
Evaluating restorability before endodontic treatment: A critical step in treatment planning
Before initiating endodontic treatment, assessing the restorability of a tooth is crucial to ensure long-term success. While root canal therapy can effectively resolve pulpal infections, it is only worthwhile if the tooth can be predictably restored and functionally maintained. Failing to evaluate restorability beforehand may lead to situations where a tooth is deemed non-restorable after endodontic therapy, resulting in wasted time, cost, and effort for both the dentist and the patient. A thorough assessment helps determine whether the tooth has sufficient structural integrity to support a definitive restoration and withstand occlusal forces over time.
Several key guidelines should be followed when determining a tooth’s restorability. First, adequate remaining tooth structure is essential—ideally, at least 2 mm of ferrule above the crown margin to provide resistance against fracture and ensure long-term stability.1,8 The presence and condition of the remaining coronal and radicular tooth structure should be evaluated, considering factors such as deep caries, fractures, or excessive loss of dentin. Additionally, periodontal health plays a significant role; teeth with significant bone loss, furcation involvement, mobility, or deep probing depths may have a poor long-term prognosis even if the endodontic treatment is successful. Lastly, the ability to achieve a predictable, well-sealed restoration, whether through a post-and-core buildup or full-coverage crown, is essential for preventing reinfection and structural failure.3,4
By carefully evaluating these factors before committing a tooth to endodontic treatment, clinicians can make more informed decisions about whether to proceed with root canal therapy or consider alternative options such as extraction and implant placement. Taking the time to assess restorability helps enhance treatment outcomes, reduces unnecessary procedures, and ultimately leads to better patient satisfaction and long-term success.
