

The maxillary nerve (V2) block via the greater palatine canal is a technique for providing profound anesthesia of the hemi-maxilla. However, many dentists lack confidence with respect to administering the maxillary block, as they are relatively unfamiliar with the anatomy of the region as it relates to this method. It has the advantage of obviating – by an effective, single, more proximal block of the nerve trunk – the need for multiple buccal, labial, and palatal injections.
The two intraoral techniques for administering the maxillary block are the greater palatine foramen (GPF) injection and the buccal or posterior, infraorbital or posterior tuberosity approach. An extraoral technique has also been described.1,2 The popularity of the buccal, pterygopalatine fossa approach has waned because of the associated risk of hematoma. The palatal approach is fundamentally different, however, as it bypasses the pterygoid plexus of veins and the posterior superior alveolar artery – the two common sources of hematoma formation in the pterygoid fossa region. To date, there have been no documented cases of hematoma following a greater palatine canal approach.16
Two compelling reasons to consider using the greater palatine foramen injection include a high rate of success and a low incidence of complications. The greater palatine canal approach was first documented by Mendel in 1917 and revived by Silverman in 1923.3,4 Various refinements to the technique were subsequently added by other workers.1,2,5 A more detailed review of this technique and the pertinent literature is presented. Its practical value is illustrated by the description of a clinical case in which a local anesthesia was achieved, allowing an extraction to be performed in a patient who would otherwise have required a general anesthetic for definitive surgical intervention.
Indications
The V2 block is considered in cases involving anesthesia of an entire quadrant of maxillary teeth, associated bone and soft tissue to allow exodontia, restorative dentistry, or periodontal therapy. It is also useful when the extent of buccal odontogenic infection contraindicates infiltration anesthesia. In addition, this technique is used effectively in sinus and endodontic procedures, in cases of trauma to the maxilla, and in the diagnosis and treatment of chronic oral and maxillofacial pain syndromes such as a trigeminal neuralgia. It has also been used in the treatment of acute epistaxis.25
Contraindications
The only absolute contraindication to the V2 block is an infection in the region of the palatal foramen where there is a risk of spreading the infection into the pterygopalatine fossa. The presence of a systemic coagulopathy may be only a relative contraindication.
Anatomy
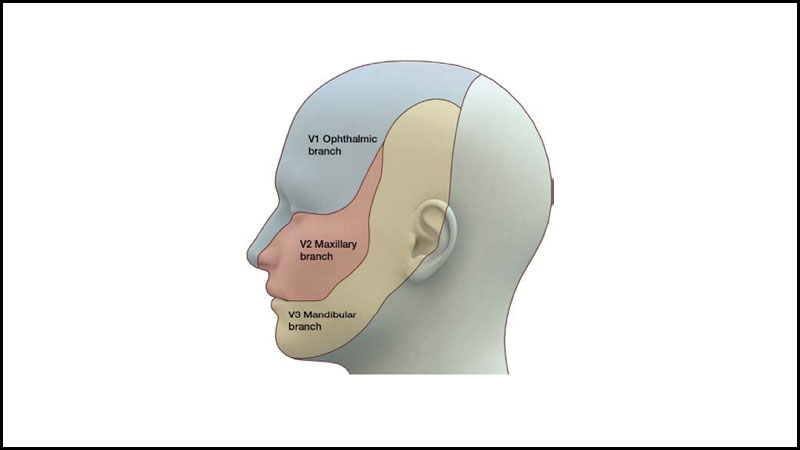
The success of any local anesthetic technique depends on a thorough and sound knowledge of the anatomy of the area to be injected and anesthetized. The second division of the trigeminal nerve arises from the gasserian ganglion in the middle cranial fossa and exits the skull via the foramen rotundum. The nerve then traverses the superior aspect of the pterygopalatine fossa, where it divides into three major branches (Fig. 1). This is the only site where the nerve trunk is devoid of bony protection, and it is here that the local anesthetic can be deposited to effect regional anesthesia. The three divisions and their terminal sensory branches(Fig. 2):
1. Pterygopalatine: nasal; nasopalatine; greater palatine; lesser palatine.
2. Infraorbital: posterior superior alveolar; middle superior alveolar (if present); anterior superior alveolar; maxillary sinus; superior labial; lateral nasal; inferior palpebral.
