


The Periodontal-Restorative Interface: Biologic and Aesthetic Considerations
When designing the optimal aesthetic outcome for a patient during the smile rejuvenation process, the restorative dentist must seek to create a symmetrical and harmonious relationship between the lips, gingival architecture, and the positions of the natural teeth. This diagnostic methodology is facially generated treatment planning, where the maxillary central incisal edges determine the soft tissue (gingiva) and bone positioning in space.1 A patient compromised by asymmetric gingival architecture and/or biologic width encroachment may be treated utilizing a variety of surgical approaches. The Er, Cr: YSGG laser is an extremely useful adjunctive instrument that performs aesthetic surgical crown lengthening procedures. The versatility of the Er, Cr: YSGG laser in recontouring both hard and soft tissues empowers a minimally invasive approach in the repositioning of the periodontal structures for aesthetic or restorative reasons. This laser decreases the need for suturing, reduces postoperative discomfort, as well as shortening healing times. The following cases demonstrate Er, Cr: YSGG laser techniques for osseous crown lengthening procedures, specifically highlighting:
- Biologic principles required for proper periodontal repositioning.
- Criteria for developing a biologically stable free gingival margin.
- Er, Cr: YSGG laser guidelines for open and closed osseous crown lengthening, considering biotypes.
- Er, Cr: YSGG laser benefits and their impact on both the clinician and patient.
The Dentogingival Complex and Its Relation to the Restorative Margin
The dentogingival complex consists of:
1) Connective tissue attachment
2) Epithelial attachment (or junctional epithelium)
3) Gingival sulcus
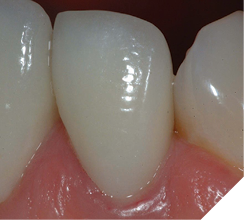
The most critical relationship for biologic health for a dental restoration at or below the free gingival margin, is the margin location relative to the crest of bone.2 The “magic” distance from the free gingival margin to the osseous crest on the facial aspect is 3 millimeters. Interproximally, on anterior teeth, due to the cementoenamel junction curvature (scallop), that number is 4mm. The interdental papilla height between anterior teeth with normal root proximity (2mm at the osseous crest) is generally maintainable 4mm incisal to the osseous crest (Figs. 1-4). The first restorative decision is to locate the restorative margin. For all-ceramic restorations that do not need to block out undesirable dentin or core materials show-through, the restorative margin is best at the free gingival crest, or slightly supragingival.
Fig. 1
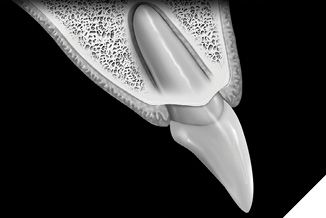
Fig. 2