To use a post or not? Best post material options
The decision to place a post after endodontic treatment depends on the amount of remaining tooth structure. Posts do not reinforce teeth; instead, they serve as retention devices for the core buildup when insufficient coronal tooth structure remains. If a tooth has sufficient coronal dentin and a strong ferrule effect (at least 2 mm of circumferential dentin), a post is generally unnecessary.1,2,8 However, if the remaining structure is compromised, a post may be required to retain the core. The key is to minimize unnecessary removal of radicular dentin, as excessive preparation can weaken the root and increase the risk of vertical root fractures.
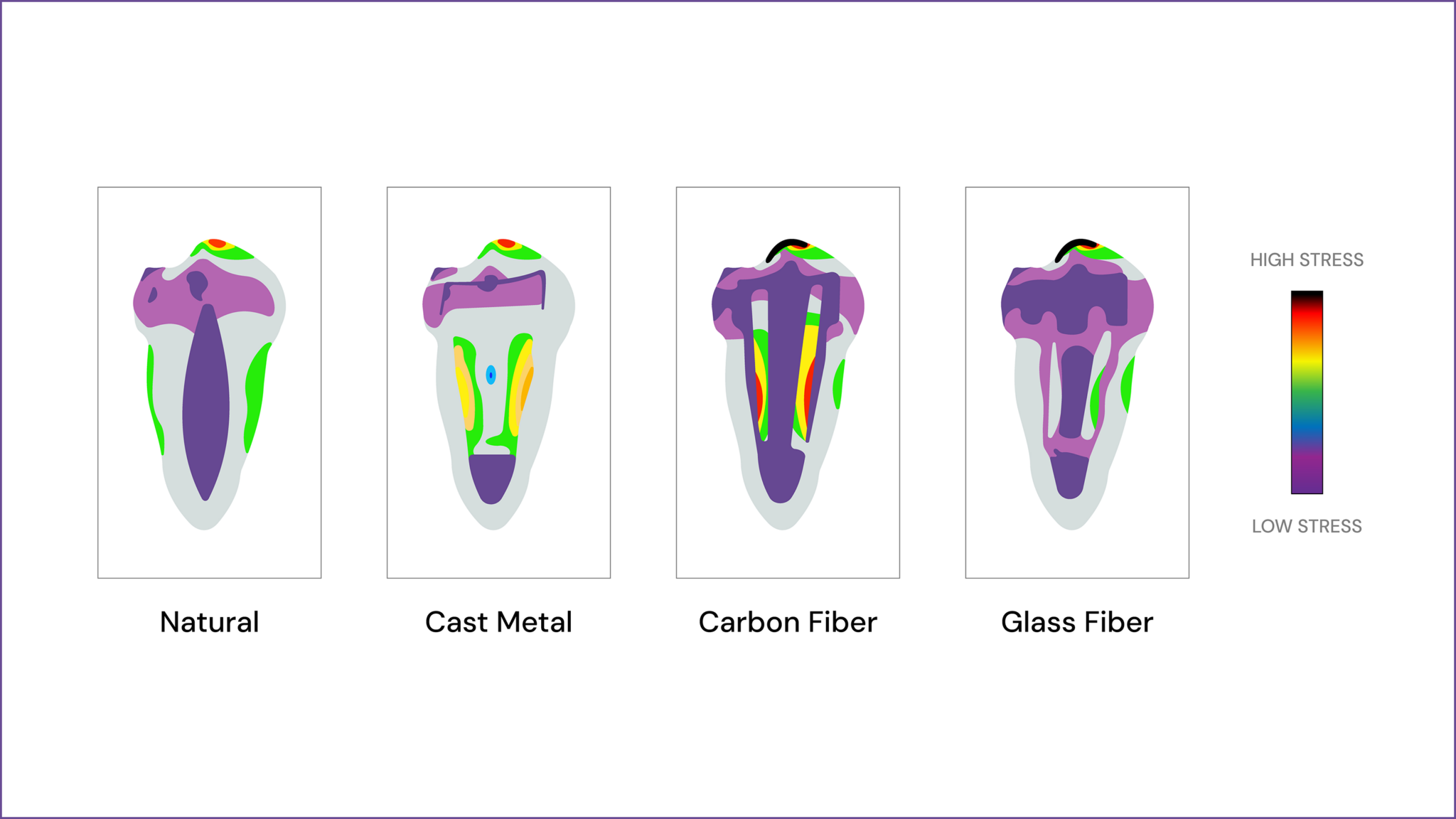
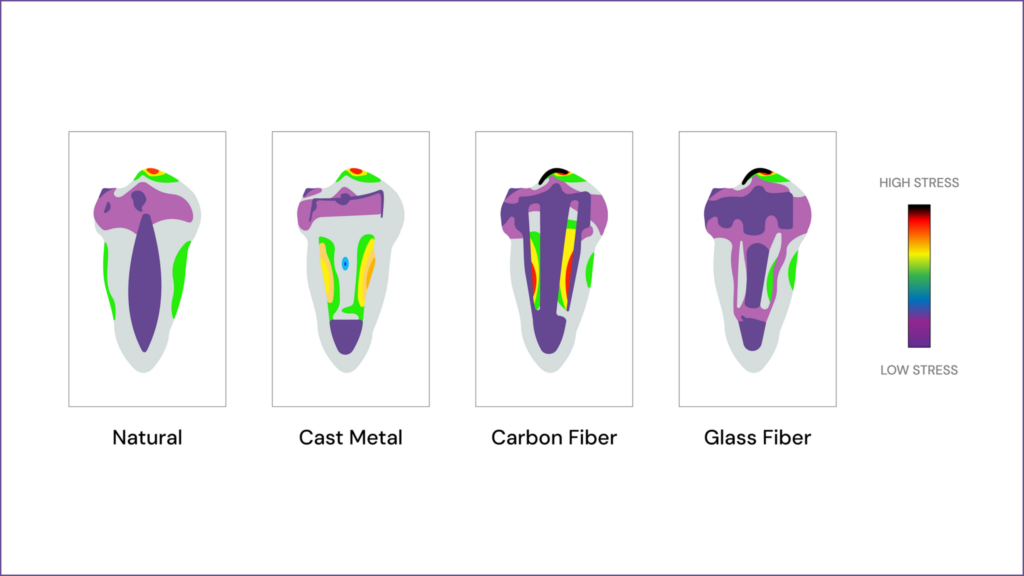
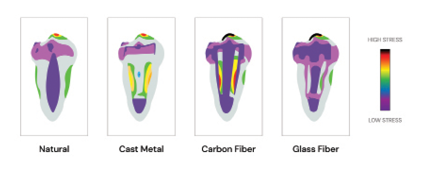
When a post is necessary, material selection plays a crucial role in long-term success. Fiber posts (composed of glass or carbon fiber in a resin matrix) are the preferred choice in most cases because they have a modulus of elasticity similar to dentin, reducing stress concentration and the risk of root fractures. They also bond well with composite core materials, improving retention. Metal posts (such as titanium or stainless steel) offer high strength but have a higher risk of root fracture due to their stiffness and can cause stress points inside the canal. Cast-metal posts and cores are still used in certain cases where a custom fit is necessary, but they are more technique-sensitive and require multiple appointments. Zirconia posts provide excellent esthetics, especially for anterior teeth, but they are highly rigid and cannot bond as effectively to composite cores, increasing the risk of debonding or fracture.
