


The oral and maxillofacial surgeon or potentially other dental practitioner may be called upon to assess and examine dental injuries, and oftentimes these patients may present with concomitant injuries to other structures outside the dentoalveolar complex, such as the midface. The dental practitioner’s role in recognizing midface fractures and related injuries extends beyond dental structures. Our unique training and comprehensive understanding of facial anatomy and functional relationships provides a strong foundation that may be of significant utility for recognizing these injuries that may result in significant functional impairment and disability if not identified and managed in a timely manner. We present a case of an 18-year-old male referred to our tertiary care centre who sustained significant midface fractures and soft tissue injuries after an ATV rollover accident.
Case Report:
A healthy 18-year-old male was transferred from Thunder Bay Regional Health Sciences Centre to our tertiary care centre in Toronto at the graduate program for oral & maxillofacial surgery for the secondary management of complex facial fractures and soft tissue injuries. The patient sustained facial injuries after being ejected from an ATV. The event was reportedly unwitnessed, and the patient only recalls that his face struck tree/foliage upon ejection from the ATV. There was no loss of consciousness and the influence of alcohol/illicit substances were not a factor in the incident. The patient was brought to the emergency department in Thunder Bay where he was seen by the on-call oral and maxillofacial surgeon. His left facial lacerations were sutured (Fig. 1) and CT head , C- spine and Facial bones were obtained. He was also assessed by an ophthalmologist in the emergency department. Remarkably, he was found to have no injuries to the left globe. After initial stabilization and assessment he was transferred to Toronto for definitive management of his facial injuries.
Fig. 1

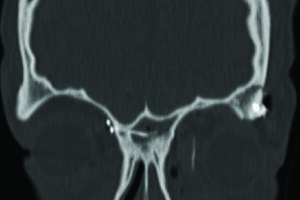
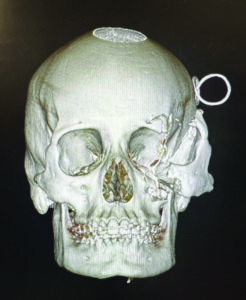
On reviewing his computed tomography scan (CT scan) it was determined that he had no intracranial or C-spine injuries and his skeletal injury was limited to his midface region involving comminuted displaced fracture of the anterior and lateral wall of the maxillary sinus, displaced fracture of the left orbital floor involving the infraorbital foramen and herniation of orbital fat, fracture of the medial orbital wall/lamina papyracea of the left orbit and displaced fracture of the left lateral orbital wall (Figs. 2A&B), there was also a displaced fracture of the left malar complex and zygomatic arch are about one inch off the skull (Fig. 2C). The left globe, is stretched laterally along with the malar complex, the medial and lateral pterygoid plates, mandible were intact.
Fig. 2A
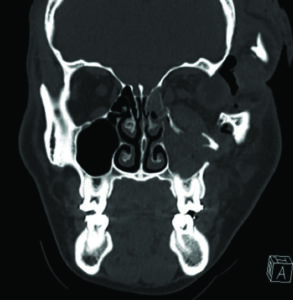
Fig. 2B
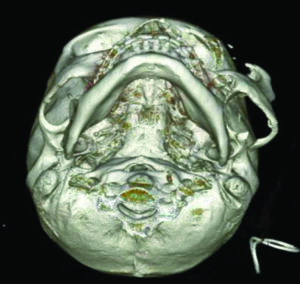
Fig. 2C

A through evaluation was performed under general anesthesia to further characterize the extent of soft tissue injuries, which showed avulsion of the medial canthal tendon, laceration of the nasolacrimal system and lacrimal sac, complex >15 cm facial laceration, and left upper eyelid laceration (Fig. 3). Traumatic telecanthus was present as a result of the laterally displaced fracture and medial canthus avulsion (intercanthal distance of 50mm compared to average of 31-35 mm) (Fig. 4).
Fig. 3

