
Hyperdontia of the permanent dentition occurs in approximately 0.1% to 3.8% of patients, with a range of ethnic variability. The vast majority of cases (76% to 86%) represent a single supernumerary tooth, with development of 2 supernumerary teeth observed in 12% to 23% of cases, and 3 or more supernumerary teeth found in less than 1% of cases.1 The etiology of hyperdontia is considered to be development of excess dental lamina leading to additional tooth buds. In many cases there is a familial tendency which is autosomal recessive. While development of supernumerary teeth may be related to an underlying syndrome (e.g., cleft lip and palate, cleidocranial dysplasia or Gardner syndrome), the majority of cases present as nonsyndromic.2 The most commonly affected site is the maxillary incisor region, followed by maxillary fourth molars and mandibular fourth molars, premolars, canines and lateral incisors. Supernumerary teeth may develop long after eruption of the permanent dentition. Publications have documented supernumerary bicuspids arising up to 11 years after completion of development of normal teeth. This paper reports a case of late development of supernumerary fourth and fifth molars in the maxilla.
Case report
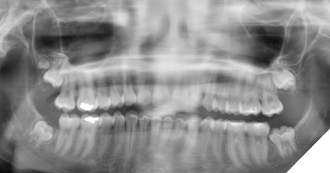
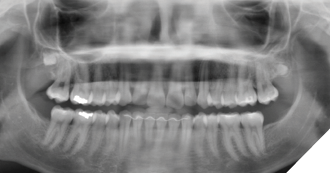
A 15-year-old female was referred for evaluation of impacted third molars. She was asymptomatic with a noncontributory medical history. Clinically, the impacted teeth exhibited completes emergence with no permucosal exposure. Panoramic radiography confirmed impaction of teeth #18, 28, 38 and 48, with suspected early development of a right maxillary supernumerary fourth molar. The maxillary third molars were positioned high in the maxilla, and surgery was deferred to allow further descent of these teeth (Fig. 1).
Fig. 1

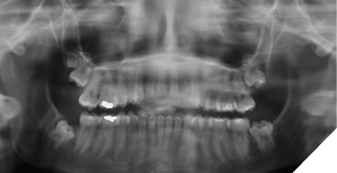
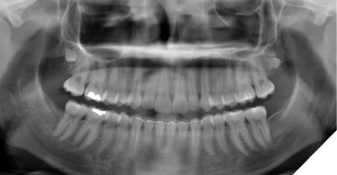
The patient was seen again 1 year following for radiologic reassessment and remained asymptomatic. The maxillary third molars were noted to have descended relative to the primary assessment, with increased mineralization of the maxillary supernumerary tooth (Fig. 2).
Fig. 2
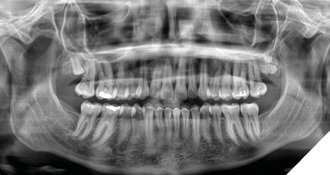
The patient was seen again one year later and deemed appropriate to proceed with surgery. Teeth #18, 28, 38 and 48 were removed under general anesthesia. Tooth #19 was retained due to its high position, and the patient remained in follow-up (Fig. 3).
Fig. 3
At the next follow-up one year later (18 years of age) the right maxillary supernumerary was relatively unchanged in position; however, a new supernumerary fourth molar was identified in the left posterior maxilla (Fig. 4).
Fig. 4
Both teeth exhibited gradual descent from their initial positions one year following (Fig. 5), and the patient was reappointed in two years.
Fig. 5
At the two-year follow-up (21 years of age), updated panoramic radiology revealed the presence of an additional supernumerary fifth molar in the second quadrant (Fig. 6). There was no pathology associated with any of the three supernumeraries. The patient remained asymptomatic, and clinical examination confirmed the absence of inflammation of the contiguous soft tissues. The patient remains in follow-up to monitor for further late odontogenesis and has been referred for genetic testing.
Fig. 6
Discussion
While supernumerary teeth are often diagnosed in the early to late mixed dentition stage, such teeth may present beyond development of the third molars. The genesis of supernumeraries has been ascribed to hyperactivity of the dental lamina leading to an accessary tooth bud.4 While supernumeraries do not usually cause resorption, if allowed to develop roots the associated eruptive potential can lead to resorption of adjacent teeth.4 In addition to the risk of resorption, retention of supernumerary teeth may also be associated with development of cystic pathology and ankylosis.4,5,6 Removal of supernumeraries is indicated due to these risks.2 Patients who develop multiple supernumerary teeth should be considered for genetic workup to rule out underlying syndromes.7Clinicians should inform patients of the possibility of the late development of additional supernumerary teeth,6 and long-term monitoring for late tooth development may be warranted.3 
Oral Health welcomes this original article.
References
- Neville BW, Damm DD et. al: Abnormalities Of Teeth. In: Oral and Maxillofacial Pathology, 5th Edition. Elsevier, 2024.
- Koenig LJ et. al.: Developmental Alternations in Size and Shape of Teeth. In: Diagnostic Imaging Oral and Maxillofacial, 2nd Edition. Elsevier, 2017
- Bozkurt M, Bezgin T. et., al. Late Developing Supernumeraries in a Case of Nonsyndromic Multiple Supernumerary Teeth. Case Rep Dent . 2015 Jan 11;2015:840460.
- Primosch R. Anterior supernumerary teeth: assessment and surgical intervention in children. Pediatr Dent. 1981;3(2):204-215.
- Nazif MM, Ruffalo RC, Zullo T. Impacted supernumerary teeth: a survey of 50 cases. J Am Dent Assoc. 1983;106(8):201-204. doi:10.14219/jada.archive.1983.0390.
- Craig R., McBride A. et. al. Metachronous supernumerary teeth in a non-syndromic patient. JIDA. Published online November 8, 2024. doi:10.58541/001c.125533.
- Lubinsky M et al: Syndromes with supernumerary teeth. Am J Med Genet A. 170(10):2611-6, 2016.
About the author

Dr. Marshall Freilich is a board-certified Oral and Maxillofacial Surgeon and holds a Master of Science degree in Orofacial Pain and Oral Medicine. He is a staff surgeon at Humber River Hospital, and maintains a private practice in Toronto, Canada.