
The goal of endodontic treatment is to prevent or cure, when present, Lesions of Endodontic Origin, at times referred to as apical periodontitis. The role of bacteria in the pathogenesis of endodontic disease is well established, and therefore, it is critical to eradicate these pathogens by employing the highest level of presently developed standards. This goal is clinically accomplished by Shaping, Cleaning, and Filling root canal systems. These 3 pillars are often referred to as the Endodontic Triad or, in modern terms, the Endodontic Trifecta.
The Role of Deep Shape in Endodontic Preparations
Grossman1 described mechanical cleaning as the most important part of root canal therapy. Later, Byström, and Sundqvist2 could show the efficacy of mechanical instrumentation alone, without antiseptic irrigants and intracanal dressings, to reduce the bacterial load of infected root canal systems. Later in 1985, the same authors demonstrated that the best results could be achieved with the combination mechanical debridement/antiseptic irrigation with NaOCl, hence the frequent use of the term “Chemo-mechanical Preparation.”3
It is biologically sound that sufficient mechanical instrumentation of the root canal system is necessary for debridement of all organic material, including predentine, and to allow the penetration and exchange of the irrigating solutions within the root canal system. The only way to create sufficient space in the apical region, without damaging this critical and delicate anatomic area, is to implement a precise Deep Shape preparation, ie, maintaining the apical extent of the root canal as small as practical with sufficient taper behind the physiologic terminus to allow the deep placement of the irrigating needle and irrigant agitation.
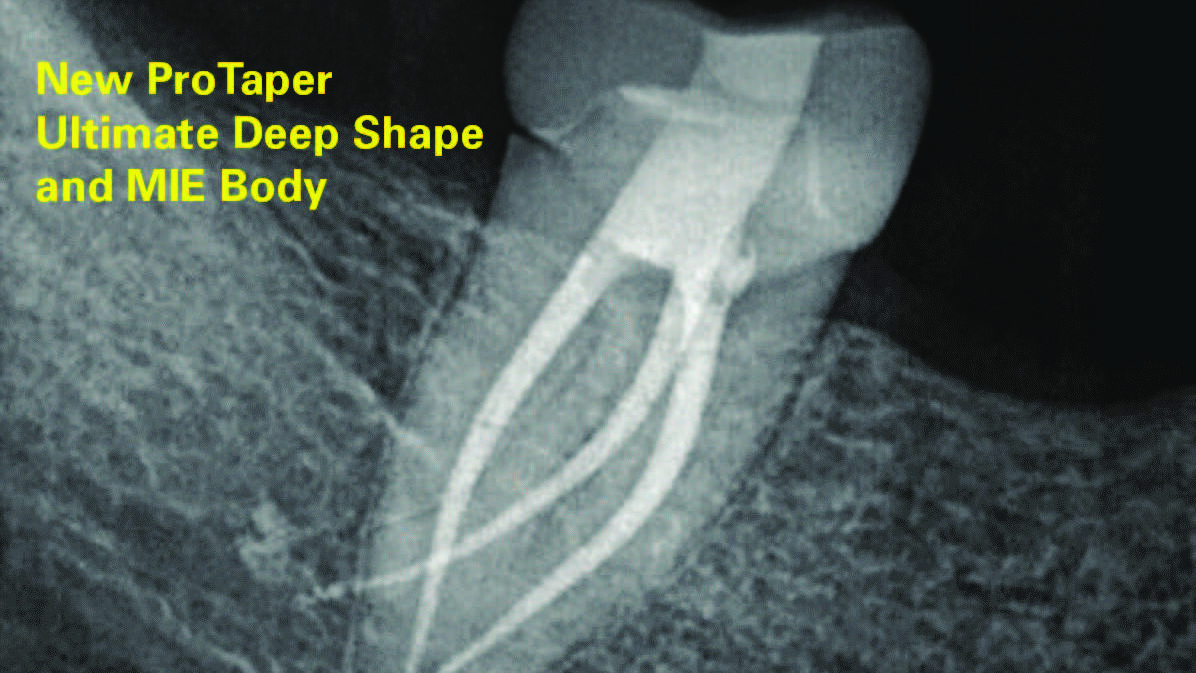
It is striking to notice that, as early as 2001, the ProTaper shaping system (Dentsply Sirona) had heralded Finishing files with progressive tapers of 7%, 8%, and 9% in their apical 3 mms of root canal preparations to cut a Deep Shape, followed by regressive tapers up to D16. The increased apical taper also provides access to the apical anatomy by shortening the length of lateral canals, therefore improving access to their cleaning. The recently launched ProTaper Ultimate endodontic shaping system (Dentsply Sirona) keeps the legacy of this unique and iconic feature, with the addition of a more conservative coronal preparation to respect, without compromise, the current Minimally Invasive Endodontic (MIE) (Fig. 1) preparation concept and trend.
