


A dental implant is defined as a prosthetic device made of alloplastic material(s) implanted into the oral tissues beneath the mucosal and/or periosteal layer and on or within the bone to provide retention and support for a fixed or removable dental prosthesis, a substance that is placed into and/or on the jaw bone to support a fixed or removable dental prosthesis. Dental implants have revolutionized restorative dentistry. They offer permanent replacement to loose and missing teeth and can be an alternative to wearing dentures and rebuilding confidence with a functional and secure smile.
Recent standards1 in implantology are intended to provide prosthetic restorations with the finest esthetic and functional results. Several parameters have been suggested to achieve benchmark results: adequate bone height, width and sagittal projection, adequate soft-tissue quantity and quality, preservation of buccal sulcus, and adequate papillae and gingival contour.2 Solutions to inadequate ridge height include the use of short implants,3 vertical ridge augmentation procedures,4,5 or cantilever prostheses.6 Although having a comparable short-term survival rate, some authors state that the long-term performance of short implants is less understood, especially in the posterior maxilla with lower bone density.7 Vertical augmentation procedures increase patient injury, and the outcome is less predictable, especially in the posterior mandible. Cantilever prostheses might incur higher rates of prosthetic complications such as abutment loosening, denture fracture, and implant failure.
Due to the less predictable long-term prognosis associated with the above-mentioned procedures, the “All-on-Four” technique was proposed for the rehabilitation in edentulous jaws. Although the use of only four implants for a complete fixed rehabilitation of the maxilla has been supported by clinical studies at short period,8,9,10 it has been suggested that using a larger number of implants (around 6) for prosthetic treatment of the edentulous maxilla may be beneficial as the stresses on the majority of the implants were lower in the all-on-six planning in comparison to the all-on-four planning.
The “all-on-six” treatment concept was developed to maximize the use of available remnant bone in jaws, allow immediate function, and avoid regenerative procedures that increase the treatment costs and patient morbidity, as well as the complications inherent to these procedures.11
Brånemark’s original surgical protocol advocated the placement of four implant fixtures for the restoration of a resorbed maxillae and six implant fixtures on mandibles that demonstrated minimal-to-moderate resorption. 12
The implant-supported fixed restoration (FP-3) restoration appears to replace the natural teeth crowns and a portion of the soft tissue. Basically, two approaches for an FP-3 prosthesis exist: a hybrid restoration of denture teeth, acrylic and metal substructure, or a porcelain-metal restoration. 13
The primary factor that determines the restoration type is the amount of interarch space, transition line, and smile line. The challenge today is not only to prove functionality but also to develop simple and cost-effective protocols. The purpose of this paper is to report a case of full-mouth prosthetic rehabilitation on six endosseous implants in maxilla and 4 implants in mandible loaded following the standard procedure.
Case Report
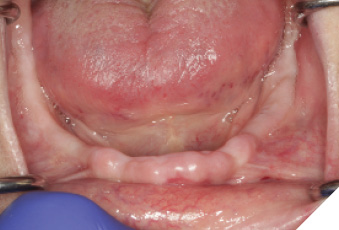
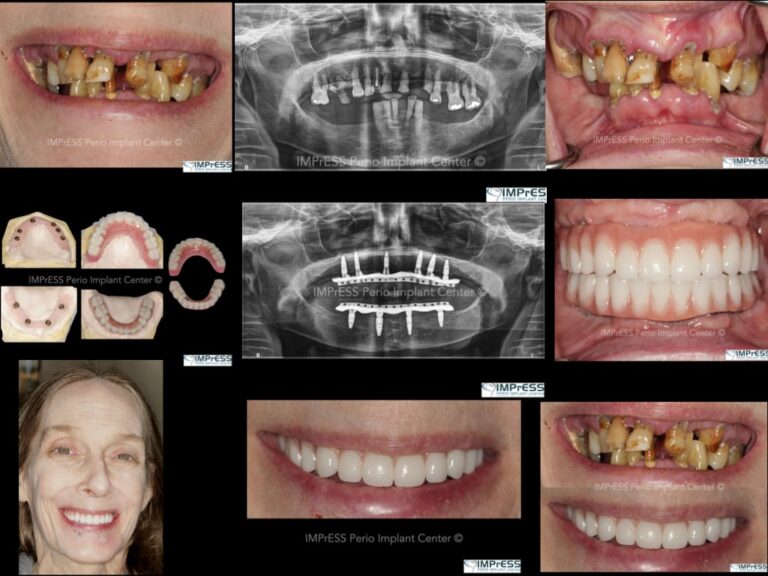
A 60-year-old female patient has been referred to our clinic with severely compromised dentition, advanced periodontitis and unsalvageable teeth (Fig. 1, 2, 3, 4). The patient was unhappy with the esthetics and did not want a removable prosthesis. After careful evaluation, it was decided to insert six implants in the maxillary and four implants in the mandibular arch. Due to presence of acute periodontal infection, full mouth clearance was done followed by delivery of immediate complete maxillary and mandibular dentures. Multiple soft relines were necessary to ensure patient’s comfort for the next three months.
Fig. 1

