
Endodontic therapy involves treating infected pulps to save a tooth that otherwise may need to be removed. This treatment can become significantly more challenging when dealing with the adolescent dentition and underdeveloped teeth. The primary goal as clinicians is to restore function to the dentition. In the adult fully developed dentition, when extraction is the chosen path, one or more tooth replacement options may exist. That is not the case when dealing with the adolescent dentition. Fixed replacement options may not be available due to the fluctuating growth phases of the child. Vital Pulp Therapy is a treatment methodology that aims to preserve the health and vitality of the pulp tissue that has been compromised due to caries or dental trauma. This procedure allows the tooth to continue its developmental path and allows for natural exfoliation and eruption patterns to proceed.1,5
Clinicians are tasked with not only educating their patients and guardians on dentistry but also a cost and benefit analysis of the treatment options. This has become an increasing burden to dental practitioners. Patient’s expectations of dental treatment and guarantees of success are at an all-time high. The difficulty with treating the adolescent dentition is deciphering what the definition of success means to everyone. Premature loss of a tooth in the mixed dentition can result in catastrophic complications down the road.5 Malocclusion from altered eruption patterns, unesthetic tooth replacement options, periodontal issues are all possible when the natural eruption pattern is altered. Our job as clinicians is to educate our patients on the importance of investing in and maintaining oral health to align with the natural timeline of development.1,9
Pulp inflammation due to caries has been shown to be localized within the affected area of the tooth. Furthermore, it has been proven that normal healthy pulp tissue can exist at a distance from the carious irritant. If the carious and bacteria laden portion of the pulp can be successfully removed leaving behind healthy tissue, the innate regenerative process of the pulp-dentin complex will take over and continue to develop and strengthen the root structure of the tooth. This not only aids in tooth retention but also results in better overall dental function. Consistency in adhering to the protocol is the key to achieving a successful outcome. The following method resulted in success rates of 97.96%.2, 3, 4
Recommendations for Vital Pulp Therapy as adapted by protocol set forth by Bogen et al.7
- After profound anesthesia is obtained, place rubber dam over tooth to be treated.
- Perform complete caries excavation.
- Obtain hemostasis with placement of 5.25% NaOCl soaked cotton ball with pressure onto the exposed pulp tissue for 5 minutes.
- Rinse with water spray.
- If hemostasis is not obtained, repeat step 3.
- Place pulp cap material directly onto pulp tissue.
- Place final restoration immediately or within 5-10 days.
Treatment protocols of Vital Pulp Therapy
The tooth to be treated is anesthetized with the clinician’s anesthesia of choice. Profound anesthesia is verified with Endo Ice and routine cold testing. If cold is felt by the patient, supplemental anesthesia is given until a negative cold response is obtained. After anesthesia, rubber dam isolation is placed to ensure a strict aseptic technique. Complete caries removal is performed using high speed tungsten carbide fissure burs under sterile water cooling with the aid of magnification and light source. Once the pulp tissue is exposed, access cavity irrigation is performed by flushing the site with 5.25% hypochlorite solution. The coronal pulp tissue should be amputated to the level of the canal orifice to ensure all the affected tissue is removed. Hemostasis of the remaining pulpal tissue is achieved by placing a 5.25% soaked cotton pellet over the root canal orifices with firm pressure. The pellet is left in place for 5 minutes. After 5 minutes the pellet is removed, and the access is rinsed with sterile water and dried. If hemostasis is not obtained, the process is repeated. If hemostasis cannot be obtained, conversion to full root canal therapy is advised. To proceed with Vital Pulp therapy, the pulp capping material of choice is placed directly over the exposed pulp tissue. The most used and supported materials for Vital Pulp therapy include MTA (Dentsply Sirona), Biodentine (Septodont) or Bioceramics. A 2-3mm layer of the chosen material is packed onto the pulpal floor and gently compacted with a plugger or saline dampened cotton pellet. The access can then be immediately restored with the clinician’s material of choice while the tooth is still under rubber dam isolation to ensure sterility of the area. Final radiographs are taken for records.1, 6, 7
Recall is advised at two weeks. At this time, it is recommended to assess pulp vitality and any symptoms the patient may be experiencing. Post operative sensitivity is still normal at this stage as one would expect with routine restorative procedures. No new radiographs are necessary at this stage. Proper follow up from this point forward would be at 3-, 6- and 12-month intervals. At all these remaining visits, vitality testing should be performed in addition to periapical radiographs to assess root development of the tooth. Patient concerns and symptoms could also be routinely addressed. If at any point failure becomes evident due to spontaneous pain or periapical swelling, root canal therapy should be considered the next treatment option to maintain the tooth.4, 8
When performed correctly, Vital Pulp therapy is a conservative and viable option to restore the health and integrity of the natural dentition in the adolescent population. There is not always a restorative option for premature tooth loss in adolescents and we can provide a great service by offering well rounded treatment modalities to our younger population of patients.4, 5, 9
Clinical examples
Case 1: 8-year-old Caucasian female fractured the cusp of tooth 41 resulting in pulpal exposure of an underdeveloped permanent tooth. The pulp was vital and the decision to perform VPT to allow for continued root development was made. VPT was performed according to the above referenced protocol. The pulp capping material utilized in this case was bioceramic putty from Avalon Biomed. The one year follow up shows complete closure of the root apices. Pulp testing confirmed normal and healthy pulp status (Figs. 1A & 1B).
