
Dental implants are the preferred treatment for edentulous and partially edentulous patients. Over the past decade there has been an increasing number of dental implants placed in patients each year.1 The longevity of dental implant integration is challenged with the increase in life expectancy. This increase in life expectancy is most often associated with an increase in the number of medications needed for the maintenance of life and the sustenance of optimum lifestyles. This article highlights the most prescribed medications which may have a potential clinical impact on bone remodeling and dental implant survival. Several of these medications directly alter bone homeostasis, while other medications work indirectly by adversely impacting the gut microbiome, the immune response and bone.
Bone homeostasis is significantly altered by various hormones and cytokines. The systemic levels of female hormones (e.g. estrogen), male hormones (e.g. testosterone), parathyroid hormones and calcitonin are involved in the pathophysiological mechanisms of bone density. Any medications or drugs that alter the levels of these hormones significantly impact the calcification of bone and may affect the osteointegrated bone around dental implants. Successful integration of dental implants is dependent on following cells: osteoblasts, osteocytes, osteoclasts, and regenerative cytokines. Osteoblasts activities are affected by estrogen, PTH, glucocorticoids, and vitamin D.2-7 Therefore, any medications that interfere with the activities of these bone cells should be considered in treatment planning dental implant rehabilitations.8 Clinicians should understand the systemic interaction of these medications on bone metabolism. The potential to control these complications can be recognized through understanding the medications’ impact on overall bone health.
Although a systematic review with meta-analysis indicates that dental implants placed in patients with osteoporosis do not directly have a higher risk of failure, it reports increased marginal bone loss of 1.8 millimeters around dental implants in patients with osteoporosis.9 The marginal bone loss ranged from 0.15 to 1.20 millimeters in patients with osteoporosis compared with healthy patients who demonstrated marginal bone loss from 0.06 to 0.87 millimeters. Therefore, there is a statistically significant difference in marginal bone loss in patients with clinical diagnosis of osteoporosis.
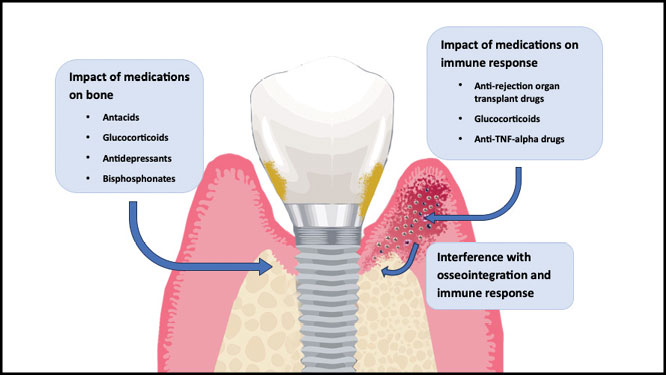
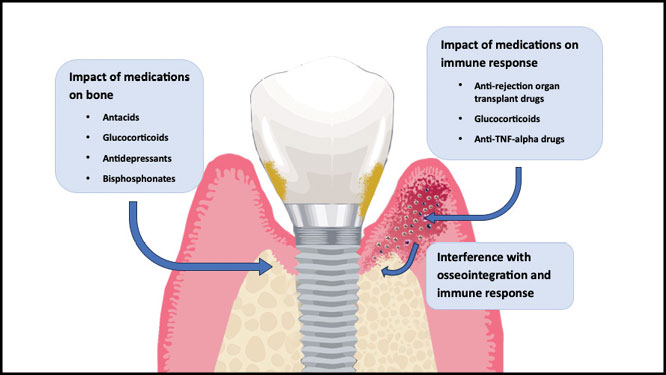
Medications associated with bone resorption around osteointegrated implants include glucocorticoids, anti-tumor necrosis factor (TNF)-alpha drugs, organ transplant medication, antacids, selective serotonin reuptake inhibitors (SSRIs), and bisphosphonates.10 Figure 1 illustrates the potential effects of selected medications on peri-implantitis. Conversely, there are also medications that improve bone density around dental implants. These medications include anti-hypertensive drugs.
