
The intention of this article is not to discuss all the factors involved in formulating a diagnosis and treatment plan for anterior tooth wear, but rather to demonstrate the favourable outcome one can achieve when implementing a minimally invasive treatment option. The option involves optimal orthodontic tooth positioning using a clear aligner system followed by conservative restorative treatment.
Dr. Vince Kokich Sr., the pioneer of adult orthodontic treatment, recognized the value and benefit of positioning teeth in their optimal locations to facilitate the best possible dental treatment, both restoratively and periodontally, over 40 years ago.
He delivered the keynote presentation at the 40th Moyers Symposium at the University of Michigan, in 2013. The topic was “Evolution of Adult Orthodontics: The Importance of a Realistic Approach.”1 His goal in the presentation was to “explain and document how adjunctive orthodontics, managed in an interdisciplinary manner, can help the general dentist to produce exceptional restorative outcomes for their adult patients.” The clinical situation, anterior tooth wear, was at the top of his list.
The challenges of anterior tooth wear
One of the greatest challenges a restorative dentist encounters is the adult patient presenting with anterior tooth wear. These patients accept the wear of their anterior teeth as the result of having a long life. Most dentists also accept this clinical situation as “normal wear and tear” of teeth over many years. The challenge with this approach is that dentin has been shown to be 4.22 and 4.5-7 times softer3 than enamel and if the situation is left untreated, the wear can potentially continue resulting in sensitivity, significant loss of tooth structure, loss of anterior guidance contributing to an undesired, and unaesthetically pleasing appearance.
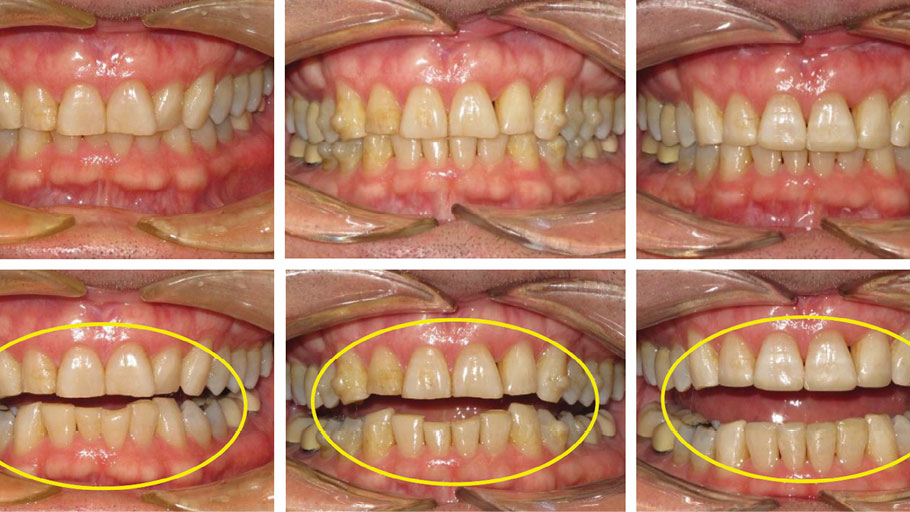
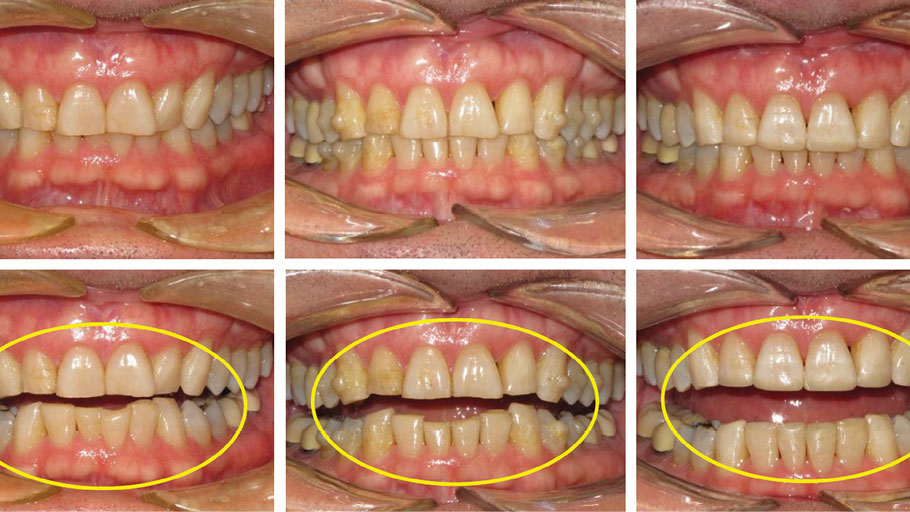
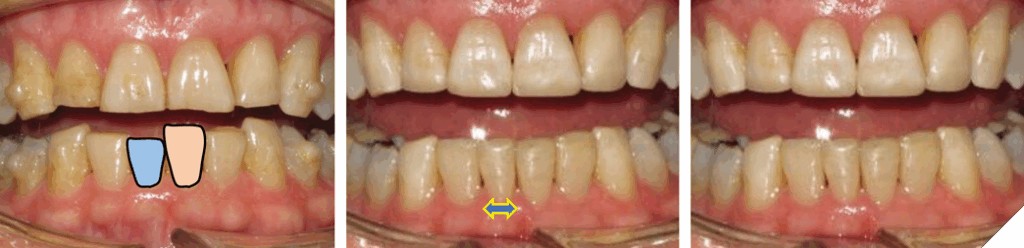
The patient in Figure 1 presented to the clinic is this situation, however, the process started much earlier. The loss of tooth structure due to wear is slow and gradual, taking place over many years. It usually starts with chipped, fractured and worn incisal edges. These patients can cover a spectrum of ages, from young adults to senior citizens (Fig. 2).
Fig. 1
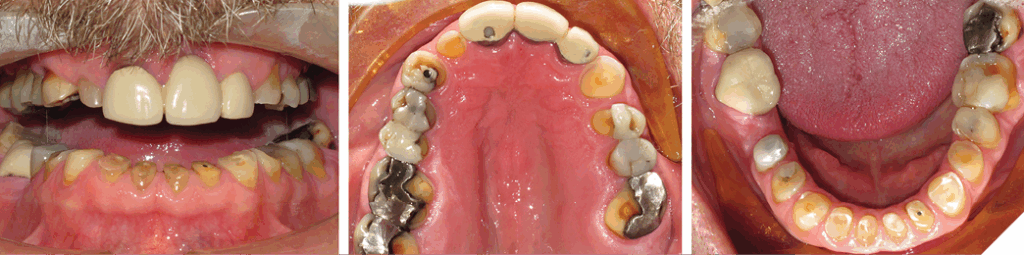
Fig. 2

Influence of bruxism and overbite
One of the leading causes of tooth wear is bruxism. The root cause of bruxism is multifactorial and requires a separate in-depth discussion. The appropriate diagnosis of clinical tooth wear will enable the dental clinician to develop a treatment plan with a realistic and predictable outcome, and a favourable long-term prognosis.
