

Abstract:
Objective: To address the challenges and solutions involved in restoring a dental implant palatally placed in the esthetic zone.
Background: Proper implant placement in the esthetic zone is essential for achieving optimal functional and esthetic results, however, ideal placement is not always possible. Implants positioned too palatal can lead to esthetic concerns such as poor buccal contour and a suboptimal emergence profile.
Methods: A 41-year-old female patient presented with a maxillary anterior dental implant replacing tooth 22 that was placed too palatal, potentially affecting the esthetic and functional outcome. The treatment plan included soft tissue management, emergence profile development with provisional crown fabrication, and a customized final impression approach. The soft tissues were relieved and moved around the implant with a surgical blade. A chair-side screw-retained provisional crown was fabricated to train and develop the restoration’s emergence profile and improve the esthetic outcome. The final prosthesis consisted of a screw-retained porcelain-fused-to-metal crown that replicated natural tooth morphology and achieved a more balanced esthetic result.
Results: The restorative approach successfully improved the implant site’s esthetics. The emergence profile was optimized, leading to a more natural appearance. The patient expressed high satisfaction with the outcome, and there were no significant complications during follow-up.
Conclusion: Management of a palatally placed implant in the esthetic zone requires a comprehensive approach involving soft tissue management and emergence profile development. This case demonstrates that with appropriate techniques, effective esthetic outcomes can be achieved even when initial implant placement is suboptimal
Introduction
Achieving optimal functional and esthetic outcomes in implant dentistry requires meticulous attention to implant placement, particularly in the esthetic zone. The positioning of dental implants in this area is critical not only for ensuring adequate functional integration but also for achieving desirable esthetic results.1 Proper implant placement is fundamental to creating a harmonious relationship between the implant, surrounding soft tissues, and adjacent natural teeth.1
However, ideal implant placement is not always feasible. Implants positioned suboptimal in the esthetic zone can present significant challenges. Such placement can lead to esthetic concerns including an undesirable soft tissue appearance and suboptimal emergence profile, which may compromise both the visual appeal and functional integration of the implant.2,3 The discrepancy between the intended and actual position of the implant necessitates careful consideration of the potential impact on the final esthetic outcome and avoid possible technical complications.3
This case report illustrates the challenges and solutions associated with palatally placed implants in the esthetic zone, highlighting strategies to optimize both functional and esthetic results despite placement limitations.
Case Presentation
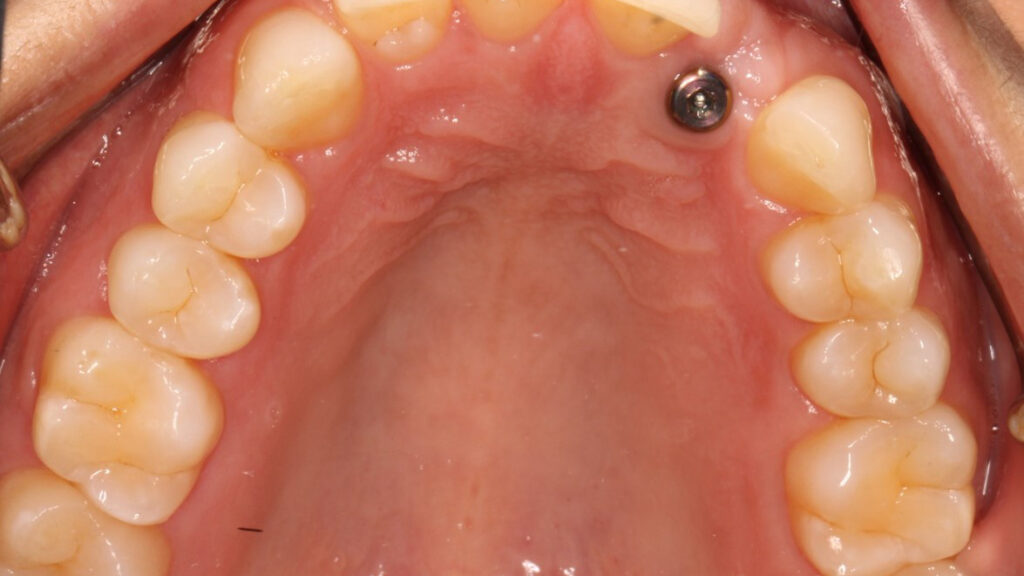
A 41-year-old healthy female patient presented to Graduate Prosthodontic Clinic at the University of Toronto with a concern regarding a maxillary anterior dental implant replacing tooth 22 with NobelReplace® Conical Connection narrow platform (NP) 3.5×10 mm (Nobel Biocare®, Zurich, Switzerland). Upon clinical and radiographic evaluation, it was noted that the osseointegrated implant had been positioned too palatal (Figure 1), which had the potential to adversely affect both the esthetic and functional outcomes of the restoration. The patient’s primary concern was the potential compromised esthetic appearance.
Fig. 1.

Initial Assessment
The implant placement had resulted in a notable discrepancy between the implant axis and the ideal tooth position, causing an unsatisfactory buccal contour and emergence profile. The soft tissues around the implant exhibited proper adaptation around the healing abutment (3.6×5 mm) with a thick gingival biotype. The patient expressed a desire for an improved cosmetic result that closely mimicked the natural appearance of the adjacent teeth. A primary impression was taken to do a diagnostic wax up of the 22.
Treatment Plan
To address these concerns, a comprehensive treatment plan was developed, which involved the following key steps:
- Soft Tissue Management: Initially, the soft tissues around the implant were assessed for their health and adaptability. Surgical intervention was performed to relieve and reposition the soft tissues around the implant. Using a surgical blade (#15), careful incisions were made to mobilize the soft tissues (4 areas buccal and palatal to the mesial and distal papilla), allowing for better adaptation of provisional crown and improved contour (Figure 2).
Fig. 2.