Fig. 1
Indeed, the apical third is considered a “critical zone” because it is the most difficult part to clean and disinfect.4 The anatomical complexity of this apical area with fins, isthmuses, and ramifications represents a real niche harboring the most harmful micro-organisms and biofilms.5 Therefore, from a biological point of view, it would make sense to create apical preparations with larger sizes to optimize debridement and irrigation.6
As early as 1961, Ingle7 proposed a standardized technique with the then newly launched standardized endodontic instruments for the purpose of filling the apical third of the root canal initially with a silver point but later with a gutta-percha cone matching the exact diameter of the last instrument used at the working length. Increasingly sized reamers were successively used at the same working length to create a wide cylindrical preparation involving the whole canal cross section in order to mechanically clean it and, at the same time, provide a retention form with an apical stop to confine the filling material inside the root canal preparation. This technique, initially developed by the University of Washington in Seattle, was quickly adopted by many dental schools, including the Scandinavian dental schools. This standard was considered the reference technique for many years.
Following Kerekes and Tronstad’s6 studies, in 1991, Ørstavik et al8 were the first to advocate extensive reaming in the apical region to reduce the endodontic source of bacterial infection.This was confirmed by Dalton et al9 in 1998 who showed that the bacterial count was reduced with larger instruments sizes. According to Card et al,10 instrumentation of molars to size 60 and cuspids/bicuspids to size 80 showed that 81.5% of molars and 100% of cuspids/bicuspids were rendered bacteria-free at the end of the first appointment.
In addition to bacterial reduction,11 several studies have observed the positive effectiveness of increased apical preparation on the cleanliness of the apical third12 in respect to a positive outcome for apical periodontitis healing13 but also a negative effect on the sealing ability14 and postoperative pain.15,16 The main drawback of larger apical preparations is the increased risk of creating adverse iatrogenic errors such as ledges, canal transportations, perforations, zipping, and instrument fractures,17,18 especially in narrow and curved canals. A literature review, while advocating larger apical sizes, warns against procedural errors and asks to balance the degree of enlargement according to the canal anatomy.19
To overcome these mishaps, Weine et al20 advocated a telescopic preparation with enlargement of the apical part of the root canal 3 sizes larger than the first file that binds at the working length. This statement was clinically random and debatable. In 1974, Schilder21 proposed an innovative manual shaping technique based on each individual canal anatomy. Using recapitulations with reamers and utilizing the envelope of motion, it was possible to achieve tapered preparations refined in the apical region by designing a Deep Shape. Deep Shape was clinically confirmed when any given gauging file was snug at length and each consecutive larger K-file uniformly stepped out of the canal on the order of 0.5 to 1.0 mm, depending on the anatomy.