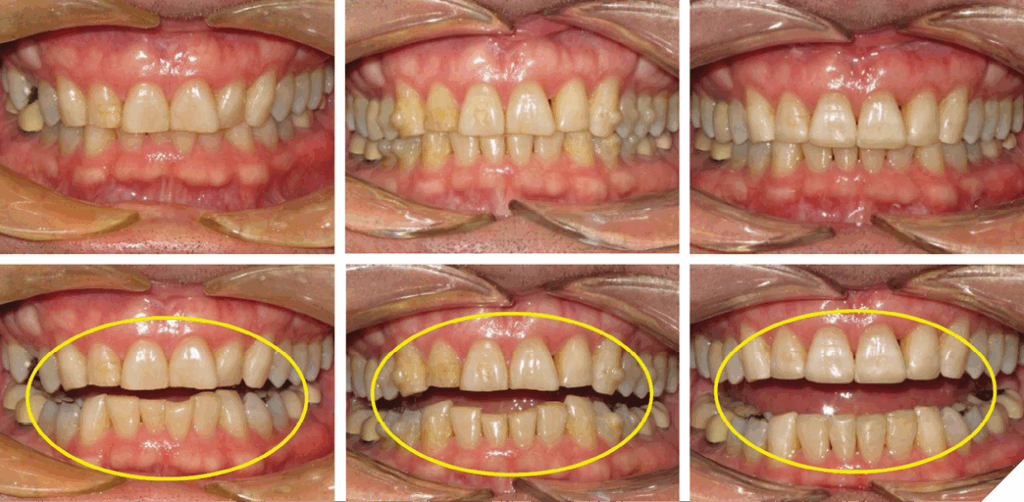
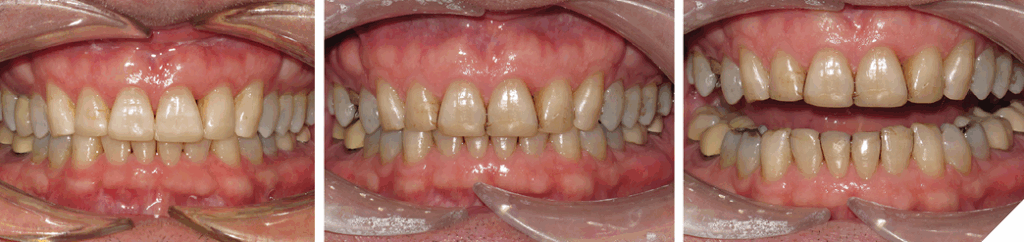
The extent of tooth wear can also be influenced by excess overbite. The positioning of the anterior teeth and a history of bruxism will have a major impact on the degree of tooth destruction (Figs. 3 and 4). Unless the excess overbite is addressed and managed, the prescribed restorations usually have a poor long-term prognosis.
The degree of overbite is a direct result of the body’s response, referred to as Dento-Alveolar Eruption (DAE), to a lack of opposing anterior tooth contact. The lack of contact can be skeletal and/or dental in origin (Figs. 5-7).
Fig. 3

Fig. 4

Fig. 5
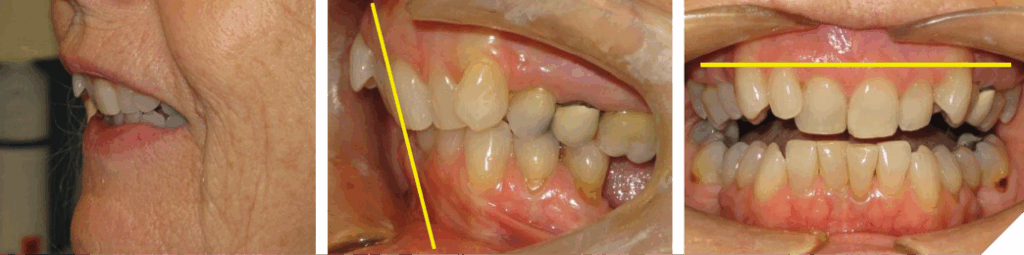
Fig. 6

Fig. 7

Clinical examples of eruption patterns
The concept of DAE has been demonstrated by Dr. Peter Dawson in his textbook “Functional Occlusion: From TMJ to Smile Design” with the topic of ‘Balance of Eruptive Forces.’4 Dr. Frank Spear has also demonstrated this concept of DAE when referring to ‘Compensatory Eruption in response to tooth wear’ during the SPEAR Education course ‘Treating the Worn Dentition.’5
Clinically, excess overbite can result from several situations: Dento-Alveolar Eruption of the maxillary incisors, mandibular incisors or a combination of both (Fig. 8).
The author has shown when the maxillary and/or mandibular incisors are re-positioned into a more favourable location, reducing the overbite and improving the overjet, the resulting anterior occlusion can provide the subsequent restorations with a long lasting and stable occlusal environment (Fig. 9).