2.Emergence Profile Development: A chair-side screw-retained provisional crown was then fabricated using polymethyl methacrylate (PMMA) (Figures 3 & 4). This provisional restoration served a dual purpose: to provide immediate esthetic improvement and to function as a tool for shaping and developing the emergence profile of the final restoration. The provisional crown was designed to gradually enhance the contour and alignment of the soft tissues, thereby improving the overall esthetic outcome. The development of the emergence profile took over a period of 8 weeks with minimal modification to the provisional crown every 4 weeks.
Fig. 3.

Fig. 4.

3. Final Impression: After a period of 8 weeks allowing soft tissue adaptation and emergence profile development (Figures 5 & 6), a customized final impression was taken. The provisional crown was removed and screwed into an implant replica, then polyvinylsiloxane impression material used to capture the emergence profile contour from the provisional crown (Figures 7 & 8). After that an open tray impression coping was screwed to the replica and flowable composite material was added to modify the impression coping to capture the emergence profile (Figures 9a & 9b). The impression was taken with polyether material (Figure 10).
Fig. 5.

Fig. 6.

Fig. 7.

Fig. 8.

Fig. 9a.

Fig. 9b.

Fig. 10.

4.Restoration: The final prosthesis was a screw-retained porcelain-fused-to-metal (PFM) crown, meticulously crafted to replicate the natural morphology of the adjacent teeth and achieve a more balanced and harmonious esthetic result. The final PFM crown was successfully placed, and it significantly improved both the functional and esthetic outcomes. The restoration seamlessly blended with the adjacent natural dentition, and the emergence profile was optimized to enhance the overall appearance. Post-treatment follow-up (6 weeks) confirmed satisfactory integration of the soft tissues and patient satisfaction with the esthetic result (Figure 11).
Fig. 11

Discussion
The management of dental implants in the esthetic zone poses unique challenges, particularly when implants are not optimally positioned. The case presented here illustrates the implications of palatally placed implants and the strategies employed to address these challenges to achieve a satisfactory esthetic outcome.
Proper implant positioning is crucial for ensuring both functional integration and esthetic harmony. Implants placed suboptimal can result in several esthetic issues, such as an unfavorable buccal contour and compromised soft tissue appearance.3 The literature highlights that implants positioned too far palatal can lead to a lack of adequate buccal contour, which can negatively impact the final esthetic result.1,3 This misalignment often necessitates additional interventions to rectify the esthetic shortcomings.
In this case, the management of soft tissues around the implant was crucial. Surgical techniques to reposition and relieve the soft tissues are essential for creating a favorable environment for esthetic outcomes. Studies emphasize that proper soft tissue management is fundamental in achieving optimal esthetic results, particularly in cases where initial implant positioning is suboptimal.4 The use of surgical blades to mobilize soft tissues carefully allowed for better adaptation and contouring, addressing the esthetic concerns associated with palatally placed implants.
The development of the emergence profile is another critical aspect in achieving a successful esthetic result.4 A screw-retained provisional crown is a valuable tool for this purpose. As highlighted by Gomez-Meda and colleagues,4 provisional restorations play a significant role in shaping the soft tissues and emergence profile, facilitating a more predictable final outcome. By using a provisional crown to train the soft tissues and establish a more favorable emergence profile, we were able to significantly enhance the esthetic result of the final restoration.
The final prosthesis, a screw-retained porcelain-fused-to-metal (PFM) crown, was designed to replicate natural tooth morphology and integrate seamlessly with the surrounding dentition. PFM restorations have been used in clinical practice for many years and are considered the standard for implant-supported restorations.5 This type of construction offers both the necessary strength and satisfactory aesthetic results required for everyday use. Also, the use of PFM crown helps in ensuring minimal discomfort from the palatal profile of the abutment by using the minimal height needed for abutment. This approach ensured that the final restoration not only achieved a harmonious esthetic result but also met the functional requirements of the patient.
Conclusion
This case highlights the importance of addressing both the placement and surrounding soft tissue considerations in implant dentistry. Effective management of soft tissues and emergence profile development can mitigate the esthetic challenges posed by suboptimal implant placement. The use of provisional restorations and careful planning for the final prosthesis are essential in achieving successful outcomes in the esthetic zone.
References
- Testori T, Weinstein T, Scutellà F, Wang HL, Zucchelli G. Implant placement in the esthetic area: criteria for positioning single and multiple implants. Periodontology 2000. 2018;77(1):176-96.
- Den Hartog L, Huddleston Slater JJ, Vissink A, Meijer HJ, Raghoebar GM. Treatment outcome of immediate, early and conventional single‐tooth implants in the aesthetic zone: a systematic review to survival, bone level, soft‐tissue, aesthetics and patient satisfaction. Journal of clinical periodontology. 2008;35(12):1073-86.
- E. Jung R, Zembic A, Pjetursson BE, Zwahlen M, S. Thoma D. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow‐up of 5 years. Clinical oral implants research. 2012;23:2-21.
- Gomez‐Meda R, Esquivel J, Blatz MB. The esthetic biological contour concept for implant restoration emergence profile design. Journal of Esthetic and Restorative Dentistry. 2021;33(1):173-84.
- Hofstede TM, Ercoli C, Hagan ME. Alternative complete-arch cement-retained implant-supported fixed partial denture. The Journal of prosthetic dentistry. 1999;82(1):94-9.
About the author:

Mohammad Al-Tamimi: Resident, Graduate Prosthodontic Program, Faculty of Dentistry, University of Toronto, Toronto, Ont. Canada M5G 1G6.