Overall, the best approach is to preserve as much dentin as possible, avoid unnecessary post placement, and, when required, choose fiber posts due to their superior biomechanical compatibility with dentin. Proper adhesive bonding techniques further enhance retention and longevity, ultimately ensuring the functional and structural success of the restored endodontically treated tooth.
Fig. 1A
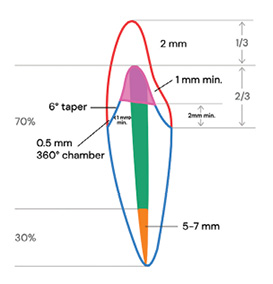
Fig. 1B
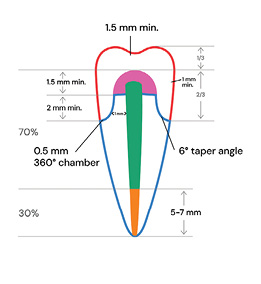
Fig. 2
The importance of sealing the gutta percha with the core material
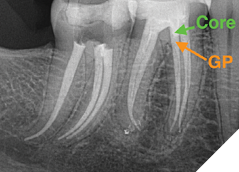
A critical step in the restorative process following endodontic treatment is ensuring a well-sealed interface between the gutta percha and the core material. A poor seal may allow bacterial leakage into the canal system, leading to potential reinfection and eventual treatment failure of the endodontic treatment, especially if the patient is delaying the placement of a crown (due to financial or motivation restraints).
When placing the core, it is essential to ensure that the coronal gutta percha is adequately sealed with a dense and well-adapted core material to prevent microleakage.3,4,5 Bonded composite or resin-based core materials are ideal for achieving a strong seal, as they offer high adhesion and minimize the risk of voids. Additionally, excessive removal of gutta percha should be avoided to preserve apical integrity while ensuring a solid foundation for the final restoration. By prioritizing a tight and secure seal, clinicians can enhance the long-term prognosis of the root canal-treated tooth and reduce the risk of endodontic failure.
Fig. 3
Furthermore, properly cleaning the endodontic cement before placing the core material is crucial for achieving a strong bond and preventing microleakage. Residual sealer may interfere with the curing process and adhesion of the core material, compromising the integrity of the restoration. If not removed completely, it can create a weak interface between the core material and dentin, leading to bonding failure over time. Thoroughly cleaning the post space with alcohol is an effective way to eliminate residual cement and ensure optimal adhesion. Neglecting this step increases the risk of poor adaptation, leakage, and potential long-term failure of the restoration.
The importance of a well-sealed and high-quality temporary crown
In the instance of a two-appointment crown scenario, the quality of the temporary crown plays a critical role in the overall success of the restoration. A poorly fitting or inadequately sealed temporary crown can lead to bacterial contamination, microleakage, and even re-infection of the root canal system, jeopardizing the long-term prognosis of the treated tooth.2,4,7 Proper marginal adaptation is crucial to prevent exposure to oral fluids, which can lead to bacterial infiltration and subsequent failure of the endodontic treatment. The temporary crown must also protect the prepared tooth structure, preventing fractures or excessive occlusal forces that could further weaken the tooth before the final restoration is placed.
Beyond sealing and protection, the temporary crown should also maintain occlusal function and proper interproximal contacts to prevent shifting of adjacent or opposing teeth. If the occlusion is left unbalanced, unwanted tooth movement can occur, making the final restoration more challenging to seat correctly. In high-risk patients, such as those with parafunctional habits or heavy occlusal forces, the temporary must be carefully adjusted to minimize stress on the remaining tooth structure. Additionally, esthetics should be considered, particularly for anterior teeth, where a properly contoured temporary restoration helps maintain gingival health and patient satisfaction. A high-quality temporary ensures that the final restoration will seat properly, maintain long-term success, and reduce complications such as open margins or occlusal imbalances that could lead to crown failure.
Occlusal management once the endodontically treated tooth is properly restored.
Once the tooth is successfully restored, proper occlusal management is critical for longevity. For anterior teeth, they should ideally have light, evenly distributed contact in centric relation, and provide adequate guidance during lateral movements,1,4 ensuring posterior disclusion through proper canine guidance or group function, depending on the case. In posterior teeth, occlusion should allow for even stable contacts in centric occlusion with no interferences in lateral and protrusive movements.5,6 In cases of heavy bruxers or parafunctional habits, special considerations are necessary, such as adjusting occlusion to distribute forces evenly, using materials that resist wear, and prescribing a protective occlusal splint to prevent excessive loading. When multiple teeth are missing, occlusal stability must be re-established through proper prosthetic planning, ensuring that forces are well-distributed and avoiding overloading of individual teeth, which could lead to fractures or restoration failure. By respecting these occlusion principles, clinicians can significantly improve the longevity and function of endodontically treated teeth while minimizing risks of structural failure.