Fig. 1
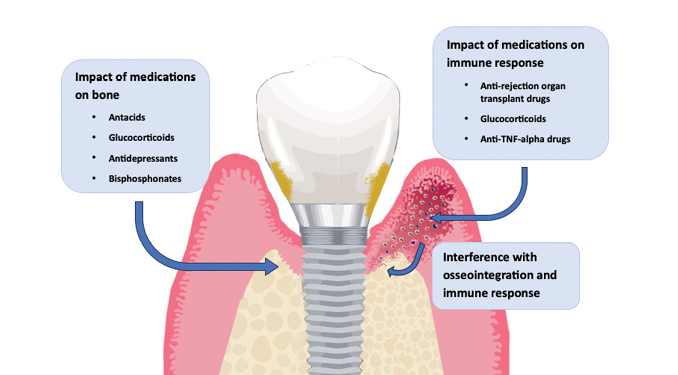
Medications affecting bone remodeling and immune response
Glucocorticoids
Glucocorticoids are commonly used in medicine for management of allergies, autoimmune diseases and selected anti-neoplastic therapies.11 It is well recognized that oral glucocorticoids can significantly impact osteocyte apoptosis, bone homeostasis and bone regeneration. Long-term chronic administration of high dose glucocorticoids caused bone loss in 40% of patients evaluated, increasing their fracture risk.12 Consequently, glucocorticoids may potentially cause osteopenia and osteoporosis.13-15 Glucocorticoids can also have an impact on immune response and defense mechanisms around dental implants.16, 17 The osteointegration of dental implants may be impacted by oral glucocorticoids in a week of starting the medication, becoming more pronounced at three months.18, 19 This interference of the immune response and bone metabolism can compromise the survival of dental implants.13-15
In addition, some patients who take oral glucocorticoids may concurrently take oral bisphosphonates and IV bisphosphonate drugs. This may further increase the risk of implant failure or peri-implantitis, since bisphosphonate use may be detrimental to implant success.15
In a murine study, excess glucocorticoids were reported to modulate the immunometabolism of the skeletal environment.13 The immunomodulatory effect of increased glucocortoids affected the macrophages and interfered with osteophysiology. Overall, excess glucocorticoids result in reduced bone turnover and net clinical loss of bone. This report emphasized on a molecular level the impact of bone resorption in patients who are on glucocorticoid therapies. This must be taken into consideration when treatment planning dental implants for these patients.13 Other studies showed direct impact of glucocorticoids on bone hemostasis. In implant patients taking glucocorticoids, osteointegration is significantly impacted.16
Anti-TNF-alpha drugs
Anti-TNF-alpha drugs are used to treat autoimmune diseases like Crohn’s disease, ulcerative colitis, psoriasis, and rheumatoid arthritis. Anti-TNF-alpha drugs include adalimumab, golimumab, certolizumab pegol, and etanercept.20 TNF-alpha is a pro-inflammatory cytokine which is released during stress or injury.21 Anti-TNF-alpha drugs have a negative impact on the immune system and interfere with bone and cartilage turnover.22
TNF-alpha increases osteoclast progenitor cells and stimulates their activity.23 TNF-alpha inhibition is linked to reduction of the osteoclast lifespan, and this interferes with bone remodeling and has a negative impact on the immune system.23 This decrease in the healing of the bone and the reduced immune defense may contribute to osteonecrosis in the jaw.20 A case report of a 63 year old female on Adalimumab receiving 6 dental implants resulted in osteonecrosis and implant loss.24
Organ transplant medications
Immunosuppressive drugs, including cyclosporine A, azathioprine, sirolimus, and tacrolimus (FK506), are routinely used by organ transplant surgeons to prevent rejection of the transplanted organ.
