
Full-arch, implant-supported fixed dental prostheses (IS-FDP) are a well-established restorative option for the replacement of missing and terminal dentition. There are multiple suprastructure configurations and materials from which clinicians can consider, including acrylic resin to metal, metal-ceramic, monolithic zirconia, and porcelain fused to zirconia prostheses. Frameworks are composed of either titanium alloy, chromium cobalt, or monolithic zirconia. With CAD-CAM technology and the evolution of milling and printing materials, additional options are becoming available including composite resin (veneering material) and polyetherether ketone (PEEK) (framework material). All options offer unique advantages and disadvantages, and general considerations in treatment planning include the status of the opposing dentition, available restorative space, anatomical considerations, cantilever length, esthetic expectations, and a history of parafunction or other biomechanical risk factors.1
As defined by the Glossary of Prosthodontic Terms,2 a hybrid prosthesis is a nonspecific term that is frequently used to describe a dental prosthesis composed of different materials. It may refer to fixed dental prostheses but may also refer to removable or maxillofacial prostheses. In the context of IS-FDP, the term hybrid prosthesis is typically used to refer to acrylic resin-to metal designs whereby a metal framework is veneered with conventional polymethyl methacrylate resin set with denture teeth. The primary advantage of hybrid prostheses is the ease of repairability and, given their long history and documented reliability, are still a good option for many patients today.
Complications of IS-FDP are classified as either biologic or prosthetic.3 Biologic complications include peri-implant diseases (peri-implant mucositis and peri-implantitis) and, ultimately, implant failure. Prosthetic complications can be defined as minor or major, with minor complications including wearing of prosthetic material, decementation (loss of retention), loss of screw access filling, chipping of prosthetic material, loosening of prosthetic or abutment screw. Major prosthetic complications include fracture of the prosthetic material, the prosthetic or abutment screw, the framework, abutment, or implant.4 Wearing and chipping of the veneering material are the most frequently reported minor and major complications in IS-FDP and, as such, clinicians must consider strategies for repair in long-term management of patients treated with these prostheses.
Simple localized fractures of acrylic veneering material and/or denture teeth can be readily repaired using conventional denture techniques utilizing either direct/chairside or laboratory-processed approaches. At a certain point of veering wearing or fracture, replacement of the entire veneering material should be considered. In a study of 205 IS-FDP, this typically occurred after 7.8 years of service5 and is considered an expected medium-term maintenance procedure.1
