


The endodontic restorative continuum
Timely and effective restoration can mean the difference between success and failure of a previously root canal treated tooth. Even after the root canal treatment (RCT) is completed, and the patient is out of pain, the clock continues to tick. Tooth contamination can start from a few hours to a few days after the process, so the restorative dentist’s quick response is vital to endodontic treatment success.1
In endodontics, many steps are involved in achieving endodontic success. From diagnosis and treatment planning to identifying the patients’ individual needs, to the determination of other clinical variables and risk factors, procedural success is affected and balanced with other details such as the dentist’s experience, skill, and comfort levels.2
While preventing and/or eliminating apical periodontitis (infection) from the root canal system is the objective of endodontic treatment and has a high degree of success, the ultimate outcome depends on patient compliance, and the technical skills and technologies employed by the restoring dentist.2
Bacteria vs. “The Seal”
All the education, talent, and skill in the world possessed by the clinician performing the root canal procedure will not be productive if the restorative portion of treatment is delayed or inadequate. If a tardy or non-compliant patient sees the dentist for definitive restoration only after the temporary filling is lost and leaking saliva, or if the crown was seated with an open margin, recontamination may be inevitable.
Oliveira et al., noted that “Although many factors of technical order are involved in the failure of endodontic treatment, the emergence of bacteria that resist therapy and proliferate in the root canal, or that contaminate the canal after endodontic treatment through coronal microleakage, is primarily responsible for unsuccessful treatment.” Even if the coronal seal is effective at the time of endodontic treatment, sometimes, the filling can be exposed to the oral environment due to failures or losses of restorations, fractures of the dental structure or the restorative material, during the intraradicular preparation for post placement or loss of the prosthetic crown, exposing the intracanal post to the buccal environment. This leaves the root canal open to invading bacteria. Oliveira et al, continues that enterococcus faecalis, which is frequently found in root canals, demonstrates resistance to endodontic disinfection procedures during chemical-mechanic protocols and has the ability to survive in root canals as a single species without the need for a cooperative relationship with other bacteria. The influence of diet and saliva also can affect the clinical situation.3
Impact of restorative treatment
When referring the case to an endodontist for treatment, it is important for the endodontist and restorative dentist to have a strong and close relationship, and both understand the importance of the endo/restorative continuum. Atlas, et al, explains that “The quality of the coronal restoration is at least equal to or even more important for the endodontic treatment outcome than the quality of the actual root canal treatment. Hence, endodontic treatment cannot be considered completed unless the crown is adequately restored.”4
Permanence of the restoration is key. One study of 166 patients (176 teeth) found that the success of endodontic treatment was much more likely when restored with either cast restorations (91.7%), amalgam restorations (86.5%), or composite restorations (83.0%) than with teeth restored with temporary restorations. The study noted that “loss of endodontically treated teeth occurred more often with those restored with temporary restorations (34.5%) than other restoration types.”5
Time is of the essence
It is generally advised that once root canal treatment has been completed, the patient should not wait longer than two weeks to have the tooth restored. Leakage of bacterial endotoxins and enzymes can begin within 48 hours. The “rule of thumb” is if the tooth has been leaking for more than one month, then endodontic retreatment should be considered.1
There are well documented studies on why well-treated teeth can fail, which back up the assertion that regardless of the obturation technique or filling material, entire “recontamination of the root canal can occur after a short period of microbial challenge.” After the coronal seal is lost, microorganisms and other irritants from saliva may reach the periradicular tissues via lateral canals or apical foramen. Clinically, since it is not possible to find out whether the entire root canal system is recontaminated after exposure to saliva, it is probably not prudent to restore a tooth with a root canal that may be completely recontaminated. Therefore, from a clinical standpoint, coronal exposure of the root canal obturation to saliva for a relatively short period of time (30 days or more) might be considered an indication for retreatment.”1,7,8,9 It is accepted that since water-soluble temporary cements have low resistance to compression, the temporary restoration should be replaced as soon as possible with the definitive restoration.
Some say that there has been a paradigm shift in endodontic treatment philosophy on whether the endodontic treatment or restorative phase has a greater impact on the outcome of root canal treatment. A study by Ray and Trope6 found that the coronal restoration had a greater impact on success than the quality of root canal treatment. An article by Gillen et al, noted, “Naturally, as endodontists, we would like to think that a well-performed root canal treatment is more important. However, as research scientists, we welcomed and admired the candidness of these clinical scientists in alerting our profession to the potential impact of previously less-emphasized aspect of coronal contamination on the maintenance of periapical health.”8
Situations that happen more often than I would like in my practice involve patients who leave my office with a beautifully performed root canal procedure with instructions to see the referring dentist as soon as possible to receive the definitive restoration. When patients are out of pain, they occasionally become out of compliance. Many return with a washed-out temporary filling and failed treatment. On occasion, the definitive crown is delayed due to many circumstances such as costs, waiting for crown lengthening to heal, fistulae to resolve, or perhaps waiting for large lesions to show a reduction in size. But regardless of the reasons, it is imperative to restore the access opening with a well-timed and quality-oriented bonded restoration as soon as possible to prevent salivary contamination. The authors recommend that the best time to restore an endodontically treated tooth is at the time of obturation whenever possible.
Conclusion
The success of root canal treatment does not end when the canals are cleaned, shaped, and filled—it hinges on the seamless transition to timely, effective restorative care. The delicate balance of eliminating bacteria during endodontic treatment and preventing reinfection through proper sealing underscores the importance of the endodontic-restorative continuum. As the research clearly shows, even the most technically proficient root canal treatment can fail if delayed or substandard restorative work allows for microleakage and bacterial invasion.
A collaborative approach between the endodontist and restorative dentist is essential to ensure that patients receive comprehensive care from start to finish. Moreover, patient compliance plays a pivotal role; timely restoration minimizes the risk of recontamination and increases the likelihood of long-term success.
Ultimately, the best time to restore a tooth is immediately following obturation—this is not merely a recommendation but a crucial factor for clinical success. By fostering stronger communication between specialists, encouraging patient adherence, and prioritizing swift restorative treatment, we can enhance outcomes and ensure the long-term survival of endodontically treated teeth (Figs. 1A, 1B, 2A, 2B, 3A and 3B).
 Fig. 1A
Fig. 1A
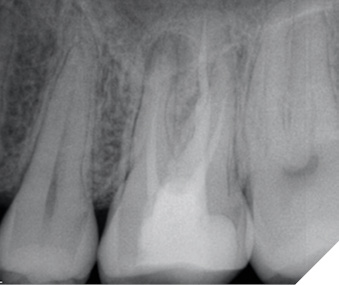
Fig. 1B
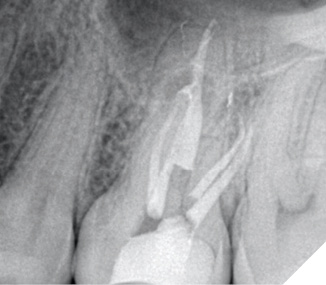
Fig. 2A