A recent adult male rat study explored the impact of FK506 and cyclosporine on the physiological and immunological mechanisms.25 The administration of FK506 and rapamycin resulted in osteopenia. However, cyclosporine therapy only resulted in modest damage to the bone of the adult rat and minimal osteopenia. Other studies suggest that cyclosporine may have detrimental effects on bone healing and remodeling.26 Therefore, in dental implant patients, the extrapolation of this animal study may require further consideration for human organ transplant patients taking organ transplant medications.
Optimal osteoblast function is critical for implant osteointegration. In human studies, osteoblast function is impacted significantly by cyclosporine, FK506 and rapamycin.27 Molecular mechanisms for these medications focus on osteoblast apoptosis with FK506 and rapamycin; and can occur as soon as one day after cell challenge. Cyclosporin A did not produce the same osteogenic mechanisms with osteoblast. Therefore, these findings should be considered for implant treatment planning in patients with organ transplantation.
Post-transplantation bone disease is a frequent sequela of organ transplant patients taking sirolimus and FK506.28 Bone marrow density studies impacted after organ transplantation should be considered in dental implant treatment planning. Specific papers investigate the role of Tacrolimus, sirolimus and cyclosporine on the intracellular signaling pathways of the osteoblast.28 If osteoblast signaling are impacted, the interference to dental implant osteointegration has a major clinical impact on dental implant success. In addition, cyclosporine also compromises the host response and increases the risk of dental implant loss. Therefore, cautious dental implant treatment planning should take into consideration organ transplantation medications.
Medications affecting bone remodeling
Antacids
The antacids, including proton pump inhibitors, have been recently supported by other evidence leading to osteoporosis and an increased risk of dental implant failures.29 Antacids effectively change the acidity of the gastric mucosa and lead to potential decreases in calcium absorption. This decrease in calcium absorption appears to translate clinically as osteoporosis.
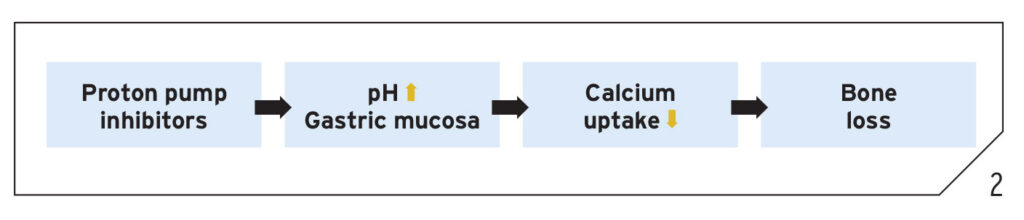
Over-the-counter medications such as H2 blockers (Tagamet and Pepcid) and proton pump inhibitors (Nexium, Prevacid, and Prilosec) appear to interfere with bone metabolism. Other over-the-counter antacids including Rolaids, Tums, and Maalox also interfere with bone metabolism. The pharmacological process appears to involve increasing gastrointestinal pH with potential impact on the gastric microbiome, resulting in long-term reduction in calcium absorption. In as little as one year, antacids can increase hip fractures by 44%.30 The longer a patient has been on antacids, the more significant the risk of hip fractures increases.30 Figure 2 illustrates the pharmacological mechanisms for reduced osseointegration by proton pump inhibitors.
Fig. 2
Current reviews also relate the osteoporotic condition of the bone to dental implant failures.31 Therefore, when treatment planning dental implant therapies, the clinician should consider the effect of the pharmacological use of antacids and proton pump inhibitors on increasing osteoporotic conditions and dental implant failures.
A meta-analysis investigating the effect of proton pump inhibitors on the risk of osteoporosis and hip fractures, reported that there is a recognized increased risk of both osteoporosis and fractures, which may be indirectly related to peri-implantitis and dental implant failure.32 However, the current evidence published in this meta-analysis did not identify direct evidence between dose response and duration of implant failures, osteoporosis, and the use of proton pump inhibitors.32 The dental clinician should be cognizant of the impact of the entire subclass of proton pump inhibitors on osteoporosis and the increased risk of dental implant failures. Antacids are now recognized to significantly increase the risk for osteoporosis as well as impact on the overall bone health of dental implants.