Fig. 3
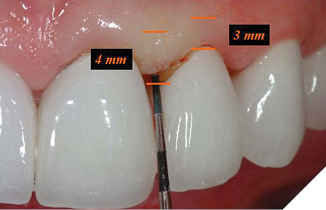
Fig. 4

With the “contact lens effect”, restorative margins can be placed in the equicrevicular and supracrevicular positions without an aesthetic compromise.3 However, if an intracrevicular margin is required, it should extend no further than 0.5mm into the gingival sulcus to avoid adverse biologic responses due to encroachment upon the attachment apparatus.
The variation in biologic width (comparing the alveolar crest-free gingival margin distance) can be divided into three categories:4,5
1) Normal crest – 70% of patients have 2mm combined epithelial and connective tissue attachment and 1mm sulcus depth. If the sulcus depth >1mm, the free gingival excess can be safely resected, and upon healing, will result in a 3mm dentogingival complex on the facial aspect.
2) High crest – shallower sulcus depth and a combined epithelial and connective tissue attachment of <2mm, with a relatively stable free gingival margin. These patients are not prone to recession upon mechanical or surgical tissue manipulation.
3) Low crest – normal sulcus depth (1-3mm) with a combined epithelial and connective tissue attachment <2mm. These patients are very prone to recession and must be treatment-planned accordingly. The free gingival margin of low crest patients tends to apically reposition and turn into a normal crest situation after gingival retraction or surgery.
The most important factor in post restorative gingival health and stability is the positioning of the restorative margin relative to the bony crest, not the preoperative health and/or position of the gingival tissues.
Smile Design and Tooth Dimension
Correct positioning of the restorative margin relative to the crest of the alveolar bone is critical to biologic success but does not address aesthetic/proportional issues or the gingival scallop positions relative to one another. The following parameters must be considered when designing a proportionally esthetic smile rejuvenation:
1) Width to length ratio of the maxillary central incisor. The average maxillary central incisor width is 10mm,6 and the length is 10-12mm.
2) Mesio-distal proportional width (Golden Proportion) of the maxillary anterior teeth. The maxillary central incisor is 1.6 times as wide as the maxillary lateral incisor. A proportional lateral with an esthetically pleasing width to length ratio of 75-80% will be 7.5-8mm wide.
3) The relative amount of tooth display of the maxillary central incisors (ideally 50 to 70%) when the patient says “e”.
4) Relative gingival zenith positions and heights of contour of the centrals and the canines are 1mm higher apically than the laterals. The gingival heights of contour (zeniths) are located at the distolabial line angles creating, a “raised eyebrow” or “gull wing effect” over the maxillary incisors.7
Attention to these parameters permits the “spatial repositioning” required to create symmetry and enhance aesthetic outcomes.
The Er, Cr: Yssg Laser Used For “Open” And “Closed” Crown Lengthening Procedures
The use of Er, Cr: YSGG laser for gingival and bone recontouring is redefining periodontal surgery. The end-cutting laser makes soft and hard tissue resection control more predictable than rotary or hand instrumentation. A tapered tip Er, Cr: YSGG allows surgically precise scalloped gingivectomies with no bleeding. Traditional rotary instrumentation for osseous resection risks damaging adjacent root surfaces. The surgical laser wound is less traumatic, decreasing bony damage due to frictional heat, always a possibility with inadequate water-cooling. Minimally invasive laser surgery offers less postoperative discomfort and quicker healing times for the patient.8
Cosmetic Recontouring of Gingival Tissues and Alveolar Bone (“Open” Surgical Crown Lengthening) To Eliminate Excessive Gingival Display and Create Esthetic Harmony
The esthetic smile shows 3-5mm of gingiva, ideally with right-left symmetry for cervico-incisal tooth height and gingival zenith positioning. Patients with asymmetrical gingival levels, “gummy smiles” (>3-5mm of soft tissue display), or both, are good candidates for aesthetic surgical gingival and/or alveolar bone repositioning. Typically, these patients have adequate attached gingiva; there are no muco-gingival junction issues post-operatively. Minor asymmetries can be corrected with gingivectomy or gingivoplasty alone. A minimum 1mm sulcus depth must always remain after any tissue resection unless the alveolar bony crest is also repositioned apically. To create the appearance of spatial relocation of teeth in the cervical direction, osseous correction must accompany soft tissue resection to respect sulcus depth.
During surgical planning towards the central incisor height of 10-12mm, the incisal edges can be shortened as long as adequate posterior freeway space for appropriate disclusion exists. The shortened incisal edges must still disclude the posterior teeth in all eccentric movements to maintain occlusal harmony. A tissue marker can be used to plan the soft tissue surgery (Fig. 5).
Fig. 5