The Role of Deep Shape in 3D Endodontic Cleaning
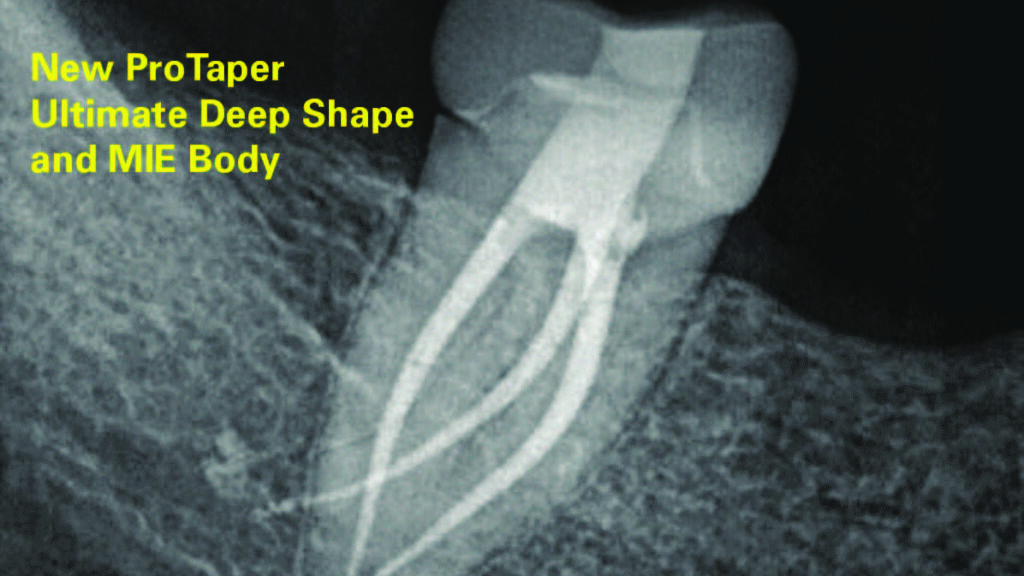
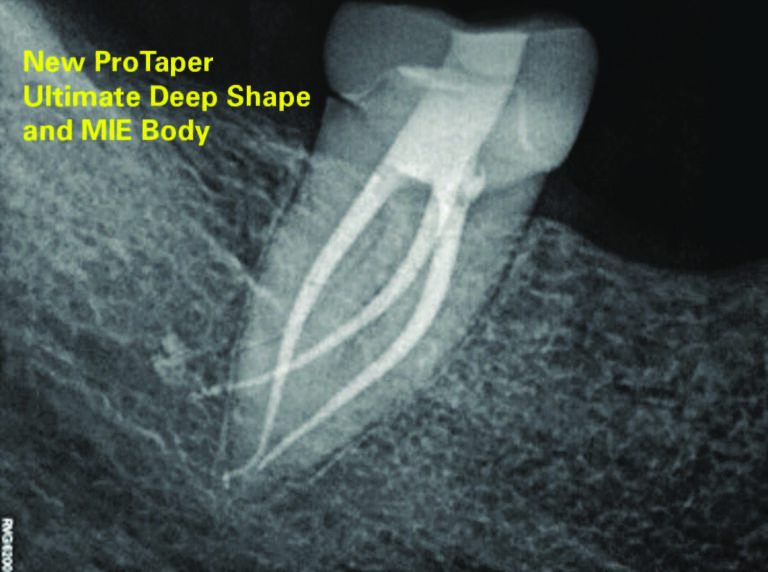
The Deep Shape allowed excellent mechanical debridement of the apical third simultaneously with improved apical cleaning due to the deep insertion of the irrigating needle and the creation of a reflux space enhancing the exchange of irrigants, as well as preparing a funnel shape enabling confined 3D Fillings (Fig. 2).22
Fig. 2
After shaping in vivo 60 root canals from anterior and posterior teeth and using a radiopaque solution for irrigation, Yana23 demonstrated in his Master’s thesis that the penetration and exchange of irrigant is complete at the end of the preparation only when the Deep Shape has been built in the apical region.In the Toronto study–Phase 4,24 which is the only study comparing the Schilder technique vs the standardized technique, the healing rate of the Schilder shaping technique with warm vertical compaction of gutta-percha was 10% higher than the standardized technique with lateral condensation: 87% vs 77%. The Schilder technique was considered as a measurably improved outcome predictor.
According to Coldero et al,25 when assessing the reduction of intracanal bacteria during root canal preparation with and without apical enlargement, reported, “It may therefore not be necessary to remove dentine in the apical part of the root canal when a suitable coronal taper is achieved to allow satisfactory irrigation of the root canal system with antimicrobial agents.”
According to Albrecht et al,26 “When a 0.10 taper can be produced at the apical extent of the root canal, there is no difference in debris removal between a size #40 and a size #20 preparation.”
Khademi et al27 have shown on mesiobuccal canals of extracted mandibular molars, that the minimum instrumentation size needed for penetration of irrigants to the apical third of the root canal is a #30 file, preferably with an 0.06 taper. Caron et al,28 using the ProTaper system for shaping difficult molar canals with different irrigation protocols, discovered that very high levels of root canal system cleanliness could be obtained in the apical third after sonic EndoActivator (Dentsply Sirona) activation and manual dynamic activation.
