


Abstract
Background: Partial edentulism (Fig. 1) of the maxilla presents unique prosthodontic challenges, especially in elderly patients with a failing dentition (Figs. 2, 3) and a compromised occlusion. Conventional well-designed Kennedy`s Class 1 partial dentures function very efficiently but over many years of use can often encounter issues with loss of support due to progressive ridge resorption (Fig. 4), which often leads to loss of retention and stability. In addition, Kennedy Class I RPDs may have adverse esthetic and psychological implications. The need for visible clasps (Fig. 5) on anterior abutments can affect smile esthetics, while the bulk of the prosthesis may reduce patient comfort and adaptation. One of the other challenges of the metal clasps are slow, long-term abrasion (Fig. 6) to the cervical junctions of the teeth involved, often causing sensitivity and pulpal pain. Combined with functional inadequacies, these disadvantages often reduce overall patient satisfaction and can negatively influence oral health-related quality of life.
Keywords: equipoise system, maxillary implant retained denture, removable prosthesis, dental implants, elderly patient rehabilitation
Implant-assisted removable prostheses (IARPDs) with an equipoise system may offer a balance between function, biomechanics, and patient acceptability.
Fig. 1

Fig. 2

Fig. 3

Fig. 4

Fig. 5

Fig. 6

Case presentation:
Patient profile: A 70-year-old non-smoking male, presented with complaints of loose teeth and difficulty chewing with his existing old partial denture. He has been wearing a removable denture for over 15 years. Cost of treatment had been a major deciding factor all these years to continue managing with a partial denture. Medical history included controlled hypertension and controlled type II diabetes mellitus (HbA1c 6.8%).
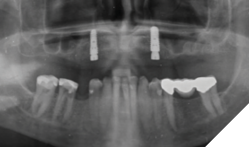
Clinical findings: On intra oral exam, he had a failing maxillary dentition with heavily restored teeth and multiple secondary decay. Soft tissue evaluation shows redness of the palate following the design of the partial denture; on enquiry patient admits not removing his partials at bedtime. Radiographic evaluation (Fig. 7) shows multiple root stumps and a large peri-apical lesion in the 22 region. Patient had a very low smile line (Fig. 8) and was not particularly concerned about aesthetics.
Fig. 7

Fig. 8

After a detailed discussion with the patient on his failing dentition in the upper arch with guarded to hopeless prognosis, the treatment plan included extractions of all maxillary teeth and retained roots, curettage of the endodontic lesion in 22 region, and guided bone regeneration to help preserve and maintain alveolar ridge dimensions for future implant therapy.
Multiple prosthodontic options were also presented including an upper complete removable denture, 4 implants with a milled bar and over denture on locators, multiple implants and a fixed upper full arch prosthesis. The patient was concerned for economics and enquired if an upper denture can be supported on just 2 implants. After a thorough search through prosthodontic concepts and consult with dental technician Michael Callaghan, the Equipoise system was evaluated and presented to the patient.
An Equipoise system incorporates load distribution to minimize off-axis forces into the removable prosthesis design. The plan was to place 2 implants in the canine regions and design a cast partial denture with the built in Equipoise system so the patient may benefit from an implant supported removable prosthesis that is both cost friendly and practical.
Definitive treatment plan:
- Extraction of remaining maxillary teeth and root stumps
- Alveoplasty with GBR in extraction sites to help preserve alveolar ridge dimension
- Placement of two implants in the canine regions (#13, #23)
- Interim complete partial denture during osseointegration phase
- Fabrication of a maxillary full-arch removable prosthesis secured over screw retained crowns with intra coronal attachments integrated (equipoise system design)
Treatment procedure
Surgical phase: After a detailed discussion and appropriate consent obtained, on the day of surgery the procedure was performed under local anaesthesia. Surgical extractions (Fig. 9) of all maxillary teeth and roots were performed. 4.5 x 11.5 and 5.0 x 11.5 implants (Fig. 10) were placed into the 13 and 23 regions as per protocol. GBR procedures (Fig. 10) were performed to graft the sockets and to help regenerate the lost buccal plate in the 23 region. Slow resorbing collagen membranes (Fig. 11) were carefully draped around the alveolar ridge to provide cell occlusive properties. PRF membranes (2700RPM at 13min) (Fig. 12A and 12B) were placed over the collagen membranes to help with wound healing. Complete passive primary closure (Fig. 13) was achieved with careful tissue release and suturing. A complete denture with soft reline was given to the patient as an interim provisional for 16 weeks. Patient was advised to not wear the denture while at home and use them only for aesthetic purposes or for his meal time, which consisted of a soft diet during the healing phase. At 4 months of healing, under local anaesthesia, a small crystal incision was given and healing abutments were placed (Fig. 14).
Fig. 9