Multiple terms are currently used to describe the process of stripping and replacing the veneering material of an IS-FDP on an existing framework. These include:
Retread: “Put a new tread on (a worn tire)” – most used term in literature related to IS-FDP
Resurface: “Put a new coating on or reform (a surface such as a road, a floor, or ice).”
Refurbish: “Renovate and redecorate (something, especially a building)”
Definitions courtesy of the Oxford Dictionary
Surprisingly, despite popularity and history of use, none of these terms are currently included in the Glossary of Prosthodontic Terms, 10th edition.2 The lack of consensus on a term to describe the same procedure leads to difficulty for clinicians and researchers alike to locate useful information related to this subject. The best available definition of this procedure in the literature is provided by Balshi et al. 2016:

“A retread is the removal of worn veneering material on an implant-supported framework followed by replacement with new veneering material at a desired VDO on the same implant-supported framework”
Indications for retread are patient-specific and include:
1. Degree of tooth wear
- >1/3 coronal height of incisors
- Significant posterior occlusal wearing
2. Apparent loss of VDO
3. History of repeated fractures/repairs of veneering material
Other clinical considerations for retread include:
- Age of the prosthesis and framework material: Significant deformation can occur after loading which may be clinically significant1
- Passive framework with acceptable design to support veneering material: Must recognize any framework misfits, inappropriate cantilever lengths, and areas of unsupported veneering due to high risk of continued prosthetic complications
Strategies for prevention of prosthetic complications:1
1. Material selection:
a. Veneering material
i. Resin: Minimum 10-15mm restorative space required for resin hybrid IS-FDP
ii. Metal-ceramic and monolithic zirconia restorations offer higher strength and wear resistance
b. Framework material: Chromium cobalt and grade 5 titanium alloys exhibit better flexural strength than commercially pure titanium (grade 1-5)
c. Framework design: Direct implant connection preferred to maximize preload and reduce overloading of the prosthetic screw
2. Adequate framework thickness: Minimum 4x4mm recommended for Ti6Al4V titanium alloy
3. Consider placing gold or porcelain inlays/onlays on occlusal surfaces to maintain stable occlusal contact and reduce rate of wearing
4. Management of biomechanical risk factors6
a. Underlying parafunctional habits (clenching, bruxism): Occlusal devices have been generally shown to be effective to reduce prosthetic complications
