
The purpose of this article is to bring into focus, in a practical clinical setting, the many risk factors underlying dental caries and periodontal disease and to suggest means of mitigating these factors.
Traditionally, dentistry has relied on a surgical model to treat dental caries — that is to drill and fill. However, the medical model1 takes a different approach by identifying and mitigating the patient’s specific risk factors leading up to tooth decay and gum and periodontal disease before or immediately after invasive treatment is performed.
The other aspect of medical dentistry today is to show a bidirectional, casual or causal relationship between oral and systemic health. Mounting evidence supports a strong link between oral inflammation and systemic disease, such as diabetes, cardiovascular conditions, and auto immune disorders.2 This article, however, will discuss dental disease management for moderate to high-risk patients who, in spite of regular dental checkups and adequate home care, continue to have new or recurrent caries or periodontal disease.
Understanding and managing risk factors
Dental caries and the extended ecological plaque hypothesis3
Research has shown that dental caries is not purely a communicable disease.4 In an acidic pH environment, even commensal bacteria can become pathogenic. Managing the biofilm is therefore key to good oral and systemic health. In addition to the biofilm, saliva quantity and quality play a vital role in oral health.
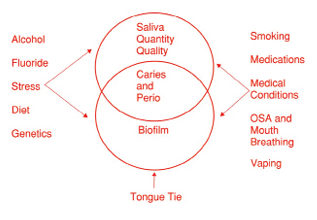
There are many factors that influence the saliva as well as the biofilm. They range from diet, nitric oxide, smoking, vaping, medications, stress, alcohol, fluoride, medical conditions, obstructive sleep apnea, mouth breathing, and tongue tie (Fig. 1).
Fig. 1
These risk factors can be identified through a comprehensive medical and dental history, interview, salivary diagnostics, and a clinical exam. (Table 1)
Table 1: Summary of risk factors for dental caries
| Name: D.O.B: | E-Mail: Phone: | |
| Risk Factor | Normal Range | Your Score |
| Biofilm (Carifree Meter) | < 1500 | |
| Salivary Factors: Consistency Resting pH Stimulated pH Buffer Capacity Flow Rate (Resting) Quantity Flow Rate (Stimulated) | Watery – Clear 6.8 – 7.8 6.8 – 7.8 10 – 12 < 60 sec >5 ml/5min 1 – 1.6 ml/min | |
| Dietary Factors: Frequency Contents: Sugar Anti-Oxidant Foods Pre-biotic Foods | 3 meals / 2 snacks Low High High | |
| Medical Conditions: Diabetes – HbA1C Blood Pressure BMI | <7 <120, <80 Men & Women 18.5 – 24.9 | |
| Plaque – Disclosed | Minimal | |
| Carries Experience | Low | |
| Sleep Mouth Breathing Snoring Bruxism Clenching Apnea Stop Bang Score | 0-2 | |
| Stress | 1-10 | |
| Smoking | None | |
| Alcohol Use | Moderate Women 1 / day Men 2 / day | |
| Genetics | ||
| Tongue-Tie | ||
| Pregnancy | ||
Once these risk factors are identified, they can be put into a caries risk assessment tool such as the ADA the AAPD or the CAMBRA form. My preference is the cariogram software program from Sweden because it is visual and more interactive.5
Key caries risk factors
Mouth breathing and salivary factors6,7
While the literature is not conclusive on this relationship one could see a possible high risk for caries for patients who have a reduced quantity and quality of saliva due to mouth breathing or medications, smoking, vaping, or alcohol. A deficiency of saliva decreases its buffer capacity leading to an increase in acidity which can lead to a proliferation of pathogenic bacteria, reduced ability to remineralize the enamel, and decreases antimicrobial activity. Sugar in alcohol and in some tobacco can be a substrate for bacteria to produce more acid. The free radicals produced by tobacco smoking or e-cigarettes can produce oxidative stress in the saliva, rendering it ineffective as a protective factor, compromising its immune function, leading to a dysbiosis in the biofilm.8
Diet as a risk factor for dental diseases
Not only can frequent sugars cause a low pH environment, but also there could be an imbalance between free radicals and antioxidants in our system, which also leads to oxidative stress in the saliva. Nitric oxide, which is derived from the breakdown of nitrates to nitrites in foods by commensal bacteria inhabiting the dorsum of the tongue, have antibacterial factors which reduce the pathogenic bacteria, thus helping to maintain a healthy biofilm. Nitric oxide is also produced endogenously in endothelial blood cells.9
Sugar also has a systemic effect on dental caries. A large body of research by Dr. Ralph Steinman showed that sugar can affect the endocrine system which affects the dentinal fluid transport through the tooth affecting tooth susceptibility.10,11
Systemic conditions
In terms of systemic conditions affecting caries and periodontal disease, diabetes has been shown to be bi-directional with dental diseases.12,13 High sugar levels find their way into the saliva and gingival tissues where bacteria can feed on them to produce more acid and destruction of dental tissues. Any systemic illness that limits the persons dexterity for home care, such as arthritis or cancer treatments that diminish the capacity of the salivary glands, can have an effect on caries susceptibility. Neurological disorders such as dementia or Alzheimer’s can definitely affect one’s oral hygiene care.
