


Abstract
Tooth wear due to aging is a natural physiological process that generally does not negatively impact individuals unless exacerbated by parafunctional habits such as bruxism or congenital anomalies. This paper explores the implications of the loss of vertical dimension of occlusion (VDO) and its effects on the stomatognathic system. Symptoms of temporomandibular joint (TMJ) pain dysfunction syndrome are common in cases of severe attrition and are addressed through both conservative and permanent treatment approaches. Conservative treatments include behavior modification, NSAIDs, physiotherapy, botulinum toxin injections, and removable interocclusal splints. Permanent solutions focus on oral rehabilitation to restore the VDO and eliminate the underlying causes of the pathological condition.
This study presents two clinical cases demonstrating the successful increase of VDO and stabilization of occlusal relationships through multidisciplinary approaches involving the use of diagnostic appliances, provisional restorations, and final prosthetic treatments. The adaptability of the stomatognathic system to changes is emphasized, with a recommendation for cautious implementation of VDO adjustments to avoid negative outcomes. The importance of a thorough diagnostic evaluation and the role of various assessment methods for determining the appropriate VDO are discussed. The findings underscore the necessity of a customized treatment plan tailored to the individual patient’s needs, with the primary goal of achieving functional and symptom-free oral health.
Wearing of the teeth due to aging is a physiological process that generally does not negatively affect the average person. When attrition, i.e., the process of wearing down the teeth, occurs gradually—even in advanced cases where neuromuscular adaptation to the change is without adverse symptoms from the temporomandibular joint (TMJ), muscles, dental pulp, and periodontium—no treatment is required.
In many cases, especially when attrition is combined with parafunctional habits such as bruxism, discomfort and spontaneous pain may involve one or both TMJs and the muscles of mastication. The pain sensation, often perceived as an earache or headache, can spread, involving the muscles of the scalp and neck; these symptoms are typical of TMJ pain dysfunction syndrome.1,2,3 The treatment is usually conservative, involving behavior changes, NSAIDs, physiotherapy, botulinum toxin, and corticosteroid injections, and removable interocclusal splints.4,5,6,7
However, excessive wear caused by congenital anomalies (amelogenesis imperfecta, dentinogenesis imperfecta), parafunctional habits (bruxism), erosion (damage to teeth by chemical agents), or loss of teeth as a result of caries, periodontal disease, or iatrogenic dentistry can result in changes demonstrated by a decrease in the vertical dimension of occlusion (VDO), leading to subsequent pathology of the teeth and TMJ, followed by a disruption of function.1,8,9,10
The loss of VDO is also known as “collapse of the bite”.1 Amsterdam and Abrams8 introduced the term “posterior bite collapse.” Treatment options for these patients depend on the individual situation as well as the goals the patient and the dentist wish to achieve.
Solutions aimed at temporary relief of symptoms can be accomplished by the conservative treatment options listed above. For example, a patient with symptoms of TMJ pain dysfunction syndrome and a certain form of collapsed bite (or loss of VDO) may improve by wearing some type of interocclusal appliance. However, once the appliance is no longer used, the symptoms return. Botox injections in areas of painful muscle spasm provide some relief, but they must be repeated every 2-3 months.7
Permanent solutions for these situations should aim to determine and address the etiological factors leading to the collapsed bite. This involves restorative work for the remaining teeth—oral rehabilitation—with the goal of treatment being to restore form and thus permanently eliminate the cause of the pathological condition.
The diagnosis for patients with a collapsed bite should include a thorough evaluation of the remaining dentition—the number of teeth present, their periodontal status, assessment for caries lesions, and the type of restorative work they have had. An important diagnostic step is estimating the amount of VDO loss, followed by deciding to what degree and how to increase it without adversely affecting the TMJs and associated muscles.8,9,10,11
Different methods for assessing VDO exist, and none of them is 100% accurate. The rest position (RP) of the mandible can be used as a reference for assessing VDO.1,13 Another approach for determining VDO is considering the speaking space, which occurs with a reliable degree of consistency between the maxilla and the mandible—whether with teeth or edentulous—when producing certain sounds, i.e., the use of phonetics.13,14
According to Gupta and co-authors,15 Morrison in 1959 introduced the use of “S” sounds when pronouncing the words “sixty-six” and “Mississippi.” Regardless of the method being used, the linear difference between the two positions is demonstrated in the incisive point as a space between maxillary and mandibular front teeth—interocclusal distance—and can be measured extraorally between two predetermined points on the skin of the patient’s face.10
Turner and Missirian10 suggest using phonetic evaluation with the “S” sound, as well as assessing facial appearance based on the clinician’s experience. They offer a classification correlating the decrease in VDO with attrition and loss of teeth in the dentition, dividing patients into three categories. For each of these categories, they suggest different treatment options.
We will follow our introduction by presenting two clinical cases, defined by the Turner-Missirian classification. Both cases fall under category 1: loss of VDO due to attrition, with some molars and premolars missing, leading to unstable posterior contacts, a deep overbite, and lower incisors traumatizing the gingival margins of #11 and #21 lingually. Both patients experienced symptoms of TMJ pain dysfunction and had been using interocclusal appliances for years, with varying degrees of success. The goal for both cases was to increase the VDO and reposition the mandible mesially through restorative treatment and oral rehabilitation, thereby achieving a stable occlusal relationship. This resulted in the elimination of occlusal trauma and the symptoms of TMJ dysfunction.
Clinical case studies
Case 1
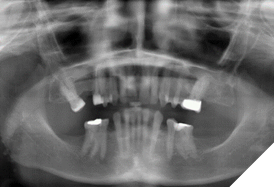
A 69-year-old Caucasian female in good general health was willing to permanently solve her dental problems, describing them as “headaches, discomfort, and earaches when chewing” and “gum problems with upper front teeth.” The maxilla/mandible relationship was prognathic, Class II, with a deep overbite (Fig. 1).
Fig. 1