b. Status of the opposing dentition (dentate, partial edentulous, or complete edentulous with fixed or removable prostheses): Opposing IS-FDP represents the highest risk of prosthetic complications
5. Regular maintenance appointments to check condition of prosthesis, occlusion, and continued passivity.7 A detailed position statement on recommendations for management of full-arch implant restorations is available through the American College of Prosthodontics website.8
Treatment options for wearing or fracture of veneering material on hybrid IS-FDP:
1. No treatment
2. Localized/Simple repair: Direct chairside repair or lab-processed repair
3. Retread of existing framework
a. In the same material
b. With new material
4. Fabrication of new prosthesis
Retread: General approaches5
A. With interim prosthesis/acceptable reference
- Alginate impressions/stone cast of opposing arch
- Remove IS-FDP, check condition of multiunit abutments (if applicable)
- Insert interim prosthesis with original VDO, take occlusal relation with opposing arch
- Use interim prosthesis on master cast to mount using interocclusal record. Then, replace with definitive prosthesis – this will show the degree of wearing and loss of VDO
- Patient wears interim prosthesis home. Definitive prosthesis is stripped of veneering material and new tooth set-up completed for wax try-in.
B. Without interim prosthesis/acceptable reference: Two options
- Traditional denture construction methodology (including wax rims)
- Mock-up on existing definitive prosthesis: Build incisal edges with shims/composite to establish recovered VDO, set incisal position, and take CR record
New CAD-CAM technologies and the rise of digital dentures may allow for digital workflows for providing a retread of existing IS-FDP frameworks, although no existing literature exists to describe this process.
Case Examples
1. Simple Repair
85-year-old ASA II female patient presents seeking repair of fractured teeth #11, 13 of hybrid maxillary IS-FDP (Fig. 1).
Fig. 1

Clinical findings:
- Minimal tooth wearing (<1/3 incisal height)
- Localized fracture
- Acceptable VDO
- Age of prostheses: 13 years
- Last refurbishing 2021 (2.5 years)
- Opposing dentition: IS-FDP
- Patient wears nightguard daily
- History of bruxism
– Treatment provided: Same-day lab-processed repair (Fig. 2)
Fig. 2

2. Retread: Utilizing existing reference
76y/o male ASA II patient presents seeking repair of fractured teeth #12, 11, 21 on maxillary hybrid IS-FDP
Clinical examination:
- Extraoral examination: Apparent loss of VDO (downturned lips, angular cheilitis, closest speaking space)
- Intraoral examination: Heavily worn teeth with framework visible, history of repeated fractures, no nightguard usage
- Opposing dentition: Mandibular IS-FDP
– Prostheses age: 25 years (framework fabricated in 1999)
- Last retread: 7 years (2017)
- Repaired 4 times since 2020
- Existing master casts with implant analogs and models of prostheses after last retread