Fig. 8
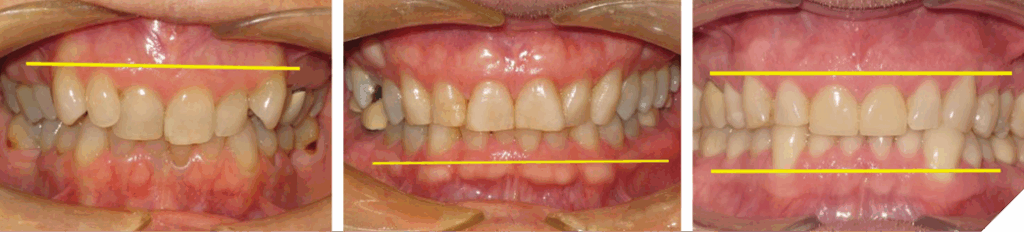
Fig. 9

Treatment approaches
Over the years, many treatment options have been devised to overcome the challenge of treating anterior tooth wear. The author has divided them into two groups: 1) without and 2) with orthodontic treatment. Within each group, a sub-category exists: i) Surgical and ii) Non-surgical. The 1st group (Figs. 10 and 11), ‘Without Orthodontic Treatment’ and ‘Non-surgical treatment’, involves a restorative ONLY approach, increasing the Vertical Dimension of Occlusion (VDO). This approach works very well, but it involves many restorations, some might not be structurally necessary. The clinician must decide if the number of restorations is warranted and have this discussion with the patient. The next group (Figs. 12 and 13), refer to ‘Without Orthodontic Treatment’ and ‘Surgical treatment’.
Fig. 10

Fig. 11
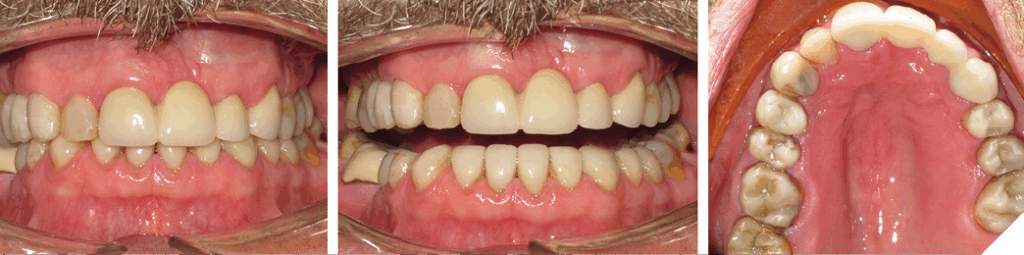
Fig. 12

Fig. 13
If the goal is to restore worn anterior teeth and increase clinical crown height, the following options exist:
Without orthodontic treatment:
- Non-surgical treatment (Figs. 10 and 11)
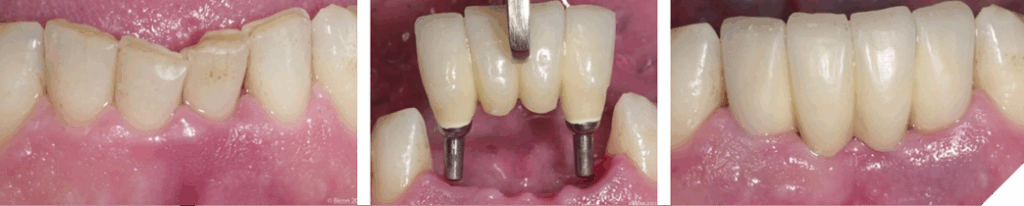
- Periodontal surgical and restorative treatment (Fig. 12)
- Extraction and Implant Treatment (Fig. 13)
With orthodontic treatment:
- Orthognathic Surgery: to balance the skeletal foundation, improve facial aesthetics and dental relationship.
- Orthodontic with Periodontal surgical treatment: if desired amount of orthodontic intrusion was not realized clinically, and clinical crown lengthening indicated, followed by restorative treatment.