Due to attrition, but mostly from the loss of maxillary and mandibular molars and premolars, she had a collapsed bite with loss of VDO and localized gingivitis in the area of #11 and #21 lingually, caused by chronic trauma from the incisal edges of the mandibular incisors.
The assessment of VDO was based on measuring the distance between two marks on the skin—under the nose and the chin. The distance was measured during maximum intercuspation and when the mandible was in rest position during the “S” sound by pronouncing “Mississippi” numerous times. There was a 7 mm difference between the two positions. However, measuring her interocclusal space at the incisive point to determine the amount of lost VDO would not be practical or informative because of her overbite.
When asked to move the mandible forward without interrupting contact at the incisive point, i.e., mesializing the position of the mandible, a space opened between the existing maxillary and mandibular molars and premolars—that’s where the lost VDO was to be determined and restored permanently.
The patient’s remaining teeth were moderately restored, with no active caries and adequate bone support (Fig. 2).
Fig. 2
The mandibular front teeth had small fractures of the incisal edges—a non-essential problem addressed later in the treatment. The gingival tissue was healthy, with the exception of the lingual aspect of teeth #11 and #21, as previously described.
The suggested treatment plan, accepted by the patient, included:
1. Fabricating and wearing for an extended period—a Gelb appliance—a mandibular repositioning, diagnostic appliance providing increased vertical dimension in the molar and premolar areas and relieving contact in the front teeth area (Fig. 3A).
Fig. 3A

2. After a new VDO was established, fabricating provisional restorations as a precursor to the permanent ones. This was an essential step for testing the patient’s acceptance of the newly attained treatment VDO.10,16
3. Once the provisionals were tested and felt comfortable, the treatment would be completed with bridges involving teeth #33, #35, #36, with pontic #34, and #43, #45, #46 with #44 pontic, permanently cemented.
4. Assessing the patient after completing the treatment with the fixed prosthodontics and, if needed, fabricating an anti-bruxism appliance.
The Gelb appliance (JBC clear polymer, JBC Company) was fabricated and inserted into the patient’s mouth. It was adjusted to provide stable bilateral contact in centric. This appliance, to be effective, should be worn at all times, with follow-up appointments for adjustments. The VDO for this appliance was determined by registering the occlusal relation (Kopy – vinyl polysiloxane bite registration – ultra-fast) when biting in the incisal area over a Lucia jig, separating the posterior teeth so that the pterygoid muscles are relaxed and the condyles seated in an optimal position.
The patient wore the Gelb appliance for about six months, with an interruption of two weeks. She removed it only when eating meals, and her headaches disappeared.
With the appliance in place, the patient was comfortable, and the posterior teeth contacted bilaterally. The space between the maxillary and mandibular incisors was initially 1-2 mm (Fig. 3B).
Fig. 3B