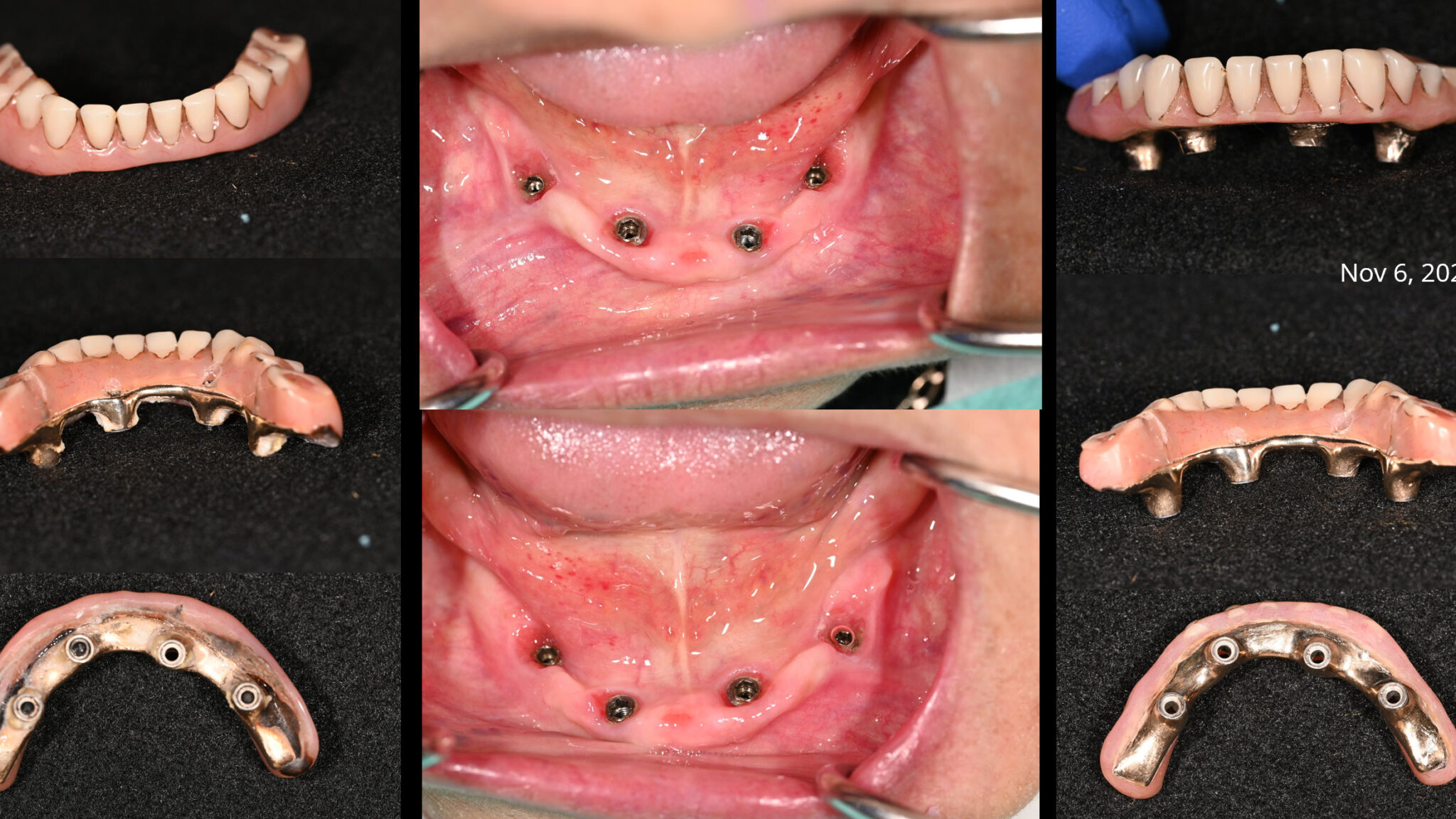
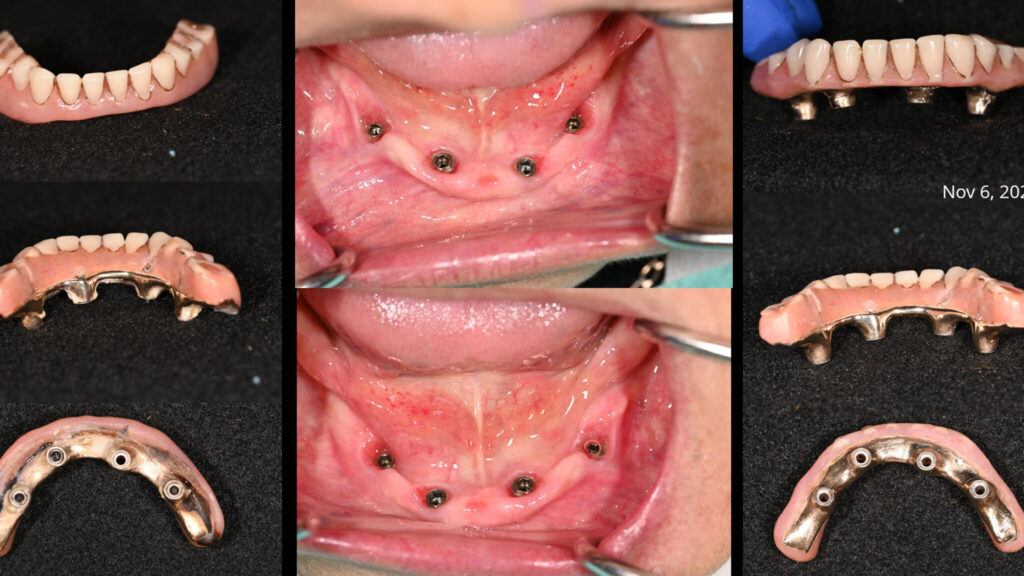
– Treatment provided: retread of maxillary and mandibular IS-FDP
Sequence of appointments (Figs. 3-5):
1. Initial records
- Photos
- Maxillary (Mx) and mandibular (Md) alginate impressions with prostheses in place
- Facebow, interocclusal record
- **check abutment screw tightness and condition
- **confirm framework seating/passivity intraorally
- Verify existing master casts using framework
- Place healing abutment/MUA caps (or use previous provisional, if available)
2. Tooth set-up try-in
- Hand-tighten abutment screws
- Radiographs to confirm seating
- Assess VDO, phonetics, esthetics, occlusion, cleansability, etc.
- Patient consent for processing
- Place healing abutments/MUA caps (or use previous provisional, if available)
3. Insertion
- Check for any acrylic flash, evaluate prostheses on articulator
- Insert prostheses and-tighten prosthetic screws
- Last opportunity to verify framework passivity
- Radiograph to confirm seating
- Torque following manufacturers recommendations
- Check occlusion, hygiene access, etc.
- Teflon + interim restoration in screw access channel (or composite resin)
4. Post-insertion check
- Check screw torque for any loss of preload (Kelly & Salinas 2017) and place final screw-access restorations as needed
- Set maintenance/recall schedule
3. Retread: Without existing reference
79-year-old female ASA II patient presents with chief concern of suboptimal esthetics and desire to replace existing maxillary denture and Md IS-FDP. Pt reports history of accidental cheek/gum biting which causes discomfort, and concern that thinning of denture will increase risk of fracture.
Fig. 3
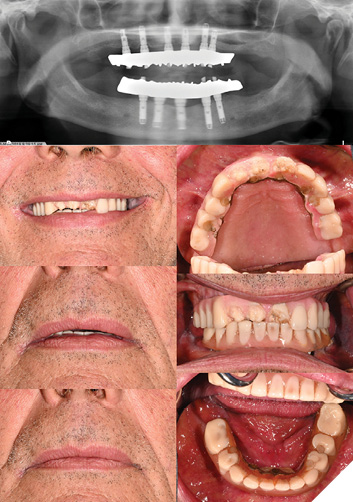
Fig. 4
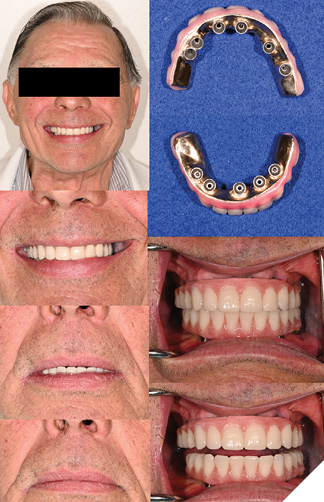
Fig. 5A

Fig. 5B
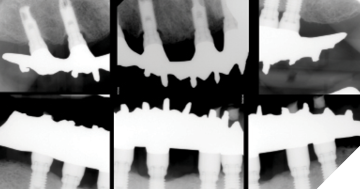
Clinical findings:
- Extraoral exam: Apparent loss of VDO, no incisal display at rest or in maximum smile, low lip line, inadequate soft tissue support
- TMJ asymptomatic, click on opening (disc displacement with reduction)
- Patient is dissatisfied with esthetics of smile
– Intraoral exam: Severe residual ridge resorption (RRR) in maxilla with a mobile, flabby ridge
- CUD: poor stability, support, moderate retention
- Heavily worn teeth
- Md IS-FDP has ridge-lap design, pt reports significant food impaction
- General BOP-Dx peri-implant mucositis
Age of prostheses:
- Md IS-FDP 2006 (original veneering material present)
- Mx CD 2019 (origin: Philippines)
Treatment provided: new Mx complete denture, retread of Md hybrid IS-FDP and periodontal therapy to manage peri-implant mucositis
– As there is no available reference prosthesis for the mandibular arch and a new complete denture is planned, the sequence of steps for the Md IS-FDP retread will follow conventional steps in denture fabrication.