3. Zygomatic: nerve to the lacrimal gland (parasympathetic fibres – secretomotor from the sphenopalatine ganglion); sensory to the malar eminence (exits the zygomatic-orbital foramen).
Fig. 1

Fig. 2

Locating the greater palatine foramen (GPF) is of prime importance for a successful anesthesia of the maxillary nerve. However, there are anatomical constraints in locating the GPF as its covered by the palatal mucosa. Most of the studies have used reference points such as maxillary molar teeth, the distance of the GPF to midline maxillary suture (MMS) and the distance of GPF from posterior border of hard palate (PBHP)
Malamed and Trieger,6 studying 204 western skulls, found that almost 40 per cent of the greater palatal foramena were located between the middle of the maxillary second molar and the interproximal space between the second and third molars, while 51 per cent were situated between the latter site and the mid-portion of the third molar. A recent systematic review22 concluded that locating the GPF in relation to the maxillary molar teeth proved to be an expeditious way to locate the GPF which is commonly located opposite the third maxillary molar (Pooled prevalence of 64.9% with a confidence interval of 95%). In edentulous patients it was also recommended that the GPF could be accurately located using measured distances to landmarks such as midline maxillary suture, PBHP, and the Incisive foramen (IF) rather than the posterior and anterior nasal septum.
The distance between GPF and MMS was 15.4mm in Nigerian skulls and a mean of 14.7 mm in Indian skulls by Ajmani et al19 which was similar to the study reported by Saralaya and Nayakand.20 Chrcanovic and Custodio in their study have reported an average 14.56mm distance between GPF and MMS.
The mean distance of the GPF from the PBHP however showed considerable variation in different studies ranging from 1.9mm and 4.2mm. This difference in location could be on account of the sutural growth between the maxilla and the palatine bone.
The range of optimal needle insertion angle, formed by the long axis of the needle and the horizontal place of the hard palate, was 20 to 70 degrees. Wong and Sved5 recommended a need to maxillary occlusal plane angle of 60 degrees, and a lateral needle angulation of five to eight degrees from the sagittal plane. Malamed & Trieger6 reported that 75 per cent of the skulls had an optimal penetration angle between 37 and 57 degrees (Fig.4). Kim DW et al in their review found the MMS-IF-GPF angle22 to be 24.07 degrees which was consistent with the angle calculated by other studies.20,21 The MMS-IF-GPF angle is derived by the angle between MMS and the line drawn between IF to GPF. Knowledge of this angle is useful to determine the angle at which the needle could be passed to infiltrate the local anesthetic into the GPF.
Fig. 3
There was considerable anatomical variation in the direction of opening of the GPF in the recent metanalysis23 An Inferior-anterior-medial opening of the GPF relative to the sagittal plane was found 54.54% of the time compared to previously estimated 82.1%21 and the second most common direction of opening was in the anterior direction (30.11%) suggesting to bend the angle of needle closer to 30 degrees as opposed to 30-45 degrees to reduce the risk of puncturing soft tissues in the hard palate in case the GPF opens in the anterior direction.
Sexual dimorphism of the greater palatine foramen has been reported along with variation in age and differences populations.16-21 It imperative that clinicians have the anatomical knowledge necessary to minimize the risk of complications when performing procedures involving infiltration of the GPF.
Technique
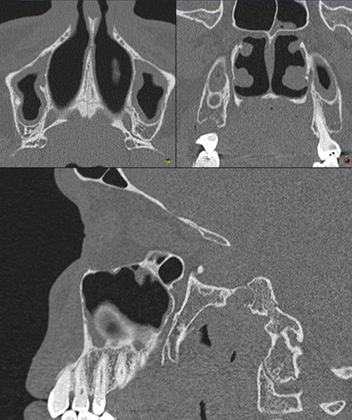
For the Greater Palatine Foramen Approach6,8,9-13 the patient is seated in a semi supine position in the dental chair, with his or her mouth opened widely. A mouth prop greatly facilitates access and visibility and stabilizes the mandible in the open position. However, the palatal mucosa makes it difficult to identify the precise location of the GPF, hence most studies have used reference points. Alternately, the hamular process can be palpated with a fingertip to orient the proper sagittal plane. The GPF will most often be located between the middle of the second molar and the middle of the third molar, 7.0 mm anterior to the end of the hard palate or 12 mm from the tip of the hamular process of the pterygoid. A CT scan or CBCT can be very useful in assisting with localization for foramen.
