


A case report and review
Abstract
With growing evidence in the literature to support soft tissue grafting around teeth and implants, reported patient concerns have been the esthetics following free gingival grafts and the management of post-operative pain. A novel approach to the recipient bed preparation using the “M-technique” for an apically positioned flap in combination with a free gingival graft was performed to increase the vascular supply and the surface area at the recipient site, which improves esthetics for the harvested graft. Palatal stents are a recommended option to manage haemostasis and patient post-operative pain, but the designs have scarcely been discussed. In this case, a vacuum formed palatal stent in addition to a digitally planned and 3D printed palatal stent were made to obtain patient feedback post-operatively. The purpose of this case report with narrative review is to outline novel approaches to improve esthetics, using the M-technique, following an apically positioned flap in combination with a free gingival graft at the recipient site and patient comfort with a palatal stent at the donor site.
There has been growing evidence in the literature to support soft tissue grafting around teeth and implants.1,2 This is to increase the thickness of the periodontal phenotype by increasing the keratinised tissue width (KTW) around teeth and keratinised mucosa (KM) around implants, when KTW/KM is <2mm.3 Following an apically positioned flap (APF), a free gingival graft (FGG) is usually an autogenous graft harvested from the palate to increase KTW/KM, increase vestibular depth (VD), increase tissue thickness, prevent further recession and improve plaque control as tissues are more resistant to physical, chemical, and thermal trauma.4 Furthermore, the FGG is a gingival augmentation procedure that helps to maintain teeth and implants in health by increasing the KTW/KM by ≥2 mm.5,6
Various options to achieve haemostasis and comfort following FGG harvesting from the palate have been discussed in the literature and can be summarized into 3 categories (Table 1).7 The most commonly reported techniques include the following options performed individually or together:
- Sutures with a collagen matrix or surgicel or platelet rich fibrin (PRF)
- Cyanoacrylate
- Palatal stent
- Periodontal dressing
Table 1: Options to achieve haemostasis following FGG harvesting from the palate.
| Protective Materials | Hemostatic Agents | Wound Healing Enhancers |
| Essix | Collagen matrix | Platelet-rich fibrin |
| Stent | Gelatin sponge | Autogenous fibrin glue |
| Retainers | Cyanoacrylate | Platelet-rich plasma |
| Periodontal dressing | Laser photobiomodulation | |
| Ozone therapy | ||
| Hyaluronic acid |
The palatal stent is one technique that can be planned in advance of the surgical procedure and it has been reported that patients require less pain medication post-operatively and have a higher willingness to do the same procedure again compared to other techniques.8
The purpose of this case report with narrative review is to outline novel approaches to:
- Improve esthetics, using the M-technique, following an APF in combination with a FGG at the recipient site and;
- Improve patient comfort with a palatal stent at the donor site.
Methods
Following informed consent, a periodontal examination was completed as defined by the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions with particular focus on the mucogingival conditions around teeth.9 The clinical parameters were completed by a periodontist that included the following:
- Probing depths (PD) were completed in millimetres using a UNC-15 probe.
- Gingival recession (GR) was completed in millimetres using a UNC-15 probe.
- Plaque/biofilm index (PI) was completed and scored as present or absent.
- Bleeding on probing (BOP) was completed and scored as present or absent.
- KTW around teeth was measured from the free gingival margin to the mucogingival junction in millimetres using a UNC-15 probe.
- Mobility and furcation involvements were also recorded.
Patient case selection
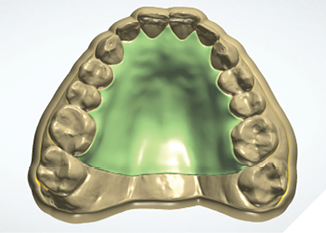
The patient was medically fit and well, with the chief complaint of brushing discomfort around the teeth #4.3 and #4.4 that had been getting progressively worse. The patient had previously had a FGG placed over 5 years ago in a different province and had no problems during or following the procedure. On presentation, a previous FGG can be visualised from teeth #3.3-4.1, the periodontal parameters were within normal limits, except there was minimal KTW (≤1mm) at the teeth #4.3 and #4.4. There were recession type (RT) defects present; RT 1 of 2mm at tooth #4.3 and RT1 of 1mm at tooth #4.4 (Fig. 1).10 A digital intra-oral scan was completed, and the palatal stent could then be designed from the STL file. The STL file enables a custom design that can utilize the interproximal undercuts to achieve retention whilst improving esthetics and comfort. Both the vacuum formed, and the 3D printed palatal stents were 0.5mm in thickness. The 3D printed palatal stent was designed by a qualified lab technician and designed according to where the patient would find the palatal stent most comfortable (Fig. 2).
Fig. 1A