Treatment sequence (Figs. 7-12):
- Initial records and periodontal therapy to manage peri-implant mucositis
- Final impression of Mx + Md to capture new RRR
- Occlusion rim appointment
- Tooth set-up try-in of Md complete denture and Md IS-FDP
- Insertion
- Post-insertion check
Fig. 6

Fig. 7
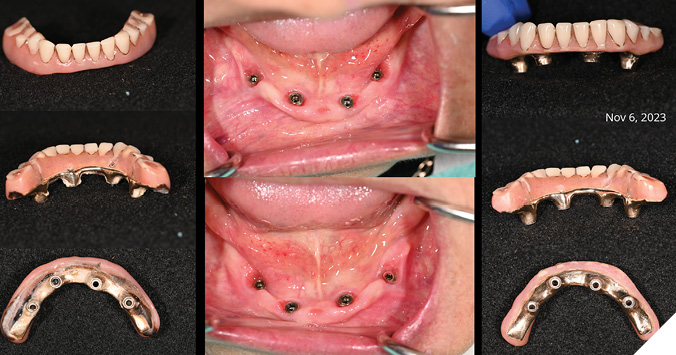
Fig. 8
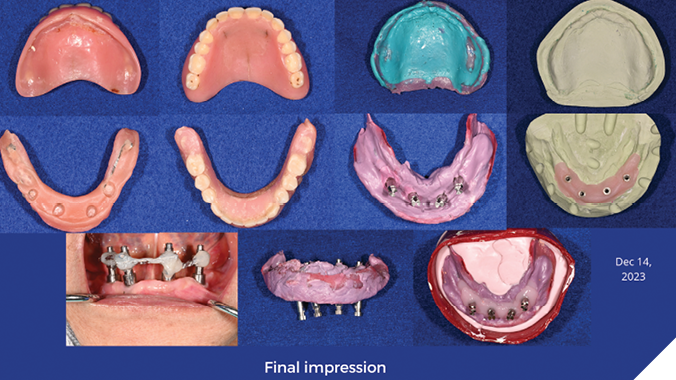
Fig. 9
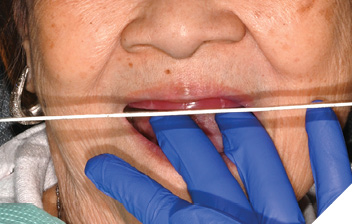
Fig. 10

Fig. 11
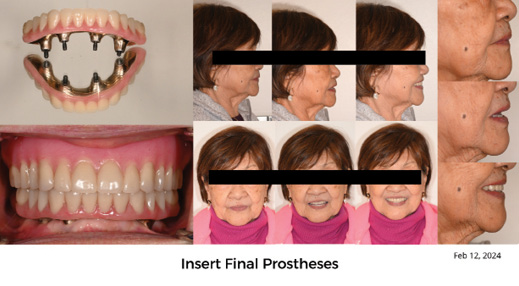
Fig. 12

Retread case comparison
| Case 1 | Case 2 | |
| Case Type | Dual Mx/Md IS-FDP | Mx CD, Md IS-FDP |
| # appointments to delivery | 3 1. Dx casts, facebow, interocclusal record 2. Wax try-In 3. Insert | 5 1. Dx casts, facebow, interocclusal record 2. Final Impression (optional) 3. Occlusion rims 4. Wax try-in 5. Insert |
| Interim prosthesis | None | Mx + MD CD |
| Total Tx time | 1 week | ~2 months |
| Date of prosthesis | 2017 (Framework 2003) | 2006 |
| Implant Type | Bränemark MKII (1998) | Bränemark MKIII TiUnite (2006) |
Conclusions
Regardless of material type, prosthetic and technical complications continue to be highly prevalent in patients treated with IS-FDP and prevention and management of these complications is an important consideration in treatment planning. Wearing and fracture of veneering material is the most common prosthetic complication of IS-FDP. Patients should be educated on preventive, maintenance, and repair strategies prior to prosthesis fabrication. The use of a nightguard has been shown to reduce the rate of chipping and fracture of veneering material and is recommended in most situations. Hybrid IS-FDP continue to provide satisfactory clinical outcomes, with their main advantage being their ease of repairability.