A cotton swab is then used to apply topical and pressure anesthesia (Fig. 4). A dental aspirating syringe and a 25-gauge long needle (32 mm in length) is gently introduced into the palatal mucosa at an angle of approximately 45 degrees to the long axis of the hard palate. Mercuri suggests a needle bent to a 30-degree angle 3.0 mm from the hub to facilitate entering the GPF. The needle is advanced superiorly and posteriorly until it has been inserted 32 mm. If resistance is encountered, the dentist should withdraw the needle 1.0 mm, change the angle slightly, and advance it again.10
Fig. 4

Aspiration is performed prior to the injection of local anesthetic. The two types of positive aspirations include blood, indicating intravascular location, and air, indicating that the needle has penetrated the nasopharynx. Following negative aspiration, anesthetic solution is deposited slowly with the aim of flooding the pterygopalatine fossa. The patient may experience a sensation of pressure behind the maxilla on the side of the injection at this point. Several authors typically injected 1.8 ml of local anesthetic solution,6,10 while others state that 4.4 ml of solution is required for good anesthesia.5,8
Onset of palatal anesthesia is almost immediate, with profound anesthesia developing within five to seven minutes. Occasionally, it is difficult to achieve profound anesthesia on the labial of the incisor teeth due to decussation of the contralateral V2 requiring supplemental anesthesia to the area. Success is indicated by numbness over the terminal branches of the maxillary nerve (lower eyelid, upper lip, cheek, and side of nose) (Fig. 5).
Fig. 5

Complications
The few complications reported for V2 blockade are the same irrespective of the approach. Sved et al8 examined the complication rate in 101 patients who were treated using maxillary nerve blockade via the GPF and reported incidences of diplopia (35.6 per cent), strabismus (11.8 per cent), failure of regional anesthesia (10.9 per cent), ptosis (9.9 per cent) positive blood aspirations (7.9 per cent) and neural trauma (one per cent).
The most common complication was diplopia of the ipsilateral eye, which can be expected due to the intimate proximity of the maxillary nerve and inferior orbital fissure. Deposition of solution at the appropriate plane (level of foramen rotundum) will almost inevitably lead to the diffusion of local anesthetic into the orbit via the inferior orbital fissure, which is reflected in the high incidence of diplopia.
Diplopia results from anesthesia of the orbital nerves (oculomotor, abducens and trochlear). The local anesthetic may block the proprioceptive fibres, resulting in strabismus (loss of ability to coordinate eyes in synchrony). Ptosis (drooping of the upper eyelid) may also accompany diplopia. Dickson and Coates13 and Corbett and Helmore9 reported diplopia in 6.25 per cent and 6.3 per cent of cases, respectively. The increased incidence reported by Sved et al8 may partly be explained by their use 4.4 ml of local anesthetic solution as compared to the 2.2 ml used by Corbett and Helmore. The resulting diplopia is transient in nature, and the patient requires reassurance of this fact. The patient’s eye should be covered with an eye patch to prevent any corneal abrasion due to a slowed blink reflex, and he or she should be accompanied home by a responsible adult, since monoscopic vision is without depth perception. There are no reported cases of permanent diplopia or other visual disturbances following this anesthetic technique. In fact, diplopia should not be feared as a consequence of this technique, but rather viewed as a positive sign of profound anesthesia.
The failure to anesthetize an entire quadrant may be cause by several factors. Operator experience plays a significant role, as it can be difficult to locate the GPF. However, a review of the relevant anatomy and practise with the technique will remedy the problem. The inability to negotiate the canal once the GPF has been located may be problematic. Several authors report constricted or tortuous canals in five per cent of patients, which may hinder negotiations of the entire length of the canal.6,8-10 Svet et al8 stated that penetration to within 15 mm of the “target” could still provide the required anesthesia. Every canal should be patent to some degree. The needle tip angulation may need to be adjusted if it impinges on the posterior wall of the canal. It is important not to force the needle at this point, as it may penetrate the paper-thin posterior aspect of the hard palate, depositing the local anesthetic solution in the nasopharynx. If this occurs, the patient will report feeling of gurgling or a bitter taste in the back of the throat.