Chronic stress
Chronic stress causes the sympathetic nervous system to release cortisol, causing the body to produce more acid which affects the pH of the saliva. Stress also causes a decrease in salivary secretions leading to a decrease in clearance of pathogenic bacteria. As well as a decrease in other vital salivary functions under stress, unhealthy eating habits can increase with more frequent sugar snacks. In addition, stress can affect one’s self-care habits with less flossing and brushing, leading to a proliferation of pathogenic bacteria.14
Adequate fluoride decreases caries both systemically and topically
There is also research to show that a tongue tie can increase carries susceptibility by limiting the tongue’s ability to clear food debris from the oral cavity.15
One final area that can contribute to dental caries is that of genetics. While there is no conclusive test to show a genetic predisposition for dental caries or periodontal disease, there is speculation that genes may influence tooth development, the salivary defense mechanism, mineralization, taste, and the innate immune system.16 A new science is emerging called Epigenetics. This science investigates the influence of the environment, nutrition, and lifestyle on our genes. These influences could be positive or negative on our genes.17
Mitigating strategies
Dietary modifications
Reduce sugar frequency and amount, and increase antioxidant rich foods such as dark chocolate, berries, leafy greens, turmeric, and ginger to balance endogenous and exogenous free radicals, therefore, reducing oxidative stress in the body.
Biofilm control
Utilize salivary diagnostics, ATP testing (Cari free system), to identify the pathogenic load and then employ antibacterial treatments, such as Prevora, a chlorhexidine varnish or hypochlorous acid or molecular iodine rinses to reduce that load. In addition to reducing the pathogenic bacteria, probiotics should be used to increase the commensal bacteria.
Saliva optimization
A simple inexpensive test called Saliva-Check BUFFER made by GC America can give you seven markers for analysis. Address low salivary flow by using xylitol gum, hydration strategies, and remineralization therapies like MI paste and baking soda based oral care products. Foods to increase the pH of your saliva include cheese and nuts for snacks and increase arginine foods which are included in nuts and seeds, spinach, lentils, whole wheat, bread, seafood, and eggs.
Mouth breathing, and sleep apnea
Screen patients using the Stop Bang questionnaire and refer to a sleep specialist as needed.
Risk factors for periodontal disease18
The risk factors for periodontal disease, which is a chronic inflammatory disease, are very similar to those for dental caries. Leading the list would be smoking or other tobacco use, recreational drugs, a dysbiotic biofilm, calculus buildup, chronic emotional mental and physical stress, oxidative stress as a result of an imbalance of free radicals and antioxidants in the diet and in the body, obstructive sleep apnea, a compromised immune system, poor glucose control, hormonal imbalance during pregnancy, and menopause, and to a lesser extent genetics. Recently, there is a simple spit test available called PerioMonitor, which measures neutrophil activity in the oral cavity showing various degrees of inflammation.19 This tool is excellent in treatment planning for periodontal disease. If the patient has any medical conditions that could be bi-directional with their oral inflammation, you should consult their physician to discuss your findings.