- Orthodontic and Restorative Treatment ONLY, No Surgery: Dento-Alveolar Intrusion (DAI) of incisors, develop level plane of occlusion, minimal change in VDO, develop interincisal space to lengthen clinical crown restoratively. This option is referred as “Non-surgical Clinical Crown Lengthening” (Fig.14).
Non-surgical clinical crown lengthening offers soft and hard tissue benefits. The soft tissue benefits include maintaining the size and shape of the interdental papillae, the scalloping of the gingival margins and conservative levelling of the gingival margins (Fig. 15).
The hard tissue benefits include minimally invasive tooth preparation for conservative restorations, maintains maximum amount of enamel to bond to, thus avoiding exposing cementum, prevents the exposure of the narrower portion of the root at the gingival margin, and reduces need for surgical intervention (Fig. 16).
Fig. 14
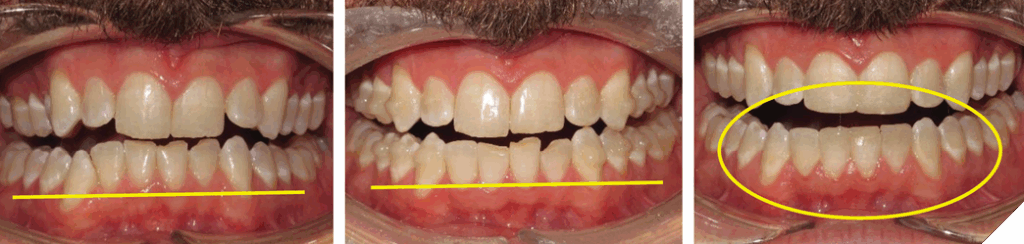
Fig. 15
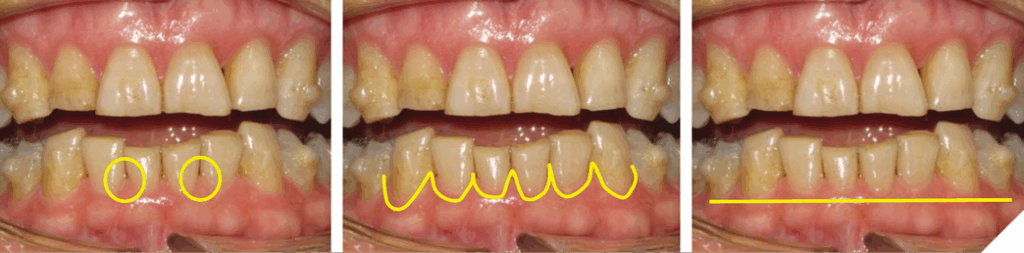
Fig. 16
Dr. Vince Kokich Sr. published an article in the JADA, 2008, discussing option 3.6 The concept involves reversing the natural response of the body to the lack of anterior tooth contact, Dento-Alveolar Eruption (DAE). He demonstrated one can increase the interincisal space by applying an orthodontic force to the mandibular incisors without causing any serious consequences to the root structure and supporting alveolar bone. As the teeth were intruded, staying within the alveolar housing, the alveolar crest followed the Cementoenamel Junction, and the overlying gingiva followed the alveolar crest. This author wanted to emphasize the technique is not a relatively new concept, but rather 35 years old. Dr. B. Melsen published a paper back in 1989 discussing incisor intrusion.7 The only difference to the previous approach is the use of clear aligners as the appliance, not conventional brackets and wires.
The best appliance to perform Dento-Alveolar Intrusion (DAI) for the adult patient is a clear aligner system. The system offers excellent vertical control, targeted gentle intrusive orthodontic forces and exceptional access to oral hygiene during treatment. A clear aligner system is a patient friendly and socially acceptable alternative to conventional brackets and wires. The combination of a clear aligner system prior to restorative treatment can provide the patient with outcomes they have always desired.
These advantages allow the clinician to rehabilitate the anterior worn dentition in a minimally, invasive manner and will provide the patient with an aesthetically, pleasing smile with optimal function for many years.
Case studies
All the following cases were treated using the clear aligner system Invisalign.