Fig. 2

Fig. 3

Fig. 4
Investigations
Dual computed tomography CBCT with radiographic markers were obtained from maxillary and mandibular edentulous ridges three months after removal of teeth.
Conventional dentures allowed us to determine the vertical dimension of occlusion, assess patient’s esthetics, phonetics, teeth set-up and facial tissue support.
One of the most crucial steps to plan and execute the surgical plan is to assess the lip support, smile line and location of the prosthetic transition line. In this case, the smile line was high and the transition line was well noticeable. Therefore, bone reduction was necessary to move the prosthetic transition line apically and gain space for the titanium bar, teeth and acrylic or ceramic foundation. Minimum of 16 mm space is required from the implant platform to the incisal edge. Digitally planned bone reduction guide allowed for predictable and safe bone removal. In the meantime, the reference point to determine the location of implant platform is preplanned based on digital information combined from CBCT and the immediate complete dentures.
Surgical phase
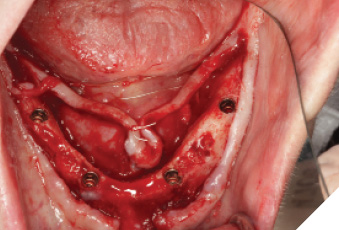
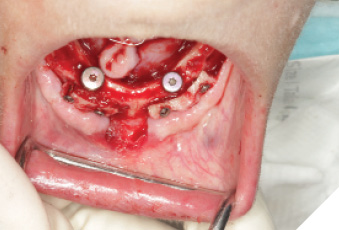
The surgery was performed under local anesthesia with articaine 4% with epinephrin 1:200K for local infiltration and lidocaine 2% with epinephrin 1:100K for regional nerve block. A total of 10 implants were placed for mandibulular (Fig. 4, 5, 6, 7) and maxillary (Fig. 8, 9, 10, 11) rehabilitation with the application of bone supported surgical guide fixated with three anchoring pins in each arch. Implant stability was sufficient (35 N/cm measured with a torque spring) for all 10 implants. One stage surgery was performed. Bone reduction was necessary to flatten the ridge, to gain more room for prosthetic components and to transfer the transition line to the ideal position.
Fig. 5

Fig. 6
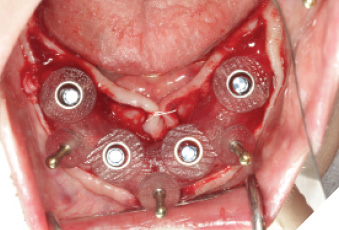
Fig. 7
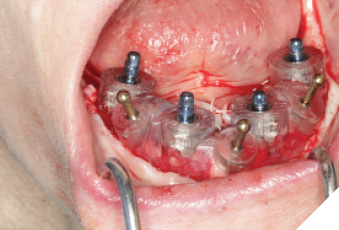
Fig. 8

Fig. 9
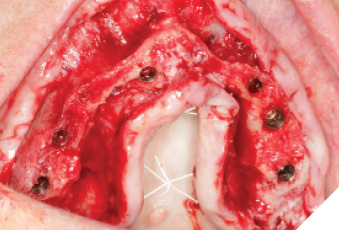
Fig. 10
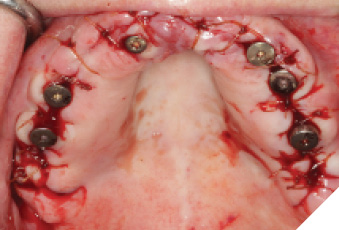
Fig. 11
The autogenous bone removed from the crestal part of the ridge was recycled and fixated with bone fixation screws according to the Khoury split bone block technique to augment the moderately atrophied mandibular ridge and to enhance the available bone for long term implant longevity (Fig. 12). Healing abutments were hand torqued, flap was closed and patient was provided with postoperative instructions.
Fig. 12
Prosthetic Phase
Three months following the implants surgery, the healing abutments were removed. Implant osseointegration was tested. IOS with scan bodies or an analogue impression with implant copings can be utilized at this stage. For this specific case, an implant level impression was taken with open tray technique to prepare primary models. The primary impressions were sent to lab to select the correct screw retained abutments (SRAs) in terms of diameter and height.
Utilizing the primary impression, our lab fabricated the Implant verification jig, Implant custom tray and bite blocks. SRA(s) were torqued to 35Ncm. Abutment level impression with splinted open tray impression copings was obtained. With the implant verification jig provided we ensure passivity. We recommend taking radiographs to confirm the perfect fit of the jig. If the jig does not fit passively, it is cut and re-luted. A pickup wash impression with the implant custom tray provided follows. This will be considered as the verified final impression. (Custom tray provided will capture landmarks needed). With the verified implant impression the final verified model or master cast (Fig. 13 & 14) is fabricated as well as a wax try-in (Fig 15). This can be used by the lab to allow for a PMMA prototype. We were able to confirm the overall shape, length, esthetics and to check occlusion (Fig. 16, 17, 18, 19, 20, 21, 22). Any occlusal adjustments needed can be done directly on the PMMA prototype. Once the bite is adjusted, take the bite registration on top of the prototype, and return everything back to your lab for remount, including the PMMA. IOS users can do a copy scan protocol of the PMMA prototype, send your lab the STL file and keep PMMA prototype in the mouth. For this digital workflow, second set of the implant parts will be needed. Only once the accuracy of the PMMA prototype is confirmed, the lab proceeds to the final zirconia restoration.
 Fig. 13
Fig. 13

