary occlusal canting.
Case presentation
A 31-year-old male presented with facial asymmetry and a canted maxillary occlusal plane. Despite previous comprehensive orthodontic treatment during adolescence, he remained dissatisfied with the esthetic and functional outcomes. Preferring to avoid orthognathic surgery, he sought evaluation for a non-surgical orthodontic alternative.
Read related article: Facial Recognition and Corrective Jaw Surgery
Clinical examination
Extraoral evaluation revealed lower facial asymmetry, with mandibular deviation to the left and maxillary occlusal canting, evidenced by a tilted smile line. In CO, intraoral examination showed bilateral Class I malocclusion. The mandibular dental midline was deviated 4.5 mm to the left of the facial midline, while the maxillary midline showed a 1.5 mm leftward deviation. Mild crowding was present in the lower anterior region (Fig. 1).
Fig. 1
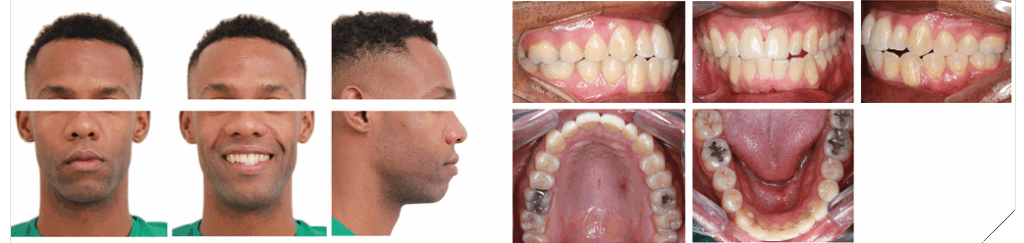
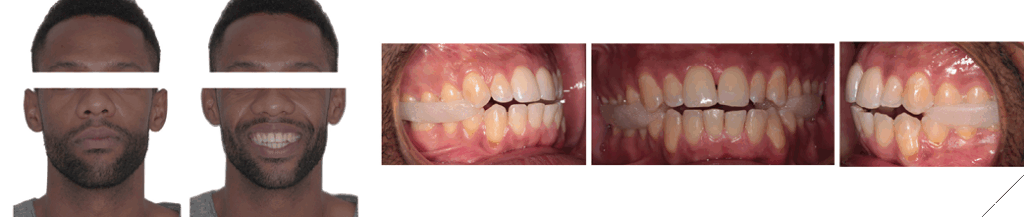
A functional mandibular shift was confirmed during clinical examination. To accurately assess the patient in CR, bilateral occlusal jigs were employed during CBCT acquisition to stabilize the mandible and ensure reproducibility of the jaw position. This approach allowed more precise evaluation of skeletal and dental relationships. In CR, a Class III subdivision right malocclusion was observed. The mandibular midline remained deviated 3 mm to the left, accompanied by an anterior open bite (Fig. 2).
Fig. 2
Radiographic evaluation
- Panoramic Radiograph: No signs of condylar asymmetry or temporomandibular joint pathology were observed (Fig. 3).
- Lateral Cephalometric Radiograph: Demonstrated bimaxillary protrusion, proclined mandibular incisors, a Skeletal Class III tendency, and a hyperdivergent facial pattern (Fig. 4).
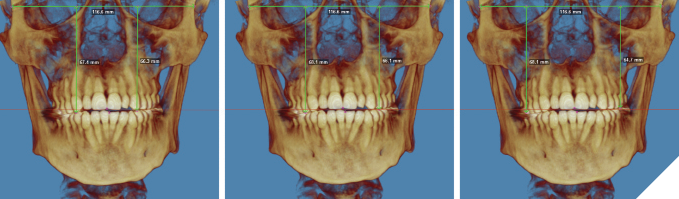
- CBCT: Revealed maxillary occlusal canting and mandibular skeletal asymmetry (Fig. 5).
Fig. 3
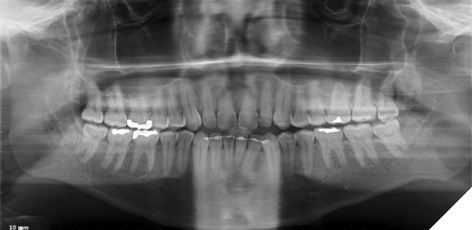
Fig. 4
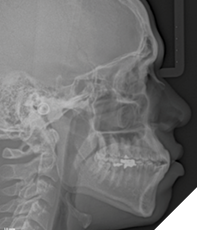
Fig. 5
Diagnosis
- Skeletal Class III tendency with mandibular asymmetry and and Hyperdivergent facial pattern
- Functional mandibular shift due to occlusal interferences
- Maxillary occlusal canting
- Class III subdivision right malocclusion
- Dentoalveolar proclination of the mandibular incisors
- Anterior open bite
- Bimaxillary protrusion
- Mild crowding
Treatment objectives
- Eliminate the mandibular functional shift
- Level the maxillary occlusal plane
- Correct the Class III dental malocclusion
- Reduce the dentoalveolar proclination of the mandibular incisors
- Correct the anterior open bite
- Reduce the bimaxillary protrusion and establish a harmonious and esthetic smile arc
- Alignment of the dentition
Treatment plan
Compensatory, non-surgical, comprehensive orthodontic therapy with full fixed appliances was planned, incorporating insertion of TADs in the Maxilla (Fig. 6) and posterior Mandible (Figs. 7-8) to facilitate vertical control during occlusal plane correction and, to provide absolute anchorage during asymmetric retraction of mandibular teeth in association with lower incisor decompensation, respectively. Extraction of all third molars was recommended prior to initiating retraction mechanics to leverage the regional acceleratory phenomenon (RAP) and enhance tooth movement efficiency.
Fig. 6
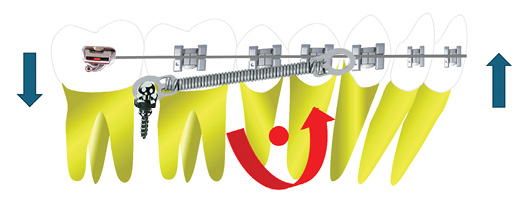
Fig. 7
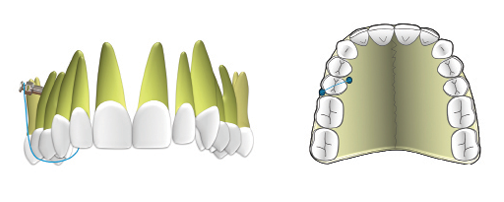
Fig. 8