Following the esthetic tissue guidelines, the perceived final gingival level is traced, creating heights of contour at the distolabial line angles. The Er, Cr: YSGG laser removes the excess gingival tissue and creates the proposed symmetry. Next, the preparation margins are adjusted to the corrected free gingival margins. Since biologic width will be encroached upon, an appropriate amount of bone must be removed to recreate normal biologic parameters. Following an internal bevel incision, a full thickness mucoperiosteal flap is elevated using a periosteal elevator. The alveolar crest correction is made using the Er, Cr: YSGG laser with a 600µ tip (Z-14), or a 9mm 600µ tip (G-9). Since the laser only cuts at the tip, it is set against the side of the root parallel to the long axis of the tooth (Fig. 6). This ensures that the dentin/cementum surface (root) is never damaged. A black marker guide line is placed at a point 3mm from end of the tip to apically position the bone 3mm from the restorative margin. Only the alveolar bone is ablated by the laser energized water. The root surface is then planed with a back action chisel. The alveolar architecture now mimics the restorative margin 3mm apically, allowing for biologic width restoration to a normal crest position. For facial esthetic correction cases the interproximal bone is not altered. The flap is sutured with 3-0 silk in an interrupted technique (Fig. 7). If the flap section requires leveling or adjustment after suturing to blend gingival levels, the Er, Cr: YSGG laser is utilized at a soft tissue setting. At the delivery appointment, the gingival zenith heights of the centrals are adjusted apically with a “closed” crown lengthening technique, described in the next section (Fig. 8). The definitive restorations three years after corrective gingival and bony surgery with the Er Cr, YSGG laser (Fig. 9).
Fig. 6
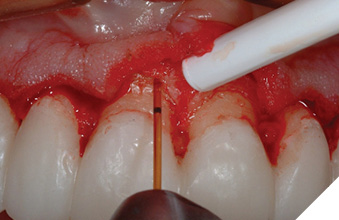
Fig. 7

Fig. 8

Fig. 9

Surgical Crown Lengthening – “Closed” Technique
The Er, Cr: YSGG laser corrects and completes the minor, localized biologic width and/or aesthetic gingival zenith correction process with reduced healing time compared to the flap procedure required for “open” crown-lengthening surgeries.9 Patients with normal to thick keratinization are good candidates for this procedure. A small percentage of thin keratinization patients may require a secondary “open” procedure to further refine the bone/tooth interface. The “closed” approach should not be used to dig a circumferential trough around a tooth; an “open” surgical technique offers more visibility and access.
The soft tissue is resected with a 400µ tapered tip facially and a 600µ tip proximally, creating the new apical position and scallop of the free gingival margin. A periodontal probe sounds the osseous crest to determine its distance from the free gingival crest. A 9mm 600µ laser tip held adjacent to the tooth and “walked” across the affected area with an up-and-down “sewing machine” movement to remove bone to a 3mm depth (Fig. 10).
Fig. 10
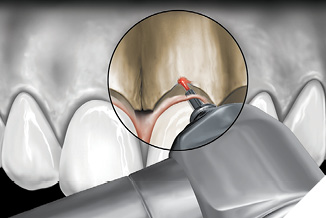
Once the corrected crestal level is established, the bone is “smoothed” by the Waterlase MD (Biolase Technologies, Foothill Ranch, CA) at 50 pulses per second, and horizontal movement of the tip over the crestal bone. The tip of the laser is in contact with the bony crest with both movements. For aesthetic crown lengthening procedures, maxillary bone is resected only in the top arc (10-2 clock face positions) and mandibular bone is resected only in the bottom arc (4-8 clock face positions). A periodontal probe verifies depth to 3mm (Figs. 11-13). For interproximal biologic width corrections, the laser tip is angled slightly away from the tooth to blend adjacent bone and to avoid “trenching” (Figs. 14, 15). A final impression and cemented provisionals complete this phase, with definitive restorations seated 2-3 weeks after the “closed” crown lengthening procedure. The secondary intention healing of the surgical area around the finished restoration is the most desirable (Fig. 16).
Fig. 11

Fig. 12

Fig. 13

Fig. 14
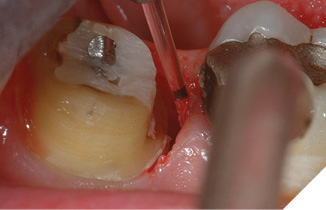
Fig. 15
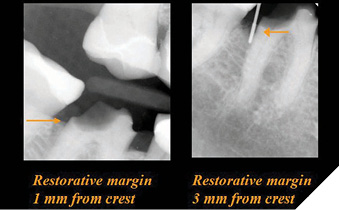
Fig. 16

The criteria for clinical health of the dentogingival complex include:
1) Pink color (absence of inflammation)
2) Reestablishment of a gingival sulcus
3) Absence of bleeding upon probing
It may be the case that a “closed” procedure does not allow the same smoothing of the bony crest as the “open” approach. But is this clinically significant? If the healed tissue fits the above criteria, the answer is simple (Figs. 17-20). Three-year follow-ups clinically document the criteria for maintained periodontal health following the “closed” crown lengthening technique with the Er, Cr, YSGG laser.
Fig. 17