There is a lack of consensus on nomenclature to describe the process of stripping and replacing the veneering material of a hybrid IS-FDP on an existing framework. “Retread”5 is the most common term used in existing literature and is most widely accepted. To provide better continuity and communication between clinicians and researchers, one universal term should be adopted for use and proposed for inclusion in the Glossary of Prosthodontic Terms.2
Indications for retread include significant wearing or chipping of the veneering material, a loss of VDO, and/or a history of repeated fractures. It is precluded by a well-designed, passively fitted framework. There are various methods that can be used to perform a retread of an existing IS-FDP framework, two of which are described in this paper. The clinical approach varies depending on the planned treatment, status of the opposing arch and existing records (previous implant master cast, mounted models of original prosthesis after fabrication capturing VDO, existing provisional restoration). Through retreading, an IS-FDP can continue to provide many years of service and extend the lifetime of the restoration. 
Oral Health welcomes this original article.
References
- Sadowsky SJ. Evidence-based implant treatment planning and clinical protocols. John Wiley & Sons, Inc.; 2017:xii, 387 pages.
- The Glossary of Prosthodontic Terms 2023: Tenth Edition. J Prosthet Dent. Oct 2023;130(4 Suppl 1):e7-e126. doi:10.1016/j.prosdent.2023.03.002
- Papaspyridakos P, Chen CJ, Chuang SK, Weber HP, Gallucci GO. A systematic review of biologic and technical complications with fixed implant rehabilitations for edentulous patients. Int J Oral Maxillofac Implants. 2012;27(1):102-10.
- Papaspyridakos P, Bordin TB, Kim YJ, et al. Technical Complications and Prosthesis Survival Rates with Implant-Supported Fixed Complete Dental Prostheses: A Retrospective Study with 1- to 12-Year Follow-Up. J Prosthodont. Jan 2020;29(1):3-11. doi:10.1111/jopr.13119
- Balshi TJ, Wolfinger GJ, Alfano SG, Balshi SF. The Retread: A Definition and Retrospective Analysis of 205 Implant-Supported Fixed Prostheses. Int J Prosthodont. 2016;29(2):126-31. doi:10.11607/ijp.4277
- Chochlidakis K, Einarsdottir E, Tsigarida A, et al. Survival rates and prosthetic complications of implant fixed complete dental prostheses: An up to 5-year retrospective study. J Prosthet Dent. Nov 2020;124(5):539-546. doi:10.1016/j.prosdent.2019.11.022
- Heitz-Mayfield LJ, Needleman I, Salvi GE, Pjetursson BE. Consensus statements and clinical recommendations for prevention and management of biologic and technical implant complications. Int J Oral Maxillofac Implants. 2014;29 Suppl:346-50. doi:10.11607/jomi.2013.g5
- Piermatti J, Barndt P, Thalji G. Maintenance of Full-Arch Implant Restorations. Position Statement of the American College of Prosthodontists2023.
About the authors

Dr. Catherine Kucey is a third-year resident of the University of Toronto graduate prosthodontics program. Originally from Edmonton, AB., she completed her DDS degree from the University of Alberta (2020) as the gold medal graduate and worked as a general dentist for 3 years prior to pursuing specialization.

Dr. Somogyi-Ganss graduated as a dentist at Semmelweis University of Medicine, Budapest, Hungary. She continued her education at the University of Toronto, Faculty of Dentistry, and completed a specialty training and an MSc in Prosthodontics. Following that, she was accepted to the MD Anderson Maxillofacial Prosthodontics and Oral Oncology fellowship program, where she has gained a solid foundation for her future career. After completion of this program, she had returned to Canada and now works as a full time Associate Professor in Prosthodontics at the University of Toronto, Faculty of Dentistry.