Fig. 4

Access to the fractures utilizing an extension of an existing laceration into a hemicoronal flap (Fig. 5).
Fig. 5

Identification of the zygomatic arch fracture (Fig. 6A) and fracture of the left orbital floor (Fig. 6B).
Fig. 6A
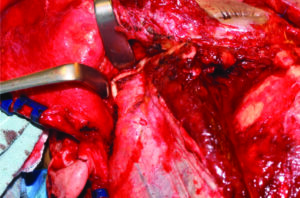
Fig. 6B

The severed ends of the lacerated nasolacrimal duct was identified and tagged with sutures (Fig. 7).
Fig. 7

The bony segments were stabilized by first reducing the zygomatic arch to correct the anterior-posterior projection and facial width, followed by plating the fronto-zygomatic suture (Fig. 8), next the zygomaticomaxillary buttress was stabilized and the comminuted bony fragments of the anterior wall of the maxillary sinus were re-approximated, finally the left orbital floor was reconstructed by extending the orbital plate medially and making sure that the plate rested on the posterior ledge of the orbital floor to regain the pre-trauma orbital volume (Fig. 9).
Fig. 8
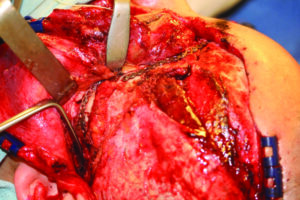
Fig. 9

On completion of plating the bony architecture, the focus was shifted on treating the soft tissue injuries which began with correctly repositioning the medial canthus to proper position. Medial canthopexy was performed by making a 1 cm incision on the contralateral medial eyebrow (Fig. 10A) and an osteotomy from the right orbit into the left orbit to pass a 28 gauge stainless steel wire, which was attached to the 3-0 prolene sutures that were used to tag the severed medial canthal tendon (Fig. 10B, Intra op and C, Post op CT scan). Resuspension into appropriate position was performed by gaining a vector of pull in a superior, posterior and medial direction from the contralateral side. The 28 gauge wire was secured to a 5 hole miniplate fixed to the right supraorbital rim.
Fig. 10A

Fig. 10B

Fig. 10C
The lacerated nasolacrimal duct was repaired by threading bicanalicular stent from the superior and inferior puncta which was delivered from the superior end of the severed duct (Fig. 11A). We were unable to further thread these ends to the inferior end of the severed duct due to significant tearing of the duct from the injury, so a new passage was was created by performing a dacryocystorhinostomy (DCR), which involved puncturing the lateral wall of the nose into the inferior meatus and tying both the free ends of the stent (Fig. 11B).
Fig. 11A

Fig. 11B

Subsequently the upper eyelid was repaired in a layered fashion by re-approximating the tarsal plate with a 5-0 vicryl, the gray line with a 6-0 vicryl vertical mattress and closure of skin with a 5-0 fast gut suture (Fig. 12).
Fig. 12