Selective serotonin reuptake inhibitors (SSRIs)
Another category of medications which may interfere with osseointegration is antidepressants, SSRIs. SSRI inhibits serotonin reuptake and increases the systemic extracellular levels of serotonin.33 These medications include Pristiq, Effexor, Celexa, Lexapro, Prozac, Symbyax, Paxil, Zoloft, among others. Antidepressants have been reported in over 5000 patients to result in osteoporosis and a twofold increase the risk of hip fractures.34
Several studies have documented the role of antidepressants in dental implant failure.35-40 Wu et al. reported that SSRIs are associated with dental implant failures.41 There is evidence that suggests abnormal bone healing and impaired osseointegration.42 Both osteoclasts and osteoblast functions are affected by the SSRIs, and contribute to greater risk of dental implant loss in these patients compared to non-users.42 Chrcanovic et al. reported an implant failure rate of 12.5% in SSRI users compared to 3.3% in non-users.43 Similarly, Wu et al. reported a 10.6% rate of implant loss in patients on SSRIs compared to 4.6% in patients not on SSRIs.41 Treatment with SSRIs is associated with increased failure risk of osteointegrated implants, which might suggest the need for careful surgical treatment planning for these patients.44-46 Figure 3 illustrates potential pharmacological mechanisms for reduced osseointegration in patients on SSRIs.
Fig. 3

Recent papers suggest that the different subclasses of antidepressants may have different effects on dental implants.31 In this recent study, patients on antidepressants were at higher risk for implant failure than implant patients who were not taking antidepressants. In addition, serotonin norepinephrine reuptake inhibitors (SNRI) and the tricyclic antidepressants (TCA) had an increasing risk of implant failure. This paper suggests that dental implant clinicians should regularly update the medications in the medical history of patients seeking dental implants in their practices. Furthermore, dental implant patients who initiate antidepressant medication should also be evaluated more frequently than patients not on these medications.
A systematic review and meta-analysis of the effect of antidepressants on dental implant failure concluded that SSRIs, as a collective group of three subtypes of antidepressants, may significantly increase the risk of dental implant failures both at the patient level and implant level.32 However, these three subtypes (SNRIs, SSRIs, and TCAs), should not be considered as final determinations of the effect on implant failures, further studies are needed. The clinician must use caution when planning dental implants in patients currently taking any form of antidepressants.
Bisphosphonates
Bisphosphonate medications, oral or intravenous, are prescribed for osteoporosis, osteopenia, and other conditions including Paget’s disease and certain antineoplastic conditions. Bisphosphonate medications are commonly used for osteoporosis in women and some men.
Osteoporosis is influenced by the following factors: growth factors, hormones, cytokines, and genetics. Bone formation and resorption are regulated by hormones and cytokines. Maintenance and renewal of bone health is a continuous cycle of bone resorption, migration, and formation. Medications that disrupt this balance can affect dental implant osteointegration.47-49
Amorim et al. evaluated differences in dental implant survival between current osteoporosis patients with the exclusion factors of oral bisphosphonates use.50 The dental implant differences between osteoporosis and non-osteoporotic patients are not recognized in this paper. However, these patients were not all taking bisphosphonates. The implication of the selected studies cited in this review strongly suggests that oral bisphosphonates and their interference with the homeostatic mechanisms of bone more directly alter dental implant status rather than the osteoporosis diagnosis.
Dental implant status may not be contingent upon osteoporosis in female patients, who are not taking antiresorptive medications. However, current studies have not explored more advanced osteoporotic patients with dental implants who are taking antiresorptive medication to reduce the risk of hip fractures.9, 51 Implant survival of severe osteoporotic patients, not on antiresorptive medication, has not been evaluated. Further investigations are necessary to elucidate differences in dental implants success in patients with early, moderate, and advanced stages of osteoporosis.