How to start a disease management program
It is first necessary to declare to your patients that you have such a program. Then, you must appoint a staff member to be the preventative and disease management counsellor. Time must be booked in the schedule for the tests and consultations. You then must implement the treatment plan, and finally, follow up with the patient to retest and monitor the results of the treatment and the compliance of the patient. This is what I call “MEDICAL DENTISTRY” and should be standard of care.20 
Oral Health welcomes this original article.
References
- Jun Yu Yon, M. et al. Medical Model in Caries Management. Dent J. (Basel). 2019 April 1; 7 (2): 37
- D’Aiuto, F. et al. The Root of the Matter: Linking Oral Health to Chronic Diseases Prevention. International Journal of Cardiology Congenital Hearth Disease. March 2025; Vol. 19
- Nyvad, B. Takahashi, N. Integrated Hypothesis of Dental Caries and Periodontal Disease. Journal of Oral Microbiology 2020; Vol. 12
- Pitts, N.B., Twetman,S. Et al. Understanding Dental Caries as a Non-Communicable Disease. British Dental Journal; December 17, 2021; Vol. 231, No. 12
- Featherstone, John D.B., et al. A Comparison of Four Caries Risk Assessment Methods. Front Oral Health. 2021 April 28; 2:656558
- Dos Santos Letieri, A. Et al. A Critical Revue on the Association of Hypo-salivation and Dental Caries in Children and Adolescents. Archives of Oral Biology; Vol.144, December 2022
- Pedersen, A.M.L., Belstrom,D. The Role of Natural Salivary Defences in Maintaining a Healthy Oral Microbiota. Journal of Dentistry 80 (2019) S3-S12
- Sosa, V. Et al. Oxidative Stress in Saliva Induced by Tobacco Smoke: Impact on Periodontitis and Perspectives with Redox Pharmacology. Odontoestomatologia; Vol. 24 No. 39; June 2022
- Morou-Bermudez, E. et al. Pathways Linking Oral Bacteria, Nitric Oxide Metabolism and Health. J Dent Res, 2022, June: 101(6):623-631
- Roggenkamp, Clyde. Dental Caries Research Observations from Ralph Steinman and John Leonora: A Historical Perspective. LLUSD Articulator; Summer/Autumn 2016
- Rubinoff, Barry and Roggenkamp, Clyde. Systemic and Local Causes of Dental Caries and Host Resistance. Ontario Dentist, July/August 2021
- Latti, B. R. Et al Evaluation of Relationship Between Dental Caries, Diabetes Mellitus and Oral Microbiota in Diabetics. J Oral Maxillofac Pathol. 2018 May-Aug; 22(2): 282
- Casanova, L. Diabetes and Periodontal Disease: a Two-Way Street. British Dental Journal, 2014; 217: 433-437
- Jain, M. et al. Relationship of Perceived Stress and Dental Caries among Pre University Students in Bangalore City. Journal of Clinical and Diagnostic Research, 2014, Nov. 20: 8(11): zc131-zc134
- Gurkowski, S. Tongue Tie as a Missing Link to Caries. RDH; Sept. 12, 2022
- Hassell, Thomas M. Genetic Influences in Caries and Periodontal Diseases. Critical Rev Oral Biol Med; 6(4): 319-342, 1995
- Seo, Ji-Yun, et al. Epigenetics: General Characteristics and Implications for Oral Health. Restor Dent Endod. 2014 Nov 13; 40(1), 14-22
- Gasner, N, Schure, R. Periodontal Disease. National Institute of Health. 2023,April 10
- Elebyary, O., Glogauer, M. Monitoring Oral Inflammation: A Chairside Game-Changer. Oral Health Group. 2023-12-12
- CDA Board of Directors; Recommendations for a Risk Assessment. February, 2019
About the author

Dr. Barry Rubinoff graduated from U of T dentistry in 1964 and from the University of Illinois in paediatric dentistry in 1967. In addition to private practice, he had been on the dental faculty at U of T for over 20 years in the preventative department. He is currently on the faculty at George Brown College in the dental hygiene program. Over his dental career, he has made many presentations to dentists, hygienists, and the public in the field of prevention and disease management.