When selecting a crown material after endodontic treatment, clinicians must consider esthetics, strength, longevity, and occlusal forces. Zirconia crowns are highly durable and fracture-resistant, making them ideal for posterior teeth or bruxers; however, they are less translucent than other materials and may appear opaque. Lithium disilicate (IPS e.max) crowns offer excellent esthetics and are strong enough for anterior and premolar restorations, but they may not be as resilient under heavy occlusal forces in molar regions without adequate support. Porcelain-fused-to-metal (PFM) crowns combine a strong metal substructure with an esthetic porcelain layer, providing good strength and longevity, though they may suffer from chipping or esthetic concerns if the metal margin becomes exposed. Full gold crowns remain the gold standard for strength and wear compatibility, particularly in heavy bruxers, but their metallic appearance makes them less desirable for many patients. Composite or resin-based crowns are an economical option but are significantly weaker and more prone to wear and staining, making them less ideal for long-term restorations. Ultimately, the choice of material should align with the patient’s functional and esthetic needs while ensuring durability and proper occlusal function for the long-term success of the restored tooth.
Conclusion
A successful endodontic outcome hinges not only on the quality of root canal treatment but also on the prompt and meticulous execution of the restorative phase. The endodontic-restorative continuum emphasizes the critical role of immediate and high-quality restoration in preventing reinfection and structural failure. Coronal microleakage, bacterial contamination, and delayed restorations can all compromise long-term success, making close collaboration between endodontists and restorative dentists essential. Evaluating restorability before treatment, selecting appropriate post-and-core materials, ensuring a well-sealed restoration, and managing occlusion effectively all contribute to the longevity of the treated tooth. Ultimately, endodontic treatment is only truly complete when a properly sealed and durable restoration is in place, safeguarding the tooth’s function and longevity. 
Oral Health welcomes this original article.
References
- D’Arcangelo C, De Angelis F, Vadini M, Zazzeroni S, Ciampoli C, D’Amario M. In vitro fracture resistance and deflection of pulpless teeth restored with fiber posts and prepared for veneers. J Endod. 2008 Jul;34(7):838-41.
- Hajizadeh H, Namazikhah MS, Moghaddas MJ, Ghavamnasiri M, Majidinia S. Effect of posts on the fracture resistance of load-cycled endodontically-treated premolars restored with direct composite resin. J Contemp Dent Pract. 2009 May 1;10(3):10-7.
- Salameh Z, Ounsi F, Aboushelib MN, Sadig W, Ferrari M. Fracture resistance and failure patterns of endodontically treated mandibular molars with and without glass fiber post in combination with a zirconia-ceramic crown. J Dent. 2008;36(7):513-519.
- Maccari PC, Conceicao EN, Nunes MF. Fracture resistance of endodontically treated teeth restored with three different prefabricated esthetic posts. J Esthet Resor Dent 2003;15:25-31.
- Schmitter M, Huy C, Ohlmann B, Gabbert O, Gilde H, Rammelsberg P. Fracture resistance of upper and lower incisors restored with glass fiber reinforced posts. J Endod April 2006;32(4):328-30.
- Goncalves LA, Vansan LP, Paulino SM, Neto MDS. Fracture resistance of weakened roots restored with a transilluminating post and adhesive restorative materials. J Prosthet Dent Nov 2006;96(5):339-344.
- Hayashi M, Takahashi Y, Imazoto S, Shigeyuki E. Fracture resistance of pulpless teeth restored with post-cores and crowns. Dentr Mat 2006;22:477-485.
- Ferrari M, Cagidiaco MC, Grandini M, De Sanctis M, Gorraci C. Post placement affects survival of endodontically treated premolars.
J Dent Res 2007;86(8):729-734.
About the authors

Dr. Mazen Dagher is the founder and chief education officer of Dagher Institute, a learning center for professionals who wish to advance their skills in implant dentistry, prosthodontics, endodontics, and periodontal surgery. Dr Dagher also founded the Hawkesbury Dental Centre in 1999, a top-tier group practice.

Dr. Gary Glassman lectures globally on endodontics, is on staff at the University of Toronto, Faculty of Dentistry in the graduate department of endodontics. He maintains a private practice, Endodontic Specialists in Toronto, Ontario, Canada. His personal/professional website is www.drgaryglassman.com, and his office website is www.rootcanals.ca.