Fig. 14

Fig. 15

Fig. 16

Fig. 17

Fig. 18

Fig. 19

Fig. 20

Fig. 21

Fig. 22
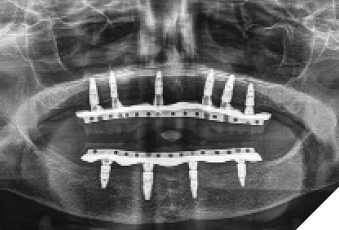
Fig. 23
Oral Health welcomes this original article.
References
- Ferro KJ. The Glossary of Prosthodontic Terms: Ninth Edition. J Prosthet Dent. 2017;117(5S):e1–e105. [PubMed] [Google Scholar]
- Guerrero C, Lopez P, Figueroa F. Three-dimensional alveolar distraction osteogenesis. In: Bell W, Guerrero C, editors. Distraction Osteogenesis of the Facial Skeleton. 1st ed. Hamilton (Canada): BC Decker; 2007. pp. 457–93. [Google Scholar]
- Esposito M, Grusovin MG, Coulthard P, Worthington HV. The efficacy of various bone augmentation procedures for dental implants: A Cochrane systematic review of randomized controlled clinical trials. Int J Oral Maxillofac Implants. 2006;21:696–710. [PubMed] [Google Scholar]
- Sorní M, Guarinós J, García O, Peñarrocha M. Implant rehabilitation of the atrophic upper jaw: A review of the literature since 1999. Med Oral Patol Oral Cir Bucal. 2005;10(Suppl 1):E45–56. [PubMed] [Google Scholar]
- Maestre-Ferrín L, Boronat-López A, Peñarrocha-Diago M, Peñarrocha-Diago M. Augmentation procedures for deficient edentulous ridges, using onlay autologous grafts: An update. Med Oral Patol Oral Cir Bucal. 2009;14:e402–7. [PubMed] [Google Scholar]
- Chaushu G, Mardinger O, Peleg M, Ghelfan O, Nissan J. Analysis of complications following augmentation with cancellous block allografts. J Periodontol. 2010;81:1759– 64. [PubMed] [Google Scholar]
- Hashemi HM. Neurosensory function following mandibular nerve lateralization for placement of implants. Int J Oral Maxillofac Surg. 2010;39:452–6. [PubMed] [Google Scholar]
- Lazari PC, Sotto-Maior BS, Rocha EP, de Villa Camargos G, Del Bel Cury AA. Influence of the veneer-framework interface on the mechanical behavior of ceramic veneers: A nonlinear finite element analysis. J Prosthet Dent. 2014;112:857–63. [PubMed] [Google Scholar]
- Hasan I, Bourauel C, Mundt T, Heinemann F. Biomechanics and load resistance of short dental implants: A review of the literature. ISRN Dent. 2013;2013:424592. [PMC free article] [PubMed] [Google Scholar]
- Corbella S, Taschieri S, Del Fabbro M. Long-term outcomes for the treatment of atrophic posterior maxilla: A systematic review of literature. Clin Implant Dent Relat Res. 2015;17:120–32. [PubMed] [Google Scholar]
- Maló P, Rangert B, Dvärsäter L. Immediate function of brånemark implants in the esthetic zone: A retrospective clinical study with 6 months to 4 years of follow-up. Clin Implant Dent Relat Res. 2000;2:138–46. [PubMed] [Google Scholar]
- Brånemark PI, Engstrand P, Ohrnell LO, Gröndahl K, Nilsson P, Hagberg K, et al. Brånemark novum: A new treatment concept for rehabilitation of the edentulous mandible. Preliminary results from a prospective clinical follow-up study. Clin Implant Dent Relat Res. 1999;1:2–16. [PubMed] [Google Scholar]
- Bodine RL. Prosthodontic essentials and an evaluation of the mandibular subperiosteal implant denture. J Am Dent Assoc. 1955;51:654–64. [PubMed] [Google Scholar]
About the Author

Dr. Mehdi Noroozi is a board-certified periodontist who provides the full scope of surgical periodontal and dental implant therapy. Dr. Noroozi has a special interest in esthetic and reconstructive periodontics and implantology. In addition to private practice, Dr. Noroozi is a clinical assistant professor in the department of graduate periodontics at the University of British Columbia where he is involved in didactic and clinical teaching of periodontics at post-graduate level. Dr. Noroozi has lectured nationally and internationally and published on various topics related to periodontics and implantology. He can be reached at info@implantperiospecialist.com IMPrESS Perio Implant Center, Vancouver, British Columbia, Canada.