In a digital substraction radiographic ex vivo study, it was shown that cleaning and shaping root canals with ProTaper instruments improved penetration and exchange of irrigants.29
In a second study, the same authors identified that only active irrigation allowed complete irrigant penetration and exchange in curved canals after ProTaper shaping.30 For syringe irrigation alone, the level of the needle tip placement in the canal, which depends on the space allowed by the shaping procedure, was the most dominating factor.
Results from a study by Boutsioukis et al31 using an unsteady computational fluid dynamic stressed the impact of an increased taper for improving irrigant replacement and wall shear stress apical to the needle tip while reducing the risk for irrigant extrusion. It was demonstrated that a 30/09 tapered preparation with a ProTaper F3 was equivalent to a 60/02 preparation.
The Role of Deep Shape in 3D Endodontic Filling
The Deep Shape is also an essential component for sealing the root canal system after shaping. Proper Deep Shape provides the resistance form to contain the filling inside the root canal. In the early 1990s, Yared and Bou Dagher14,32 have showed in 2 studies the benefits of maintaining a small apical size compared to a large one in order to obtain a hermetic seal of the root canal system and avoid extrusion of filling materials. The Deep Shape is mandatory for softened gutta-percha techniques, such as warm vertical compaction and carrier-based obturation, to allow the capture of apical anatomy, which is an essential prerequisite determinant for predictably successful endodontics.33 A micro-computed tomography, studying the influence of apical taper on the quality of thermoplasticized root canal fillings, found that shaping the apical third (last 3 mm) of root canals to an 8% taper is necessary to achieve a better sealing ability and thus long-term success for root canal obturations.34
The recent availability of bio silicate sealers has updated the use of the single cone technique. But, as opposed to the old, standardized technique,7 all current canal preparations are performed with tapered instruments. So, to expect a 3D seal, a perfectly matching gutta-percha cone is mandatory. Germain et al35 have assessed the influence of root canal taper on the apical adaptability of 3 root canal sealers and matching GP cones used in a single cone technique by measuring void’s volume. In this study, 6% tapered preparations showed significantly less voids compared with a 4% tapered preparation. In a confocal microscopic evaluation, Eid et al36 have assessed the impact of warm vertical compaction (WVC) on the sealing ability of calcium silicate-based sealers in comparison with the single cone technique (SCT). WVC allowed better penetration at 1 mm and 5 mm into the dentinal tubules than the SCT. After shaping with ProTaper Ultimate, whatever the filling technique used, the triple lock fit of the new Dentsply Sirona GP cones provides a better seal over a wider surface distance of the preparation walls.
In conclusion, available reliable data is poor so far to solve the dilemma between apical size and taper after shaping. There are very few randomized controlled clinical trials, and they assess mainly the effect of increased apical size on the outcome of healing radicular periodontitis15 and post-op pain.16,37 The only CONSORT prospective randomized clinical trial assessing, for the first-time, different preparation sizes combined with different apical tapers on the outcome of primary endodontic treatment was released in September 2021.38 Based on a thorough literature review and a stringent protocol, the results of this study showed that the minimum apical preparation required to adequately disinfect the canals was 25/0.06 or 30/0.04, which is in accordance with previous studies.25-27
Deep Shape Summary
The new ProTaper Ultimate shaping system, with a shorter range of instruments, simplifies the shaping procedure and combines a minimally invasive tapered preparation coronally with the predictably successful ProTaper Deep Shape, 3D Cleaning, and 3D Filling hallmark distinctions. Optimizing the essential elements of design, unique machining, and purpose-specific metallurgy allows the clinician to experience a seamless workflow through Slider, Shaper, and Finisher transitions. The ProTaper success story offers an entirely new performance benchmark not just for the dentist but also for our most important commodity: the patient. 