Bisphosphonates interfere with bone remodeling; healthy bone remodeling is necessary for implant integration.52 Bisphosphonates hinder osteoclast function, reducing bone resorption and healing.53 Bisphosphonates have been linked to dental implant complications like osteonecrosis and implant disintegration.54 Intravenous bisphosphonates further increase the risk of osteonecrosis and implant failure.54 Women older than 40 yrs on oral bisphosphonate treatment have a rate of late implant loss that is 2.5 times more, compared to women who are not on bisphosphonates.52 Thus, bisphosphonates can be a risk factor for peri-implantitis and implant failures.54-56
Medications favoring osteointegration
Antihypertensives
Antihypertensives are used to manage hypertension. Antihypertensives include calcium channel blockers, beta-blockers, thiazide diuretic, angiotensin receptor blocker, and angiotensin converting enzyme (ACE) inhibitors. Channel blockers, beta-blockers, and angiotensin converting enzyme (ACE) inhibitors are protective against bone fractures.57 Antihypertensives anabolically affect bone metabolism and can increase bone density in the mouth.58, 59 This may increase both osseointegration and implant survival. Wu et al. and Garcia-Denche et al. reported increased implant survival outcomes in patients on antihypertensives compared to patients not taking antihypertensives.60, 61 In a systematic review by Mishra et al., their findings reported implant survival rates to be 99.4% in patients on antihypertensives compared to 96.1% in patients not medicated.62 Additionally, this systematic review also reported increased implant stability quotient (ISQ) in antihypertensive-medicated patients compared to non-medicated patients.62
Thus, taking antihypertensive medication may benefit patients who have hypertension in terms of improved implant integration and implant survival. However, taking antihypertensives in a healthy person may cause hypotension and complications associated with syncope. In a healthy person, these complications may not compensate for the dental implant benefits, especially since the implant survival rates in healthy individuals are already very high.
Conclusion
These six main groups of medications adversely affecting bone health and dental implant osseointegration include the following: glucocorticoids, anti-tumor necrosis factor (TNF)-alpha drugs, organ transplant medication, antacids, selective serotonin reuptake inhibitors (SSRI), and bisphosphonates. Conversely, antihypertensive medications can improve bone quality and dental implant outcomes. Thus, the clinician needs to understand the systemic ramifications of these medications and their effects on the longevity of their dental implant restorations. More human studies are needed to further link these medications to peri-implantitis and dental implant failure. 
Oral Health welcomes this original article.
References
- Elani HW, Starr JR, Da Silva JD, Gallucci GO. Trends in dental implant use in the u.S., 1999-2016, and projections to 2026. J Dent Res. 2018;97(13):1424-30.
- Turner RT, Riggs BL, Spelsberg TC. Skeletal effects of estrogen. Endocr Rev. 1994;15(3):275-300.
- Eastell R, O’Neill TW, Hofbauer LC, et al. Postmenopausal osteoporosis. Nat Rev Dis Primers. 2016;2:16069.
- Dempster DW, Cosman F, Parisien M, et al. Anabolic actions of parathyroid hormone on bone. Endocr Rev. 1993;14(6):690-709.
- Swarthout JT, D’Alonzo RC, Selvamurugan N, Partridge NC. Parathyroid hormone-dependent signaling pathways regulating genes in bone cells. Gene. 2002;282(1-2):1-17.
- Chotiyarnwong P, McCloskey EV. Pathogenesis of glucocorticoid-induced osteoporosis and options for treatment. Nat Rev Endocrinol. 2020;16(8):437-47.
- Lian JB, Stein GS, Stein JL, van Wijnen AJ. Regulated expression of the bone-specific osteocalcin gene by vitamins and hormones. Vitam Horm. 1999;55:443-509.