Discussion
The management of skeletal Class III malocclusions accompanied by facial asymmetry and occlusal plane canting requires a comprehensive diagnostic approach to determine the appropriate treatment modality, whether orthodontic camouflage or orthognathic surgery. While severe skeletal discrepancies typically require surgical intervention, borderline cases may be effectively managed non-surgically with the support of precise imaging and advanced biomechanical techniques.1,2,3 CBCT has become a cornerstone in diagnosing complex asymmetries and occlusal discrepancies, allowing for detailed visualization of hard tissue structures and skeletal relationships.2,4,5
In cases with functional mandibular shifts, premature occlusal contacts in CO may obscure the true skeletal relationship, increasing the risk of misdiagnosis.3 Therefore, assessment in CR is essential. In this case, the use of occlusal jigs during CBCT acquisition allowed for mandibular stabilization in CR and more accurate evaluation of skeletal and dental relationships.
Traditional Class III camouflage often relies on intermaxillary elastics, which are patient-dependent and can introduce unfavourable outcomes such as upper molar extrusion, incisor flaring, and occlusal plane rotation.6 For this patient, such mechanics were contraindicated due to pre-existing upper molar extrusion in the first quadrant and the need to avoid further maxillary incisor proclination.
TADs provide a reliable, compliance-free anchorage allowing clinicians to control tooth movement more precisely and minimize undesirable side effects associated with traditional orthodontic mechanics. Their advantages – particularly mini-implants – include affordability, minimally invasive placement under local anesthesia, immediate loading, and suitability for use in a private practice setting (Fig. 8). These attributes make mini-implants a practical option for patients seeking non-surgical orthodontic alternatives.1,6,7
Our primary treatment objectives included correction of the dental classification, lower incisor proclination, and closure of the anterior open bite through targeted mandibular unilateral retraction. Furthermore, the maxillary occlusal cant – with a discrepancy of 1 mm in the canine region, 2 mm in the premolar region, and 3 mm in the molar region (Fig. 5) – was addressed through localized intrusion of the maxillary posterior right quadrant using inter-radicular mini-implants placed palatally between teeth #14 and #15, and buccally between teeth #15 and #16 (Fig. 6).5,6 The timing of third molar extraction was synchronized with the onset of retraction forces to leverage RAP and accelerate the biological response to tooth movement.4 This strategy contributed to efficient decompensation of the mandibular incisors and correction of the occlusal plane.
This approach demonstrates the effectiveness of mini-implant supported biomechanics in correcting minor occlusal plane canting by providing precise vertical control and facilitating targeted retraction and retroclination of the lower incisors, thereby improving both functional and esthetic outcomes1,6,7 (Figs. 9-12).
Fig. 9