Reprinted with permission from Dentistrytoday.com
References
- Grossman L. Endodontic
Practice. Lea & Febiger; 1970. - Byström A, Sundqvist G. Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand J Dent Res. 1981;89(4):321–8. doi:10.1111/j.1600-0722.1981.tb01689.x
- Byström A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J. 1985;18(1):35-40. doi:10.1111/j.1365-2591.1985.tb00416.x
- Zehnder M. Root canal irrigants. J Endod. 2006;32(5):389–98. doi:10.1016/j.joen.2005.09.014
- Arnold M, Ricucci D, Siqueira JF Jr. Infection in a complex network of apical ramifications as the cause of persistent apical periodontitis: a case report. J Endod. 2013;39(9):1179–84. doi:10.1016/j.joen.2013.04.036
- Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endod. 1979;5(3):83-90. doi:10.1016/S0099-2399(79)80154-5
- Ingle JI. A standardized endodontic technique utilizing newly designed instruments and filling materials. Oral Surg Oral Med Oral Pathol. 196;14:83–91. doi:10.1016/0030-4220(61)90477-7
- Ørstavik D, Kerekes K, Molven O. Effects of extensive apical reaming and calcium hydroxide dressing on bacterial infection during treatment of apical periodontitis: a pilot study. Int Endod J. 1991;24(1):1-7. doi:10.1111/j.1365-2591.1991.tb00863.x
- Dalton BC, Orstavik D, Phillips C, et al. Bacterial reduction with nickel-titanium rotary instrumentation. J Endod. 1998;24(11):763–7. doi:10.1016/S0099-2399(98)80170-2
- Card SJ, Sigurdsson A, Orstavik D, et al. The effectiveness of increased apical enlargement in reducing intracanal bacteria. J Endod. 2002;28(11):779–83. doi:10.1097/00004770-200211000-00008
- Rollison S, Barnett F, Stevens RH. Efficacy of bacterial removal from instrumented root canals in vitro related to instrumentation technique and size. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(3):366–71. doi:10.1067/moe.2002.126164
- Fornari VJ, Silva-Sousa YT, Vanni JR, et al. Histological evaluation of the effectiveness of increased apical enlargement for cleaning the apical third of curved canals. Int Endod J. 2010;43(11):988–94. doi:10.1111/j.1365-2591.2010.01724.x
- Souza RA, Dantas JC, Brandão PM, et al. Apical third enlargement of the root canal and its relationship with the repair of periapical lesions. Eur J Dent. 2012;6(4):385–8.
- Yared GM, Bou Dagher FE. Apical enlargement: influence on the sealing ability of the vertical compaction technique. J Endod. 1994;20(7):313–4. doi:10.1016/S0099-2399(06)80091-9
- Saini HR, Sangwan P, Sangwan A. Pain following foraminal enlargement in mandibular molars with necrosis and apical periodontitis: A randomized controlled trial. Int Endod J. 2016;49(12):1116–23. doi:10.1111/iej.12583
- de Freitas Portela FSM, De Martin AS, Pelegrine RA, et al. Effect of Foraminal Enlargement on Postoperative Pain in Necrotic Single-Rooted Teeth: A Randomized Clinical Trial. J Endod. 2021;47(7):1046–51. doi:10.1016/j.joen.2021.04.008
- Ruddle CJ. Nonsurgical endodontic retreatment. J Calif Dent Assoc. 1997;25(11):769–75, 777, 779–86 passim.
- Buchanan LS. Shaping root canals, Part VI: GT File technique in abruptly curved canals. Dent Today. 2000;19(2):66-71, 166
- Baugh D, Wallace J. The role of apical instrumentation in root canal treatment: a review of the literature. J Endod. 2005;31(5):333–40. doi:10.1097/01.don.0000145422.94578.e6
- Weine FS, Healey HJ, Gerstein H, et al. Pre-curved files and incremental instrumentation for root canal enlargement. J Can Dent Assoc (Tor). 1970;36(4):155–7.
- Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18(2):269–96.
- Machtou P. L’irrigation en endodontie [Irrigation in endodontics]. Actual Odontostomatol (Paris). 1980;34(131):387–94. French.
- Yana Y. An in vivo comparative study of the penetration of sodium hypochlorite in root canal systems during cleaning and shaping procedures using the B.U. technique and the sonic instrumentation [Master’s thesis]. Boston: Boston University; 1989.
- de Chevigny C, Dao TT, Basrani BR, et al. Treatment outcome in endodontics: the Toronto study—phase 4: initial treatment. J Endod. 2008;34(3):258–63.