Fig. 2B

Fig. 3A

Fig. 3B
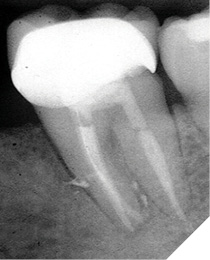
NOTE: Although the root canal was retreated appropriately and composite was bonded in the coronal aspect of each of the canals, and the distal marginal leakage area was sealed, a NEW crown must be considered as there is potential for continued leakage due to the open distal crown margin. This case was treated this way as the patient at the time could not yet afford a new properly fitted crown.
Oral Health welcomes this original article.
References
- Khayat A, Lee SJ, Torabinejad M. Human saliva penetration of coronally unsealed obturated root canals. J Endod. 1993 Sep;19(9):458-61. doi: 10.1016/S0099-2399(06)80533-9.
- Huang D, Wang X, Liang J, Ling J, Bian Z, Yu Q, Hou B, Chen X, Li J, Ye L, Cheng L, Xu X, Hu T, Wu H, Guo B, Su Q, Chen Z, Qiu L, Chen W, Wei X, Huang Z, Yu J, Lin Z, Zhang Q, Yang D, Zhao J, Pan S, Yang J, Wu J, Pan Y, Xie X, Deng S, Huang X, Zhang L, Yue L, Zhou X. Expert consensus on difficulty assessment of endodontic therapy. Int J Oral Sci. 2024 Mar 1;16(1):22. doi: 10.1038/s41368-024-00285-0. PMID: 38429281; PMCID: PMC10907570.
- Oliveira SG, Gomes DJ, Costa MH, Sousa ER, Lund RG. Coronal microleakage of endodontically treated teeth with intracanal post exposed to fresh human saliva. J Appl Oral Sci. 2013 Sep-Oct;21(5):403-8. doi: 10.1590/1679-775720130184. PMID: 24212985; PMCID: PMC3881841.
- Atlas A, Grandini S, Martignoni M. Evidence-based treatment planning for the restoration of endodontically treated single teeth: importance of coronal seal, post vs no post, and indirect vs direct restoration. Quintessence Int. 2019;50(10):772-781. doi: 10.3290/j.qi.a43235. PMID: 31559397.
- Lynch CD, Burke FM, Ní Ríordáin R, Hannigan A. The influence of coronal restoration type on the survival of endodontically treated teeth. Eur J Prosthodont Restor Dent. 2004 Dec;12(4):171-6. PMID: 15691191.
- Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995 Jan;28(1):12-8. doi: 10.1111/j.1365-2591.1995.tb00150.x.
- Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2008;July 7. https://doi.org/10.1046/j.1365-2591.2001.00396.x. Accessed January 7, 2025.
- Gillen BM, Looney SW, Gu LS, Loushine BA, Weller RN, Loushine RJ, Pashley DH, Tay FR. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod. 2011 Jul;37(7):895-902. doi: 10.1016/j.joen.2011.04.002. Epub 2011 May 24. PMID: 21689541; PMCID: PMC3815527.
- Heling I, Gorfil C, Slutzky H, Kopolovic K, Zalkind M, Slutzky-Goldberg I. Endodontic failure caused by inadequate restorative procedures: review and treatment recommendations. J Prosthet Dent. 2002 Jun;87(6):674-678.doi: 10.1067/mpr.2002.124453. PMID: 12131891.
About the authors

Dr. Gary Glassman lectures globally on endodontics, is on staff at the University of Toronto, Faculty of Dentistry in the graduate department of endodontics. He maintains a private practice, Endodontic Specialists in Toronto, Ontario, Canada. His personal/professional website is www.drgaryglassman.com, and his office website is www.rootcanals.ca.

Dr. Mazen Dagher is the founder and chief education officer of Dagher Institute, a learning center for professionals who wish to advance their skills in implant dentistry, prosthodontics, endodontics, and periodontal surgery. Dr Dagher also founded the Hawkesbury Dental Centre in 1999, a top-tier group practice.