Every few weeks, she had appointments for adjustment of the Gelb appliance, during which the VDO was gradually decreased until a light contact occurred between the maxillary and mandibular incisors. The patient, who kept wearing the appliance, did not report any adverse effects. This gradual decrease in VDO from that with the Gelb appliance was an important step in avoiding major restorative treatment of the mandibular incisors and maintaining the comfort zone attained through the treatment.
Once the new VDO with the Gelb appliance in place was established, we developed what we called a “palatal jig” (Fig. 4).
Fig. 4
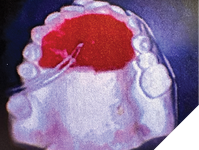
Made of fast-setting acrylic resin (Duralay Reliance Dental), it involved the palate and the lingual surface of teeth #14 to #24, finishing about 2-3 mm short of the incisal edges and occlusal surfaces. It was secured against accidental swallowing with dental floss incorporated in the resin. When inserted into the patient’s mouth together with the Gelb appliance, it provided, after proper adjustment, vertical stop for the mandibular closure at the already established VDO (Fig. 5A, 5B).
Fig. 5A

Fig. 5B

At the same time, the incisal edges of the maxillary teeth were not engaged as they were with the Lucia jig. This way, having the incisal edges and occlusal surfaces of all of the teeth exposed facilitated and made the registration of the bite more reliable (Fig. 6).
Fig. 6

After appropriate anesthesia—mandibular nerve block combined with local infiltration (2×1.8 mL 2% lidocaine, 1:100,000 epinephrine, and 2x 1.8mL Mepivacaine)—teeth #33, #35, #36, #43, #45, and #46 were prepared for crowns (Fig. 7), and provisional acrylic crowns made at the newly established VDO were cemented with temporary cement (Kerr, Temp-Bond NE, Unidose) (Fig. 8, 9).
Fig. 7

Fig. 8

Fig. 9

After two weeks, with no adverse effect reported, the provisional crowns were removed, the prepared teeth were assessed, and a final impression with a custom tray and vinyl polysiloxane impression material (putty and light body) was made. A bite registration with the palatal jig in place was also made (Kopy – vinyl polysiloxane bite registration ultra-fast) (Fig. 10).
Fig. 10

The provisional crowns were recemented with temporary cement, and occlusion was examined.
A week later, laboratory-made Zirconia bridges #33, #35, #36 with pontic #34 and #43, #45, #46 with #44 pontic were permanently cemented (Yttrium Zirconia – YZ – Argen Corporation, Shaw Lab, Kingston, Ontario).
The mandibular anteriors (#42, #41, #31, #32) were restored with composite material (Activa, Pulpdent) (Fig. 11).
Fig. 11

With bridge prostheses in place, the patient’s occlusion in centric had strong bilateral contacts between maxillary and mandibular molars, premolars, and cuspids, with light contact in the front.
During off-centric mandibular movement, anterior/cuspid guidance was evident, with disclusion in the molar/premolar areas (Fig. 12, 13).
Fig. 12

Fig. 13

Case 2
The second patient, at the time of treatment, was a 69-year-old female with clinical findings and symptoms as described above and no general health issues. The first step in the treatment was to establish a new VDO with a mesialized position of the mandible. As in the previous case, she wore Gelb appliances for periods of three months. The initial VDO with the appliance was gradually decreased during appointments for adjustments until attaining light contact between maxillary and mandibular front teeth, with strong bilateral occlusal contacts in the molar/premolar area.
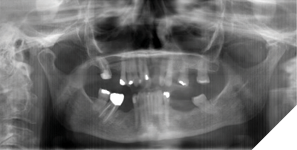
After establishing the restorative VDO, the patient was presented with different treatment options. She chose removable partial dentures; her choice was dictated by the fact that she was accustomed to having removable partial dentures before and had been satisfied with them. The existing teeth in her dentition were moderately restored, with a periodontal status appropriate for providing support for removable partial dentures (Fig. 14).
Fig. 14
Tooth #21 had been extracted due to chronic trauma of the gingival margin by the opposing #31 and #32 (Fig. 15).

The maxillary edentulism was treated with a tooth-borne partial upper denture (Fig. 16).
Fig. 16

As part of the preparation, #46—endodontically treated—was restored with a single Zirconia crown (Yttrium Zirconia – YZ – Argen Corporation, Shaw Lab, Kingston, Ontario), with the occlusal surface well under the level of the restorative VDO and a height of contour providing an undercut for a cast clasp (Fig. 17).
Fig. 17

A mandibular overdenture was fabricated and inserted, covering the occlusal surfaces of #47, #46, #44, #34, #37 (Fig. 18).
Fig. 18

With both maxillary and mandibular removable dentures inserted, the occlusal relation was at the previously established restorative VDO and mesially repositioned mandible (Fig. 19, 20).
Fig. 19