Case #1: Compensatory DAE in response to wear
A 64-year-old male has been receiving routine dental care over the years. The treating dentist did not have the knowledge to treat the anterior tooth wear. The provider attended a two-day course, “Treating the Worn Dentition”, offered by SPEAR Education and also completed the recommended workshop. Armed with the necessary knowledge and confidence, the patient underwent the treatment seen in Figure 17.
Fig. 17
Bruxism can lead to loss of incisal tooth structure, followed by compensatory DAE. The patient usually presents with level incisal edges and uneven gingival margins. Orthodontic DAI will produce uneven incisal edges with level gingival margins. This new arrangement allows the patient to receive four equally sized lower incisors and improved anterior guidance, with favourable overjet/overbite which reduces the risk of catastrophic destruction of tooth structure (Fig. 18).
Fig. 18
Case #2: DAE due to lack of anterior contact caused by a skeletal discrepancy
A 35-year-old male presented with a chief complaint of the lower teeth “chipping away”. The patient is a non-growing individual with a Class II skeletal base. The patient was advised the existing overjet could only be corrected with mandibular jaw advancement surgery. The patient declined this treatment option. It was advised a lifetime retention protocol would be necessary to maintain the desired tooth position (Figs. 19, 20 and 21). He was also not concerned of the midline discrepancy and Class II relationship on the left side.
Fig. 19
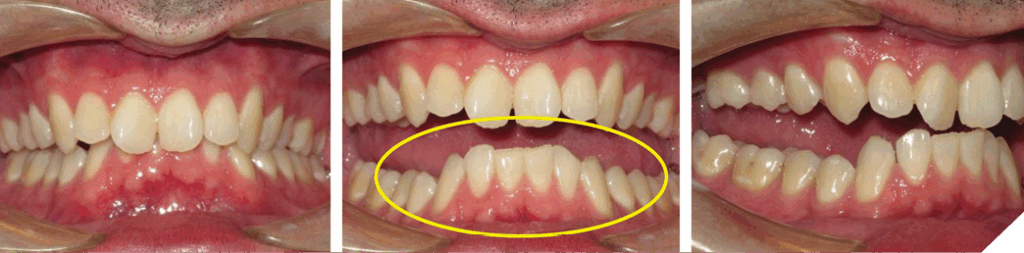
Fig. 20
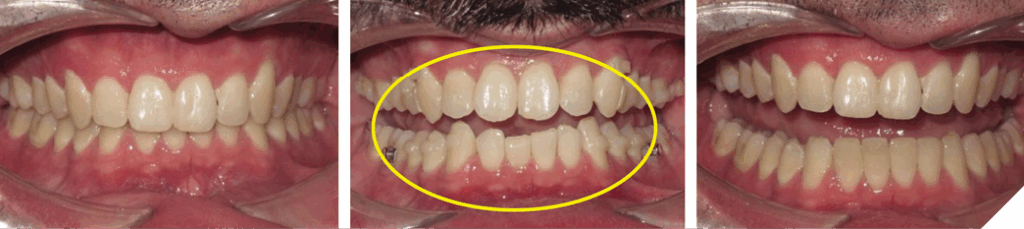
Fig. 21

Case #3: DAE due to lack of anterior contact caused by a dental origin…missing teeth
The case demonstrates the degree to which the alveolar complex will undergo DAE until it encounters an opposing contact. In this case, the contact was provided by the opposing cast RPD framework. It does not represent significant anterior tooth wear, however, if the patient had teeth 11/21 present, and with the degree of overbite, one can imagine the extent of wear on the lower incisors. The treatment demonstrates the surprising amount of DAI a clear aligner system can achieve (Figs. 22, 23 and 24).