The incidence of positive aspirations is low (8 per cent) when compared to conventional mandibular block techniques (22 per cent).8 This may be related to the anatomy of the neurovascular bundle within the GPF and the technique of the GPF injection. As the needle is advanced within the canal, it passes in a parallel direction to the bundle, allowing little angulation for penetration. Another possible explanation may be that the tough perineural fibrous sheath around the bundle deflects the cutting edge of the needle. If an intravascular injection should occur, the patient will complain of discomfort as the artery goes into spasm. As well, the terminal branches of the artery may constrict, causing blanching of the skin on the ipsilateral side. The patient should be advised that the symptoms are transient, with no postoperative sequelae. However, they can be avoided by always using the proper aspiration technique prior to injecting the local anesthetic.
Although neural trauma may be an obvious concern for the operator when administering the V2 block via the GPF, it has been recorded at the frequency of less than one per cent of the complication rate.8 The reason for this may be like those given for the lack of intravascular injections, namely the parallel sheath within the perineural sheath. If neural trauma does occur, the patient may experience an electric shock. The needle should then be backed out 1.0 mm and the anesthetic deposited. This may result in partial anesthesia, due to the failure to achieve the target depth, and supplemental injections may be required.
A theoretical complication is needle breakage within the GPF itself. This may be avoided if basic anesthetic rules and techniques are adhered to. The needle should never be forced, should not be bent at the hub, and should never be buried to the hub in the tissue.
Of the regional anesthesia failures reported (10.9 per cent), 5.9 per cent showed partial anesthesia and 4.9 per cent were complete failures.8 Supplemental injections may be required to complete the quadrant anesthesia for the incisors, due to cross innervation from the contralateral side. The claimed success rate of 89 per cent was consistent with Dickson and Coates (80 per cent),13 Corbett and Helmore (78 per cent),9 and Malamed and Trieger (90 per cent).6 By way of comparison, success rates for the inferior alveolar nerve block are 79 per cent for the Akinosi, 92 – 100 per cent from the Gow-Gates, and 65 – 85 per cent by the standard technique.8
Conclusion
The maxillary block via the GPF is an extremely useful technique for the dental practitioner and specialist alike. With sound knowledge of the regional anatomy and a thorough understanding of GPF length and pathway types is needed to properly administer anaesthesia prior to maxillofacial procedures. Aside from direct digital palpation or use of a cotton applicator, a CT or CBCT may be useful in assisting with the localization of the foramen. 
Oral Health welcomes this original article.
References:
- Stebbins, H.M and Burch, R.J. Intraoral and extraoral injections / Oral Surg 19: 21-29, 1961.
- Poore, T.E. and Carney, F.M.T. Maxillary nerve block. A useful technique / Oral Surg 31: 749-755. 1973.
- Mendel, N. and Puterbaugh, P.G. Conduction, infiltration and general anesthesia in dentistry, 4th ed. Dental Items of Interest Publishing Co., New York, 1938. P. 140.
- Silverman, S.I. Advances in block anesthesia including original technique of injecting the superior maxillary nerve. Dent Cosmos 15:474-477, 1923.
- Wong, J. D. and Sved, A.M. Maxillary nerve block anesthesia via greater palatine canal: A modified technique and case reports Aust Dent J 36:15-21, 1991.
- Malamed, S.F. and Trieger, N. Intraoral maxillary nerve block: An anatomical and clinical Study Anesth Progress 30:44-48, 1983.
- Jorgensen, N.B. and Hayden, Jr. J. Sedation, local and general anesthesia in dentistry. 3rd ed. Lea and Febiger, Philadelphia 1980, pp. 58-62
- Sved, A.M., Wong, J.D., Donker, P. et al. Complications associated with maxillary nerve block via greater palatine canal. Aust Dent J 37:340-345, 1992.
- Corbett, T.R. and Helmore, F.E. Block anesthesia of the maxillary nerve via the greater palatine foramen. Proc 11th Aust Dent Congress, Perth, WA, pp. 137-145, 1948.