Fig. 10
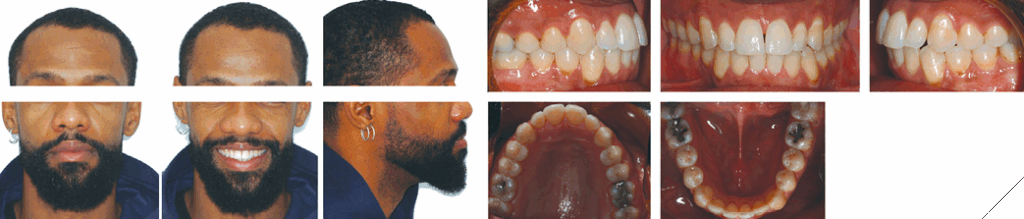
Fig. 11

Fig. 12

The total treatment time was 32 months. Bilateral Class I molar and canine relationships were achieved along with ideal overjet and overbite, and significant improvement of maxillary and mandibular midline alignment. Notably, the smile arc and incisor positioning were enhanced (Figs. 10-12). Cephalometric evaluation confirmed improvements in incisor angulation, sagittal dental relationships, and vertical control (Fig. 12). As this was a compensatory treatment, the underlying skeletal mandibular asymmetry remained; however, the dental and occlusal corrections resulted in a satisfactory outcome.
Conclusion
In select borderline Class III cases presenting with facial asymmetry and functional mandibular shift, non-surgical management can be a viable and effective option. The integration of CBCT imaging and TAD supported biomechanics enables clinicians to design precise, individualized treatment plans that deliver esthetic and functional results without the need for orthognathic surgery. This case demonstrates how thoughtful diagnosis and modern orthodontic tools can successfully resolve complex asymmetries and occlusal challenges in adult patients. 
Oral Health welcomes this original article.
References
- Kim HJ, Noh HK, Park HS. Nonsurgical orthodontic correction of facial asymmetry by condylar remodeling and mandibular repositioning following occlusal cant correction with micro-implants: a case report. Angle Orthod.2023;93(1):111–125
- Kim HJ, et al. Mandibular asymmetry types and dental compensations analyzed with CBCT. Angle Orthod.2023;93(6):695–705
- Facial asymmetry revisited: diagnostic accuracy with CR evaluation. Semin Orthod. 2018;24(3):196–204 .
- Kim MS, Lim SH, Jeong SR, Park JH. Maxillary molar intrusion and transverse decompensation to enable mandibular single-jaw surgery in mandibular prognathism with asymmetry. Am J Orthod Dentofacial Orthop.2020;157(6):818–831
- Seminars in Orthodontics review of non-surgical occlusal cant correction using TADs, supporting CBCT-guided anchorage mechanics
- Park HS, Kim JY, Kwon TG. Correction of roll-type asymmetry using miniscrews: clinical utility in borderline cases. AJODO 2020;157(6):818–831
- Kim HJ, et al. Mandibular asymmetry types and dental compensations analyzed with CBCT. Angle Orthod.2023;93(6):695–705.
About the authors

Dr. Aura Sofia C. Manfio is a Specialist in Orthodontics (University of British Columbia / PUCRS). She holds a Master’s degree from the University of São Paulo and completed a Craniofacial Orthodontics fellowship at the Hospital for Sick Children in Toronto. She is currently engaged in private practice in Ontario, Canada. Contact: aurasofia.manfio@gmail.com

Dr. Bruno Nehme Barbo is a Specialist in Orthodontics with a Master’s and Doctorate degree from the Pontifical Catholic University of Rio Grande do Sul (PUCRS). He serves as a faculty member at PUCRS and maintains an active private practice in southern Brazil. Contact Information: bruno.barbo@hotmail.com