Fig. 20

During nighttime, when sleeping, the patient has been wearing an anti-bruxism appliance (Key Splint – Soft – Keystone Industries, Watersedge Lab – Ottawa, Ontario) to maintain the restorative VDO.
The treatment of this patient was concluded about five years ago, and she has been comfortable; the photographs illustrating the case were taken recently.
The adaptability of the stomatognathic system to changes is a fact that can be explored for the benefit of the patient, but with caution. Abrupt changes could result in negative outcomes. During the transition to the new, restorative VDO, a multidisciplinary approach is advisable. This includes implementing home exercises and massage therapy, recommending over-the-counter muscle relaxants and NSAIDs, and monitoring the patient’s response to the changes. In both cases, achieving this new, restorative VDO was, in our opinion, the most important part of the oral rehabilitation. The rest of the treatment and the type of prosthesis to be used were dictated by the availability of teeth in the dentition and the extent of the work the patients were willing to undergo. 
Oral Health welcomes this original article.
References
- Ramfjord, S., and M.M. Ash. 1983. Occlusion. Philadelphia: Saunders. pp. 25-28, 195, 239-267, 248, 359-379, 514, 519-524.
- Okeson, J.P. 2003. Management of Temporomandibular Disorders and Occlusion. St. Louis, Missouri: Mosby. pp. 191, 204, 233, 234, 227.
- 2nd Edition International Classification of Headache Disorders (ICHD-2). International Headache Society. 2013. “Classification and Diagnosis of Headache Disorders.” Accessed September 15, 2013. http://-classification.org/en/02_klassifikation/03_teil2/11.07.00_cranial.html.
- Orlando, B., D. Manfredini, G. Savetti, and M. Bosco. 2007. “Evaluation of the Effectiveness of Biobehavioral Therapy in the Treatment of Temporomandibular Disorders: A Literature Review.” Behavioral Medicine 33(3): 101-118.
- De Toledo, E.G., D.P. Silva, J.A. de Toledo, and I.D. Salgado. 2012. “The Interrelationship Between Dentistry and Physiotherapy in the Treatment of Temporomandibular Disorders.” Journal of Contemporary Dental Practice 13(5): 579-583.
- Marbach, J.J. 1996. “Temporomandibular Pain and Dysfunction Syndrome: History, Physical Examination, and Treatment.” Rheumatic Disease Clinics of North America 22(3): 477-479.
- Schwartz, M., and B. Freund. 2002. “Treatment of Temporomandibular Disorders with Botulinum Toxin.” The Clinical Journal of Pain 18(6): 198-203.
- Amsterdam, M., and L. Abrams. 1980. “Periodontal Prosthesis.” In Periodontal Therapy, edited by H.M. Goldman and D.W. Cohen, 6th ed., 1121-1154. St. Louis, Missouri: Mosby Co.
- Krishna, M.G., K.S. Rae, and K. Goyal. 2005. “Prosthodontic Management of Severely Worn Dentition, Including Review of Literature Related to Physiology and Pathology of Increased Vertical Dimension of Occlusion.” Journal of Indian Prosthodontic Society 5(2): 89-93.
- Turner, K., and D. Missirian. 1984. “Restoration of Extremely Worn Dentition.” Journal of Prosthetic Dentistry 52(4): 467-474.
- Nakamura, S., D. Donatelli, and E. Rosenberg. 2022. “Posterior Bite Collapse: Guidelines for Treatment Based on Form and Function.” International Journal of Periodontics and Restorative Dentistry 42(3): 351-359.
- Rivera-Morales, W.C., and N.D. Mohl. 1992. “Restoration of the Vertical Dimension of Occlusion in the Severely Worn Dentition.” Dental Clinics of North America 36: 651-664.
- Shayistha, M.U., V.N. Vivek, K. Harshakumar, and G.M. Noxy. 2021. “Concept of Rest Position of Mandible: An Overview.” International Journal of Applied Dental Sciences 7(2): 9-14.
- Pound, E. 1966. “The Mandibular Movements of Speech and Their Seven Related Values.” Journal of Prosthetic Dentistry 16(5): 835-843.
- Gupta, R., R.P. Luthra, and D. Gautam. 2016. “Phonetics in Complete Denture: A Review.” International Journal of Healthcare Sciences 4(1): 373-377.
- Carlsson, G.E., and T. Magnusson. 1999. Management of Temporomandibular Disorders in the General Dental Practice. Quintessence Publishing Co. pp. 128-129.
About the authors

Dr. Venelin Topouzov is a general dentist in private practice in Cornwall, Ontario.

Dr. Justin Lee is a general dentist in private practice in Cornwall, Ontario.