- Umur E, Bulut SB, Yiğit P, et al. Exploring the role of hormones and cytokines in osteoporosis development. Biomedicines. 2024;12(8).
- Lemos CAA, de Oliveira AS, Faé DS, et al. Do dental implants placed in patients with osteoporosis have higher risks of failure and marginal bone loss compared to those in healthy patients? A systematic review with meta-analysis. Clin Oral Investig. 2023;27(6):2483-93.
- Romanos GE, Vaglica M, Sculean A. Drug-associated bone resorption with potential dental and implant implications. Periodontol 2000. 2022;90(1):236-46.
- Newton R. Molecular mechanisms of glucocorticoid action: What is important? Thorax. 2000;55(7):603-13.
- Dykman TR, Gluck OS, Murphy WA, et al. Evaluation of factors associated with glucocorticoid-induced osteopenia in patients with rheumatic diseases. Arthritis Rheum. 1985;28(4):361-8.
- Li X, Liang T, Dai B, et al. Excess glucocorticoids inhibit murine bone turnover via modulating the immunometabolism of the skeletal microenvironment. J Clin Invest. 2024;134(10).
- Henneicke H, Gasparini SJ, Brennan-Speranza TC, et al. Glucocorticoids and bone: Local effects and systemic implications. Trends Endocrinol Metab. 2014;25(4):197-211.
- Van Staa TP. The pathogenesis, epidemiology and management of glucocorticoid-induced osteoporosis. Calcif Tissue Int. 2006;79(3):129-37.
- Cain DW, Cidlowski JA. Immune regulation by glucocorticoids. Nat Rev Immunol. 2017;17(4):233-47.
- Flammer JR, Rogatsky I. Minireview: Glucocorticoids in autoimmunity: Unexpected targets and mechanisms. Mol Endocrinol. 2011;25(7):1075-86.
- Fu JH, Bashutski JD, Al-Hezaimi K, Wang HL. Statins, glucocorticoids, and nonsteroidal anti-inflammatory drugs: Their influence on implant healing. Implant Dent. 2012;21(5):362-7.
- Bencharit S, Reside GJ, Howard-Williams EL. Complex prosthodontic treatment with dental implants for a patient with polymyalgia rheumatica: A clinical report. Int J Oral Maxillofac Implants. 2010;25(6):1241-5.
- Rosenberg SA, Migliorati C, Romanos GE. Is medication-related osteonecrosis of the jaw associated with tumor necrosis factor-α inhibition? Oral Surg Oral Med Oral Pathol Oral Radiol. 2021;131(4):422-7.
- Monaco C, Nanchahal J, Taylor P, Feldmann M. Anti-tnf therapy: Past, present and future. Int Immunol. 2015;27(1):55-62.
- Tracey D, Klareskog L, Sasso EH, et al. Tumor necrosis factor antagonist mechanisms of action: A comprehensive review. Pharmacol Ther. 2008;117(2):244-79.
- Anti-inflammatory medication linked to osteonecrosis of the jaw. Steiner bio. (n.D.). Https://www.Steinerbio.Com/anti-inflammatory-medication-linked-to-osteonecrosis-of-the-jaw. January 24, 2020.
- Cassoni A, Romeo U, Terenzi V, et al. Adalimumab: Another medication related to osteonecrosis of the jaws? Case Rep Dent. 2016;2016:2856926.
- Rubert M, Montero M, Guede D, et al. Sirolimus and tacrolimus rather than cyclosporine a cause bone loss in healthy adult male rats. Bone Rep. 2015;2:74-81.
- Tedesco D, Haragsim L. Cyclosporine: A review. J Transplant. 2012;2012:230386.
- Martín-Fernández M, Rubert M, Montero M, de la Piedra C. Effects of cyclosporine, tacrolimus, and rapamycin on osteoblasts. Transplant Proc. 2017;49(9):2219-24.