Lastly the coronal flap was re-approximated and the laceration was repaired using 2-0, 3-0, 4-0, 5-0 vicryl at different aspects of laceration for deep closure with a running 3-0 chromic gut for coronal skin. A 10 JP drain was inserted exiting the left coronal incision, which was secured with a 3-0 slik suture. An antibiotic ointment was placed on the skin incision and the left nare was packed with merocel pack coated with antibiotic before shifting the patient to recovery unit where he was extubated and neural check were performed Q1H for first 24 hrs.
Post-op CT was obtained within 24 hours which demonstrated adequate bony fixation and restoration of the bony architecture in the A-P, transverse and vertical dimensions (Fig. 13A&B) with the pre-op CT scan for comparison.
Fig. 13A
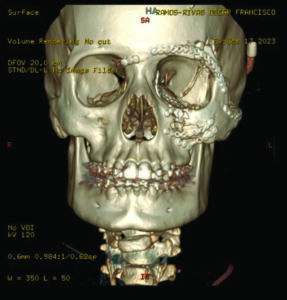
Fig. 13B
Discussion
The aforementioned case serves as a point of discussion regarding the functional and cosmetic sequelae of midface fractures, specifically, management of the naso-orbital-ethmoid fractures. We will discuss two important components that were addressed in this case: The avulsed medial canthal tendon and the nasolacrimal apparatus.
The medial canthal tendon is an anatomic structure that contains an anterior component, which attaches to the frontal process of the maxilla, and is involved in pulling the medial commissure of the eyelid forward and down. The posterior component inserts into the posterior lacrimal crest and functions to position the eyelid in relation to the globe. It is also involved in lacrimal drainage with its association to Horner’s muscle. Signs of medial canthal ligament disruption may include increased intercanthal distance (the distance between the inner and outer corners of each eye), and epiphora (excessive tearing). The normal intercanthal distance is 31-35mm, and an increase in this distance can result in a significant cosmetic deformity.1 Aside from measuring the intercanthal distance, one can perform a bowstring test, which is performed by pulling the eyelid laterally while palpating the medial canthal tendon to detect movement of the fracture segment. Avulsion of the medial canthal tendon requires surgical resuspension of the tendon slightly superior and posterior to its original position to mitigate forces of relapse and migration.2
The nasolacrimal apparatus is the central component of the eye’s tear drainage system, consisting of the lacrimal gland, puncta, canaliculi, lacrimal sac, and nasolacrimal duct.3 Recognizing such injuries involves a thorough clinical assessment and may require imaging studies to evaluate the anatomy and functionality of the tear drainage system. Cotton tip applicators can be used to gently inspect the lacrimal and canthal area. Fluorescent dye can be utlilized to identify the potential tear and/or inability for the dye to pass through the canalicular system. One must have a high index of suspicion for a canalicular laceration if the injury is medial to the puncta. Consequences of nasolacrimal apparatus injuries include epiphora, which can lead to blurred vision, skin irritation, and social discomfort. Blockages or obstructions in the system can cause dacryocystitis (inflammation of the lacrimal sac) characterized by pain, swelling, and purulent discharge. Furthermore, untreated injuries can result in chronic tear drainage issues, and potential complications affecting the ocular surface. If a tear between the puncta and the lacrimal sac is noticed, surgical repair options may include intubation of the canaliculi and nasolacrimal duct for a period of 12-20 weeks, or a dacryocystorhinostomy (DCR), where a new drainage pathway is created to bypass obstructions and allow tears to flow into the nasal cavity.4 
Oral Health welcomes this original article.
References
- Ellis, E. (1993). Sequencing treatment for Naso-Orbito-ethmoid fractures. Journal of Oral and Maxillofacial Surgery, 51(5), 543–558.
- Markowitz, B. L., Manson, P. N., Sargent, L., Vander Kolk, C. A., Yaremchuk, M., Glassman, D., & Crawley, W. A. (1991). Management of the medial canthal tendon in nasoethmoid orbital fractures: The importance of the central fragment in classification and treatment. Plastic and Reconstructive Surgery, 87(5), 843–853.
- Fonseca, R. J., & Eberts, A. (2013). Oral & Maxillofacial trauma. Elsevier.
- Kademani, D., & Tiwana, P. (2023). Atlas of Oral and Maxillofacial Surgery. Elsevier.
About the Authors
Dr. Freddy Mistry is an Oral & Maxillofacial Surgery PGY-1 resident at the University of Toronto.

Dr. David Au is an Oral & Maxillofacial Surgery PGY-3 resident at the University of Toronto.

Dr. Bruce Pynn is the Chief of Dentistry/Oral and Maxillofacial Surgery at Thunder Bay Regional Health Sciences Centre and Assistant Professor at the Northern Ontario School of Medicine.

Dr. Karl Cuddy is an Assistant Professor and Director of Education and Maxillofacial Trauma for the Graduate Training Program in Oral and Maxillofacial Surgery at the Faculty of Dentistry, University of Toronto.