Fig. 18

Fig. 19
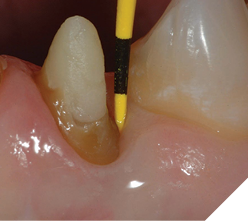
Fig. 20
Epilogue: A Paradigm Shift in Surgical Tissue Management
Er, Cr: YSGG lasers offer innovative periodontal crown lengthening opportunities. The biologic parameters described above enable both facial and interdental “open” periodontal procedures and accurately predict the healing levels based on the positioning of the restorative margins. It is essential to sound the depth from the free gingival margin to the alveolar crest with a periodontal probe to determine the biologic parameters prior to preparing teeth for restoration. Final impressions are taken on the day of preparation and surgery, and definitive restorations are delivered several weeks later, with full confidence that the gingival tissues will heal to the appropriate aesthetic levels (Figs. 21, 22). The decreased time spent in provisionals, and the tissues maturing around the new ceramic restorations are beneficial to both patient and dentist.
Fig. 21

Fig. 22

References
- Spear FM, “Diagnosis and Treatment Planning Inadequate Tooth Display”, British Dental Journal, Vol 221, No. 8, October 2016, pp. 263-272.
- Kois JC, “Altering Gingival Levels: The Restorative Connection Part 1: Biologic Variables”, Journal Of Esthetic Dentistry, Volume 6, Number 1, 1994, pp. 3-9.
- Materdomini D, Friedman MJ, “The Contact Lens Effect: Enhancing Porcelain Veneer Esthetics”, Journal Of Esthetic Dentistry, Volume 7, Number 3, 1993, pp. 99-103.
- Kois JC, “Altering Gingival Levels: The Restorative Connection Part 1: Biologic Variables”, Journal Of Esthetic Dentistry, Volume 6, Number 1, 1994, pp. 3-9.
- Coslet GJ, Vanarsdall R, Weisgold A, “Diagnosis and Classification Of Delayed Passive Eruption Of The Dentogingival Junction In The Adult”, Alpha Omegan, December 1977, pp. 24-28.
- Kois JC, “ New Paradigms For Anterior Tooth Preparation”, Oral Health, Volume 88, Number 4, April 1998, pp. 19-30.
- Shavell HM, “Extreme Occlusal Makeover: A Morphoaesthetic Approach To The Dynamics Of Occlusion” Lecture at The Holiday Dental Conference, Charlotte, NC, November 17, 2005.
- Dean DB, “Concepts In Laser Periodontal Therapy: Using The Er, Cr:YSGG Laser”, The Academy Of Dental Therapeutics And Stomotology A Peer-Reviewed Publication, Continuing Education Course, 2005.
- Lowe RA, “The Use Of Dental Lasers And Ridge Preservation To Maximize Esthetic Outcomes” Contemporary Esthetics And Restorative Practice, Volume 8, Number7, July 2004, pp.48-53.
About the Author

 Dr. Robert A. Lowe graduated Loyola University magna cum laude. He is Assistant Professor in the Department of Oral Rehabilitation, Medical University of South Carolina and a clinical evaluator of materials and products. He lectures internationally and publishes extensively on esthetic and restorative dentistry. Dr. Lowe has been awarded Fellowships in the AGD, ICD, ADI, ACD, ASDA, IADFE and DiplABAD, and received the 2004 Gordon Christensen Outstanding Lecturers Award. A founding member of the World Clinical Laser Institute, Dr. Lowe maintains a part-time private practice in Charlotte, North Carolina.
Dr. Robert A. Lowe graduated Loyola University magna cum laude. He is Assistant Professor in the Department of Oral Rehabilitation, Medical University of South Carolina and a clinical evaluator of materials and products. He lectures internationally and publishes extensively on esthetic and restorative dentistry. Dr. Lowe has been awarded Fellowships in the AGD, ICD, ADI, ACD, ASDA, IADFE and DiplABAD, and received the 2004 Gordon Christensen Outstanding Lecturers Award. A founding member of the World Clinical Laser Institute, Dr. Lowe maintains a part-time private practice in Charlotte, North Carolina.