Fig. 10

Fig. 11
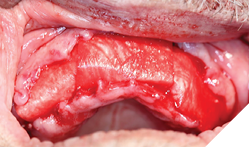
Fig. 12A

Fig. 12B
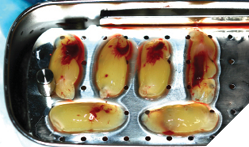
Fig. 13

Fig. 14
Prosthetic phase: After 16 weeks of osseointegration and 6 weeks of soft tissue healing post healing abutment placement, a custom tray was fabricated and an open tray impression technique (Fig. 15, 16) was performed using regular set medium phase PVS. Custom wax rims (Fig. 17) were made, jaw relation records recorded, and the occlusal plane was transferred to the articulator using the Kois Dento-Facial Analyzer (Fig. 18,19). Two weeks later, the lab had delivered the final prosthesis consisting of 2 modified screw retained PFM NP alloy restorations and a cast partial denture (Fig. 20) with built in vertical slots that will seat into the crowns.
Fig. 15
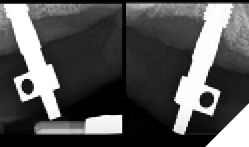
Fig. 16

Fig. 17

Fig. 18
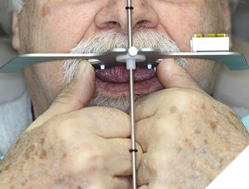
Fig. 19

Fig. 20

First the crowns were screwed onto the implants, hand tightened with passive seating (Fig. 21). Radiographs were taken to confirm seating with no microgap (Fig. 22). The restorations were final torqued at 30Ncm. The partial denture was then inserted, carefully seating into the vertical internal slots (Fig. 23) designed along the mesial and palatal portion of the screw retained crowns (Fig. 24). Occlusion was adjusted (Fig. 25), insert and removal techniques were demonstrated, and home care oral hygiene instructions were provided. The patient was happy (Fig. 26) with his final prosthesis. Post insertion and prosthetic follows ups were done at 2 weeks, 3 months and 6 months with minor denture adjustments and no major discomfort.
Fig. 21

Fig. 22
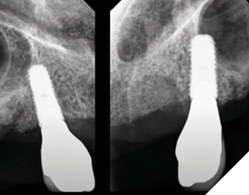
Fig. 23

Fig. 24

Fig. 25

Fig. 26

Results
At the 6-month follow-up:
- Patient outcomes: Excellent retention, stability, mastication, and esthetics compared to previous dentures.
- Implant health: Probing depths ≤3 mm, no bleeding on probing, healthy surrounding soft tissue.
- Prosthesis performance: Equipoise system demonstrated balanced retention with minimal rotational movement.
Discussion
Maxillary implant overdentures traditionally require multiple implants for long-term success. However, in elderly patients with systemic comorbidities, limited bone, or financial limitations require alternative approaches.
The Equipoise system’s design directs forces axially and minimizes torque, protecting both implants and mucosa. In this case, two anterior implants combined with Equipoise mechanics provided sufficient retention and stability. This strategy avoided extensive grafting or placement of multiple implants while achieving patient satisfaction.
Conclusion
This case demonstrates that an implant-assisted Equipoise-supported removable prosthesis is a predictable and cost-effective solution for elderly patients where extensive implant rehabilitation is not feasible. The approach provided functional, esthetic, and psychosocial benefits while minimizing surgical and financial burdens.
Careful patient selection and precise prosthetic design are essential for success. 
Oral Health welcomes this original article.
About the author

Dr. Joshua Shieh is a third generation clinician and has been practising general dentistry in Ontario since 2015. Over the last eight years, he has earned his Diplomate of the American Board of Oral Implantology, Fellow of the International Congress of Oral Implantology and Fellow of the Academy of General Dentistry. A travelling surgical associate in the GTA with special interests in wisdom teeth, hard and soft tissue regeneration around teeth / implants, surgical implant placements and full arch implant rehabilitations. The author can be reached out via email: drjoshuashieh@gmail.com