- Coldero LG, McHugh S, MacKenzie D, et al. Reduction in intracanal bacteria during root canal preparation with and without apical enlargement. Int Endod J. 2002;35(5):437–46. doi:10.1046/j.1365-2591.2002.00496.x
- Albrecht LJ, Baumgartner JC, Marshall JG. Evaluation of apical debris removal using various sizes and tapers of ProFile GT files. J Endod. 2004;30(6):425–8. doi:10.1097/00004770-200406000-00012
- Khademi A, Yazdizadeh M, Feizianfard M. Determination of the minimum instrumentation size for penetration of irrigants to the apical third of root canal systems. J Endod. 2006;32(5):417–20. doi:10.1016/j.joen.2005.11.008
- Caron G, Nham K, Bronnec F, et al. Effectiveness of different final irrigant activation protocols on smear layer removal in curved canals. J Endod. 2010;36(8):1361–6. doi:10.1016/j.joen.2010.03.037
- Bronnec F, Bouillaguet S, Machtou P. Ex vivo assessment of irrigant penetration and renewal during the cleaning and shaping of root canals: a digital subtraction radiographic study. Int Endod J. 2010;43(4):275–82. doi:10.1111/j.1365-2591.2009.01677.x
- Bronnec F, Bouillaguet S, Machtou P. Ex vivo assessment of irrigant penetration and renewal during the final irrigation regimen. Int Endod J. 2010;43(8):663-72. doi: 10.1111/j.1365-2591.2010.01723.x
- Boutsioukis C, Gogos C, Verhaagen B, et al. The effect of root canal taper on the irrigant flow: evaluation using an unsteady Computational Fluid Dynamics model. Int Endod J. 2010;43(10):909–16. doi:10.1111/j.1365-2591.2010.01767.x
- Yared GM, Bou Dagher FE. Apical enlargement: influence on overextensions during in vitro vertical compaction. J Endod. 1994;20(6):269–71. doi:10.1016/s0099-2399(06)80813-7
- West JD. The relationship between the three-dimensional endodontic seal and Endodontic failures [Master’s thesis]. Boston: Boston University; 1975.
- Zogheib C, Naaman A, Medioni E, et al. Influence of apical taper on the quality of thermoplasticized root fillings assessed by micro-computed tomography. Clin Oral Investig. 2012;16(5):1493–8. doi:10.1007/s00784-011-0638-4
- Germain S, Meetu K, Issam K, et al. Impact of the root canal taper on the apical adaptability of sealers used in a single-cone technique: a micro-computed tomography study. J Contemp Dent Pract. 2018;19(7):808–15.
- Eid D, Medioni E, De-Deus G, et al. Impact of warm vertical compaction on the sealing ability of calcium silicate-based sealers: a confocal microscopic evaluation. Materials (Basel). 2021;14(2):372. doi:10.3390/ma14020372
- Silva EJ, Menaged K, Ajuz N, et al. Postoperative pain after foraminal enlargement in anterior teeth with necrosis and apical periodontitis: a prospective and randomized clinical trial. J Endod. 2013;39(2):173–6. doi:10.1016/j.joen.2012.11.013
- Fatima S, Kumar A, Andrabi SMUN, et al. Effect of apical third enlargement to different preparation sizes and tapers on postoperative pain and outcome of primary endodontic treatment: a prospective randomized clinical trial. J Endod. 2021;47(9):1345–51. doi:10.1016/j.joen.2021.05.010
About the Authors

Dr. Pierre Machtou was the Charter President of the CPEA in 1988 and received the Pierre Fauchard’s Elmer S Best Memorial award in 2006. He has authored over 70 publications in peer-reviewed journals and has conducted lectures, seminars and workshops in over 60 countries.

Dr. John West is the founder and director of the Center for Endodontics. He received the Distinguished Alumni Award from the Boston University Henry M. Goldman School of Dental Medicine 1975. He is a thought leader for Kodak Digital Dental Systems. He serves on the editorial advisory boards for the Journal of Esthetic and Restorative Dentistry, Practical Procedures and Aesthetic Dentistry, and Microscope Enhanced Dentistry. Contact Dr. West at johnwest@centerforendodontics.com.

Dr. Clifford J. Ruddle is the founder and director of Advanced Endodontics (www.endoruddle.com), an international educational source website for endodontics. As an inventor, Dr. Ruddle has designed and developed several instruments and devices widely used internationally. He is well known for providing endodontic education through his teachings, clinical articles, multimedia products, webinars, and online presence.