- Krocker D, Perka C, Tuischer J, et al. Effects of tacrolimus, cyclosporin a and sirolimus on mg63 cells. Transpl Int. 2006;19(7):563-9.
- Kopic S, Geibel JP. Gastric acid, calcium absorption, and their impact on bone health. Physiol Rev. 2013;93(1):189-268.
- Yang YX, Lewis JD, Epstein S, Metz DC. Long-term proton pump inhibitor therapy and risk of hip fracture. Jama. 2006;296(24):2947-53.
- D’Ambrosio F, Amato A, Chiacchio A, et al. Do systemic diseases and medications influence dental implant osseointegration and dental implant health? An umbrella review. Dent J (Basel). 2023;11(6).
- Chappuis V, Avila-Ortiz G, Araújo MG, Monje A. Medication-related dental implant failure: Systematic review and meta-analysis. Clin Oral Implants Res. 2018;29 Suppl 16:55-68.
- Tsapakis E, Gamie Z, Tran G, al. e. The adverse skeletal effects of selective serotonin reuptake inhibitors. Eur psychiatry. 2010; 27: 156-169.
- Richards JB, Papaioannou A, Adachi JD, et al. Effect of selective serotonin reuptake inhibitors on the risk of fracture. Arch Intern Med. 2007;167(2):188-94.
- Silva CCG, Dos Santos MS, Monteiro J, et al. Is there an association between the use of antidepressants and complications involving dental implants? A systematic review and meta-analysis. Int J Oral Maxillofac Surg. 2021;50(1):96-103.
- Harutyunyan L, Lieuw K, Yang B, et al. The effect of antidepressants on dental implant failure: A systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2024;39(5):665-73.
- Shariff JA, Gurpegui Abud D, Bhave MB, Tarnow DP. Selective serotonin reuptake inhibitors and dental implant failure: A systematic review and meta-analysis. J Oral Implantol. 2023;49(4):436-43.
- Hakam AE, Vila G, Duarte PM, et al. Effects of different antidepressant classes on dental implant failure: A retrospective clinical study. J Periodontol. 2021;92(2):196-204.
- Block MS, Mercante D. Selective serotonin reuptake inhibitors may increase implant failure. J Oral Maxillofac Surg. 2025;83(5):585-91.
- Kotsailidi EA, Gagnon C, Johnson L, et al. Association of selective serotonin reuptake inhibitor use with marginal bone level changes around osseointegrated dental implants: A retrospective study. J Periodontol. 2023;94(8):1008-17.
- Wu X, Al-Abedalla K, Rastikerdar E, et al. Selective serotonin reuptake inhibitors and the risk of osseointegrated implant failure: A cohort study. J Dent Res. 2014;93(11):1054-61.
- Gupta B, Acharya A, Pelekos G, et al. Selective serotonin reuptake inhibitors and dental implant failure-a significant concern in elders? Gerodontology. 2017;34(4):505-7.
- Chrcanovic BR, Kisch J, Albrektsson T, Wennerberg A. Is the intake of selective serotonin reuptake inhibitors associated with an increased risk of dental implant failure? Int J Oral Maxillofac Surg. 2017;46(6):782-8.
- Battaglino R, Fu J, Späte U, et al. Serotonin regulates osteoclast differentiation through its transporter. J Bone Miner Res. 2004;19(9):1420-31.
- Wu X, Al-Abedalla K, Abi-Nader S, et al. Proton pump inhibitors and the risk of osseointegrated dental implant failure: A cohort study. Clinical Implant Dentistry and Related Research. 2017;19(2):222-32.
- Winnett B, Tenenbaum HC, Ganss B, Jokstad A. Perioperative use of non-steroidal anti-inflammatory drugs might impair dental implant osseointegration. Clin Oral Implants Res. 2016;27(2):e1-7.
- Sulaiman n, fadhul f, chrcanovic br. Bisphosphonates and dental implants: A systematic review and meta-analysis. Materials. 2023; 16(18):6078. Https://doi.Org/10.3390/ma16186078.