Fig. 1B

Fig. 2
Surgical procedure: APF in combination with a FGG
The APF in combination with a FGG procedure was completed by a periodontist at the #4.3-4.4 implant site and profound anaesthesia was achieved using 1 carpule of 1:200,000 articaine.
A split thickness flap at this site was completed using the no.15C scalpel blade (Fig. 3). The vertical incisions are usually perpendicular to the bone (Figs. 4a and 4b); however, a variation was completed. The technique improved esthetics and healing as there was an increased blood supply at the site. The new suggested “M-technique” is a technique that angles the no.15C scalpel at 30-45 degrees towards the bone, in a convergent direction at the mesial and distal margins towards the recipient bed (see Figures 5a and 5b for the distal converging incision line in this case). The most coronal aspect of the recipient bed is also de-epithelialized. The inverse bevel towards the recipient site bed increases the vascular supply and increases the surface area at the recipient site, which improves esthetics for the harvested graft during the initial healing, especially during the plasmatic circulation and organic union phases.7 The root surface was debrided with hand instrumentation using universal scalers prior to the application of saline on a dampened gauze at the recipient site during the graft harvesting process.
Fig. 3

Fig. 4A

Fig. 4B
Fig. 5A

Fig. 5B

the bone viewed in the coronal plane.
A graft, of 1.5mm thickness, was harvested from the right palate.
Haemostasis at the site was achieved with a vacuum formed palatal stent and the patient also had a previously digitally designed 3D palatal stent as an alternative option once the palate was no longer anaesthetised for comparison of comfort and function (Figs 6 & 7).
Fig. 6
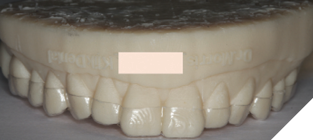
Fig. 7

The FGG was stabilised with 5-0 chromic gut sutures, that included 2x compressive sutures and 3x simple interrupted sutures (Fig. 8).
Fig. 8

Post-operative instructions were given that included analgesia advice and the temporary interruption in brushing at the surgical sites whilst CHX was prescribed twice daily around the grafted site.
Results
Following the procedure, at 6 weeks, the FGG blends in naturally with the existing KT and although treatment of recession was not the primary aim of the procedure, there was a decrease in recession at tooth #4.3 from 2mm to 1mm and at tooth #4.4 from 1mm to 0mm (Fig. 9 & 10).
Fig. 9