Fig. 1A
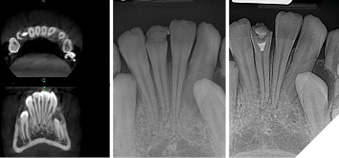
Fig. 1B
Case 2: (Courtesy of Dr. David Landwehr)
Carious exposure of underdeveloped tooth 35 with MTA (Dentsply) as pulp capping material. 4-year recall shows full root development of the tooth with apical closure. Pulp vitality was maintained (Figs. 2A, 2B, 2C).
Fig. 2A
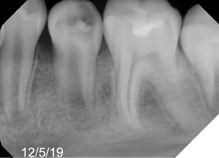
Fig. 2B
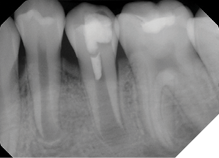
Fig. 2C
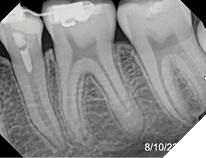
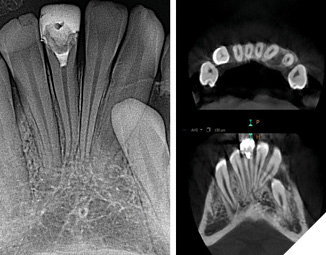
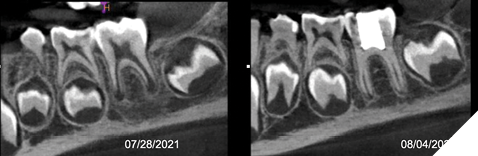
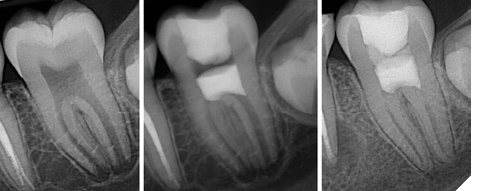
Case 3: 6-year-old Caucasian male presented with carious exposure of tooth 36 Underdevelopment of the root structure evident in PA and CBCT pre-op images. VPT was performed with bioceramic putty from Avalon Biomed. Continued recall shows progression and development of root structure while maintaining vitality of the tooth structure (Figs. 3A, 3B, 3C).
Fig. 3A
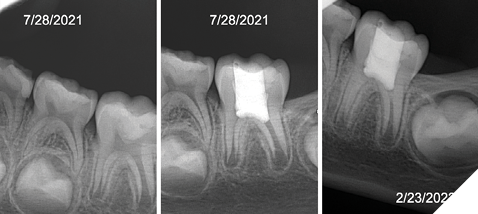
Fig. 3B
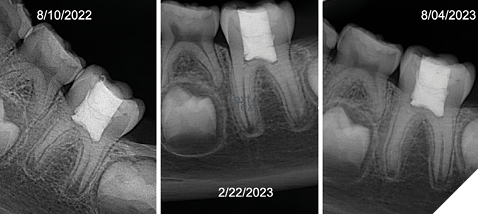
Fig. 3C
Case 4: 16-year-old Caucasian female presents with decay into pulp tissue of tooth 37. Roots are underdeveloped. VPT was performed using MTA (Dentsply). 2-year recall shows full root development and apex closure. Vitality of the tooth remains intact (Fig. 4).
 Fig. 4
Fig. 4
Oral Health welcomes this original article.
References
- AAE Position Statement on Vital Pulp Therapy. J Endod. 2021 Sep;47(9):1340-1344.
- Kakehasi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965 Sep;20:340-9.
- Ricucci D, Siqueira JF Jr, Li Y, Tay FR. Vital pulp therapy: histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J Dent. 2019 Jul;86:41-52.
- Xiaomiao Z, Zhang Y, Wang J, Wang Z, Wang X, Liu X, Cooper PR, Cheng X, He W. Effect of full pulpotomy using a calcium silicate-based bioactive ceramic in adult permanent teeth with symptoms of irreversible pulpitis. JADA. 2023 June;156(6).
- Murray PE. Review of guidance for the selection of regenerative endodontics, apexogenesis, apexification, pulpotomy, and other endodontic treatments for immature permanent teeth. Int Endod J. 2023 Mar;56 Suppl 2:188-199.
- Cao Y, Bogen G, Lim J, Shon WJ, Kang MK. Bioceramic Materials and the Changing Concepts in Vital Pulp Therapy. J Calif Dent Assoc. 2016 May;44(5):278-90. PMID: 27290822.
- Bogen G, Kim JS, Bakland LK. Direct pulp capping with mineral trioxide aggregate: an observational study. J Am Dent Assoc. 2008 Mar;139(3):305-15; quiz 305-15.
- Silva EJNL, Pinto KP, Belladonna FG, Ferreira CMA, Versiani MA, De-Deus G. Success rate of permanent teeth pulpotomy using bioactive materials: A systematic review and meta-analysis of randomized clinical trials. Int Endod J. 2023 Sep;56(9):1024-1041.
- Duncan HF. Present status and future directions-Vital pulp treatment and pulp preservation strategies. Int Endod J. 2022 May;55 Suppl 3(Suppl 3):497-511. doi: 10.1111/iej.13688. Epub 2022 Feb 3. PMID: 35080024; PMCID: PMC9306596.
About the author

Dr. Beth Ann Damas earned her D.D.S. alongside an M.S. in Oral Sciences at the University of Illinois at Chicago. She received an M.S. in Endodontics from the University of Detroit Mercy. Dr. Damas treats a range of patients in her practice and specializes in adolescent care. She is currently the Endodontic Consultant for Lurie Children’s Hospital in Chicago, Illinois. Her teaching focuses on modern endodontic approaches to provide patients with realistic expectations on how to preserve their natural dentition and maintain their oral health. Dr. Damas is a Diplomate of the American Board of Endodontics.