- Mercuri, L.G. Intraoral second division nerve block. Oral Surg Oral Med Oral Pathol 47:109-113, 1979.
- Canter, S.R., Slavkin, H.C. and Canter, M.R. Anatomical study of pterygopalatine fossa and canal J Oral Surg 22:26-41, 1964.
- Trieger, N. New approaches to local anesthesia In: Pain Control 2nd ed. Mosby, Toronto, 1994, pp. 49-55.
- Dickson, G.C. and Coates, R.H. Regional anesthesia of the maxillary nerve by the palatal method Br Dent J 79:242-244, 1945.
- Malamed, S. F. Handbook of Local Anesthesia 2nd ed. C.V. Mosby Co., Toronto, 1986, pp. 146-182.
- Aoun, G. et al. Maxillary nerve block via the greater palatine canal: An old technique revisited. J Int Soc Prev Community Dent 2015.5(5) 359-364.
- Nish IA, Pynn BR, Holmes HI, Young ER. Maxillary nerve block: a case report and review of the intraoral technique. J Can Dent Assoc. 1995:61(4):305-10.
- Mahesh, A and Rajesh, S. A study of the greater palatine foramen and its importance in the application of maxillary nerve block in south Indian population. In J Ant Res 2015.9 (1.1)7857-60
- Westmoreland EE, Blanton PL. An analysis of the variations in position of the greater palatine foramen in the adult human skull. Anat Rec. 1982;204:383–8.
- Ajmani ML. Anatomical variation in position of the greater palatine foramen in the adult human skull. J Anat. 1994;184:635–7
- Saralaya V, Nayak SR. The relative position of the greater palatine foramen in dry Indian skulls. Singapore Med J. 2007;48:1143–6.
- Chrcanovic BR, Custódio AL. Anatomical variation in the position of the greater palatine foramen. J Oral Sci. 2010;52:109–13.
- Tomaszewska IM, Frączek P, Gomulska M, Pliczko M, Sliwińska A, Sałapa K, Chrzan R, Kowalski P, Nowakowski M, Walocha JA. Sex determination based on the analysis of a contemporary Polish population’s palatine bones: a computed tomography study of 1,200 patients. Folia Morphol (Warsz) 2014;73:462–468. doi: 10.5603/fm.2014.0069.
- Kim DW, Tempski J, Surma J, Ratusznik J, Raputa W, Świerczek I, Pękala JR, Tomaszewska IM. Anatomy of the greater palatine foramen and canal and their clinical significance in relation to the greater palatine artery: a systematic review and meta-analysis. Surg Radiol Anat. 2023 Feb;45(2):101-119. doi: 10.1007/s00276-022-03061-z. Epub 2023 Jan 14. PMID: 36640185; PMCID: PMC9899171.
- Tomaszewska IM, Kmiotek EK, Pena IZ, Sredniawa M, Czyzowska K, Chrzan R, et al. Computed tomography morphometric analysis of the greater palatine canal: A study of 1,500 head CT scans and a systematic review of literature. Anat Sci Int. 2014 Dec 3; doi: 10.1007/s12565-014-0263-9.
- Harris R. Greater palatine block in the treatment of acute epistaxis. Ann R Coll Surg Engl. 2015 Mar;97(2):161-2
About the Authors:

Dr. Bharathidasan, is a staff anesthesiologist, Assistant Professor in the Department of Anesthesia at the Thunder Bay Regional Health Sciences Centre. He sub-specializes in Neuro anesthesia, Perioperative anesthesia and has special interest in Point of Care Ultrasound.

Dr. Nish, is a graduate of The University of Toronto in both Dentistry and Oral & Maxillofacial, and subsequently completed a Fellowship in Plastic & Reconstructive Surgery in Basel, Switzerland. Dr. Nish was a Staff OMFS at Sick Kids Hospital for two decades, with a particular interest in reconstructive surgery as applied to patients with Cleft Lip & Palate and Craniofacial deformities.

Dr. Pynn, is Oral Health’s editorial board member for oral and maxillofacial surgery. He is an Assistant Professor, North Ontario School of Medicine, Lakehead University, and Chief of Dentistry, Thunder Bay Regional Health Sciences Center.