Fig. 10

The patient reported increased comfort with both palatal stents. The 3D printed palatal stent was more esthetic when the patient had a public engagement and more comfortable during eating and drinking. However, the vacuum formed stent required less manual dexterity to place in situ and to remove by the patient.
Discussion
Esthetics and patient comfort are 2 important aspects that accompany the success of gingival augmentation procedures. In a world where patient demands and expectations are ever rising in addition to an increase in digital workflows, this case report and narrative review has sought to highlight a few methods that can be integrated into practice.
Patient comfort can be achieved in multiple ways as outlined in Table 1; however, with patients that require multiple grafts or grafts requiring a larger amount of keratinised tissue from the donor site, the palatal stent can be a time efficient alternative to achieve haemostasis on the day of surgery. Other reported benefits include improved eating comfort and protection from chemical, physical, or thermal trauma for the patient during the initial healing period. Digital planning can help achieve retention by utilizing interproximal undercuts for retention, but a limitation would be that this requires higher patient manual dexterity and improved tongue movements to remove the palatal stent compared to the vacuum formed stent. The vacuum formed stent achieves retention, stability, and support by material extension over to the facial aspects of the teeth from the palate.
The “M technique” is a technique that is a modification of an established technique for the split thickness preparation of the recipient bed during the APF. The technique enhances vascularity to the donor tissue, as the blood supply from the recipient bed to the margins of the donor graft are improved. This increased vascularity to the graft improves blending of the donor graft to the new recipient site. In areas, where an increase in KTW is required, this technique can be recommended as an esthetic and less time-consuming alternative technique to a connective tissue graft (CTG). 
Oral Health welcomes this original article.
References
- Jepsen S, Caton JG, Albandar JM, Bissada NF, Bouchard P, Cortellini P, et al. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89 Suppl 1:S237-S48.
- Berglundh T, Armitage G, Araujo MG, Avila-Ortiz G, Blanco J, Camargo PM, et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018;89 Suppl 1:S313-S8.
- Avila-Ortiz G, Gonzalez-Martin O, Couso-Queiruga E, Wang HL. The peri-implant phenotype. J Periodontol. 2020;91(3):283-8.
- Camargo PM, Melnick PR, Kenney EB. The use of free gingival grafts for aesthetic purposes. Periodontol 2000. 2001;27:72-96.
- John V, Langer L, Rasperini G, Kim DM, Neiva R, Greenwell H, et al. Periodontal Soft Tissue Non-Root Coverage Procedures: Practical Applications From the AAP Regeneration Workshop. Clin Adv Periodontics. 2015;5(1):11-20.
- Herrera D, Berglundh T, Schwarz F, Chapple I, Jepsen S, Sculean A, et al. Prevention and treatment of peri-implant diseases-The EFP S3 level clinical practice guideline. J Clin Periodontol. 2023;50 Suppl 26:4-76.
- Tavelli L, Barootchi S, Stefanini M, Zucchelli G, Giannobile WV, Wang HL. Wound healing dynamics, morbidity, and complications of palatal soft-tissue harvesting. Periodontol 2000. 2023;92(1):90-119.
- Basma HS, Saleh MHA, Abou-Arraj RV, Imbrogno M, Ravida A, Wang HL, et al. Patient-reported outcomes of palatal donor site healing using four different wound dressing modalities following free epithelialized mucosal grafts: A four-arm randomized controlled clinical trial. J Periodontol. 2023;94(1):88-97.
- Cortellini P, Bissada NF. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J Periodontol. 2018;89 Suppl 1:S204-S13.
- Cairo F, Nieri M, Cincinelli S, Mervelt J, Pagliaro U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: an explorative and reliability study. J Clin Periodontol. 2011;38(7):661-6.
About the Authors

Dr. Matthew Morris is a certified periodontist in Canada and the UK. He is based in Halifax, Nova Scotia, where he works at Ocean Periodontal, Victoria Road Periodontal Associates, and teaches at Dalhousie University.

Manuel Fischer is a Master Dental Technician from Germany who has relocated to Canada and specializes in fixed denture restoration and 3D printing.

Dr. Michael Gillis received his DDS from Dalhousie University, and his MSc in Implant Dentistry from Goethe University in Frankfurt, Germany. He maintains a practice limited to implant dentistry in Halifax.

Dr. Zeeshan Sheikh was trained as a dental clinician, periodontist & a biomaterials scientist. He is an Assistant Professor at Dalhousie University and practices at Parklane Dental Specialists. He is a Clinical Scientist in Periodontics and a Fellow of The Royal College of Dentists of Canada, and a Diplomate of The American Board of Periodontology.

Dr. Haider Al-Waeli is a certified Periodontist, a Fellow of the Royal College of Dentists of Canada and works as an Assistant Professor at the Faculty of Dentistry Dalhousie University. He is also an Associate Periodontist in Park Lane Dental Perio Clinic in Halifax.