- Fiorillo L, Cicciù M, Tözüm TF, et al. Impact of bisphosphonate drugs on dental implant healing and peri-implant hard and soft tissues: A systematic review. BMC Oral Health. 2022;22(1):291.
- Rebelo, c.G.; fernandes, j.C.H.; bernardo, n.; couto, p.; fernandes, g.V.O. Bisphosphonates and their influence on the implant failure: A systematic review. Appl. Sci. 2023, 13, 3496. Https://doi.Org/10.3390/app13063496.
- Amorim MA, Takayama L, Jorgetti V, Pereira RM. Comparative study of axial and femoral bone mineral density and parameters of mandibular bone quality in patients receiving dental implants. Osteoporos Int. 2007;18(5):703-9.
- Shibli JA, Naddeo V, Cotrim KC, et al. Osteoporosis’ effects on dental implants osseointegration and survival rate: A systematic review of clinical studies. Quintessence Int. 2025;56(3):206-16.
- Yip, y.K., and dennis tarnow (journal of clinical periodontology, 2012, volume 39, page 408.
- Russell RG, Xia Z, Dunford JE, et al. Bisphosphonates: An update on mechanisms of action and how these relate to clinical efficacy. Ann N Y Acad Sci. 2007;1117:209-57.
- de-Freitas NR, Lima LB, de-Moura MB, et al. Bisphosphonate treatment and dental implants: A systematic review. Med Oral Patol Oral Cir Bucal. 2016;21(5):e644-51.
- Ting M, Suzuki JB. Clinical effects of antiresorptive medications on dental implant survival and implant-related osteonecrosis of the jaw. J int clin dent. 2022;3(2):E001.
- Ting M, Huynh BH, Woldu HG, et al. Clinical impact on dental implant survival in patients taking antiresorptive medications: A systematic review and meta-analysis. J Oral Implantol. 2023;49(6):599-615.
- Rejnmark L, Vestergaard P, Mosekilde L. Treatment with beta-blockers, ace inhibitors, and calcium-channel blockers is associated with a reduced fracture risk: A nationwide case-control study. J Hypertens. 2006;24(3):581-9.
- Takeda S, Elefteriou F, Levasseur R, et al. Leptin regulates bone formation via the sympathetic nervous system. Cell. 2002;111(3):305-17.
- Togari A, Arai M. Pharmacological topics of bone metabolism: The physiological function of the sympathetic nervous system in modulating bone resorption. J Pharmacol Sci. 2008;106(4):542-6.
- Wu X, Al-Abedalla K, Eimar H, al. e. Antihypertensive medications and the survival rate of osseointegrated dental implants: A cohort study. Clin. Implant. Dent. Relat. Res. 2016, 18, 1171–1182.
- García-Denche JT, Wu X, Martinez PP, et al. Membranes over the lateral window in sinus augmentation procedures: A two-arm and split-mouth randomized clinical trials. J Clin Periodontol. 2013;40(11):1043-51.
- Mishra SK, Sonnahalli NK, Chowdhary R. Do antihypertensive medications have an effect on dental implants? A systematic review. Oral Maxillofac Surg. 2024;28(2):459-68.
About the authors

Miriam Ting, DMD (Temple University, magna cum laude), BDS (Singapore), Cert. Advanced Periodontology and MS (Craniofacial Biology) at USC. Diplomate, American Board of Periodontology and ICOI. Dr. Ting is founder and director, Think Dental Learning Institute and Magnifico Oral Health Foundation and practises at Think Oral Implants and Periodontics in Paoli, PA.

Dr. Jon B. Suzuki, Clinical Professor, University of Maryland, Baltimore, MD, USA. Clinical Professor, University of , Seattle, WA, USA. Clinical Professor, Nova-Southeastern University, Ft. Lauderdale, FL USA. Professor Emeritus, Temple University, Philadelphia, PA, USA.