Fig. 22
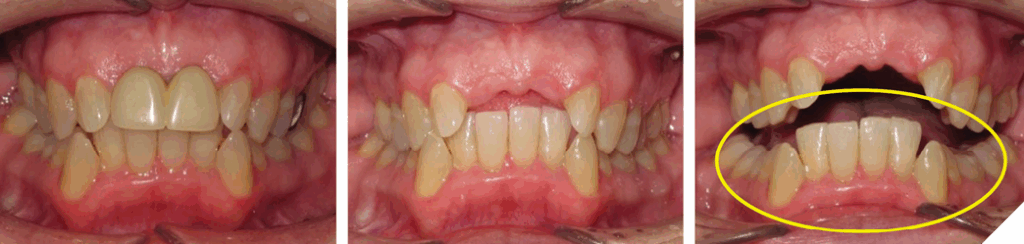
Fig. 23

Fig. 24

The patient had been edentulous for over 45 years, and it was deemed she was not a suitable candidate for implant treatment due to the unpredictability of the hard and soft tissue grafting necessary to augment the deficient area; thus, a fixed bridge was planned.
Case #2 was a very challenging case and was treated very early in the author’s Invisalign journey. Initially, the author was expecting an unrealistic outcome from the clear aligners. After a period of time, during which he re-evaluated the aligner force system, a very satisfactory outcome was achieved.
Summary of treatment time:
| Case | Treatment Time | Sets of Additional Aligners |
| #1 | 29 stages @10 day intervals, 41 weeks | None |
| #2 | Many stages over 20 months | 3 Sets |
| #3 | 52 stages @ 7 day intervals, 52 weeks | 1 Set |
Conclusion
During his keynote presentation, Dr. Kokich remarked that the “majority of pre-doctoral dental students are unaware of the benefits of pre-restorative orthodontics. We should recognize this deficiency in pre-doctoral dental education.” It is noteworthy that he spoke these words, or the like, 15 times. Dr. Kokich strongly emphasized the need for further education in this area. In the 12 years since his presentation, not much progress has been made in educating the dental profession, the restorative dentist and specialties alike, of the benefits of orthodontic assisted dentistry. This dentist wants the journey to continue.
The clinical management of anterior tooth wear is very challenging. It requires a thorough diagnosis and the implementation of a realistic and predictable treatment plan to provide the patient with the best possible outcome dentistry can provide. When one uses an ‘ortho first’ approach, these outcomes can be realized in a minimally invasive manner, both non-surgically and restoratively. 
Oral Health welcomes this original article.
References
- Kokich VG, The Evolution of Adult Orthodontics, The 40th Moyers Symposium, Needham Press, (2013): p.29 – 58.
- R.G. Craig and F.A Peyton, The microhardness of enamel and dentin. J Dent Res., 37, (1958) 661 – 668.
- Chun K, Choi H, Lee J. Comparison of mechanical property and role between enamel and dentin in the human teeth. J Dent Biomech. 2014 Feb 6;5
- Dawson, P.E, Functional Occlusion, From TMJ to Smile Design, Mosby Elsevier.
- Spear Education. Treating the Worn Dentition [seminar]. Scottsdale, Ariz. 2015.
- Bellamy LJ, Kokich VG, Weissman JA. Using orthodontic intrusion of abraded incisors to facilitate restoration: the technique’s effects on alveolar bone level and root length. J Am Dent Assoc. 2008 Jun;139(6):725-733.
- Melsen B, Agerbaek N, Markenstam G. Intrusion of incisors in adult patients with marginal bone loss. Am J Orthod Dentofacial Orthop. 1989 Sep;96(3):232-41.
- Spear FM, Kokich VG, Mathews DP. Interdisciplinary management of anterior dental esthetics. J Am Dent Assoc. 2006 Feb;137(2):160-169.
About the author

Dr. Richard Schmidt is a graduate of the Faculty of Dentistry, University of Toronto in 1988, and has been a presenter for Align Canada, Halton–Peel Dental Association and Victoria District Dental Society. He became a member of SPEAR Education in 2014 and a Study Club Leader of the ‘SPEAR Study Club of Dental Nerds’ in 2022. He also organized the ‘Orthodontic Dentistry Study Club’ the same year. He was a semi-finalist and finalist at the Invisalign GP Summit and prepared Poster Presentations for the Moyers Symposium at the University of Michigan. He is currently presenting “How to Manage the Compromised Dentition” on behalf of the Headwaters Dental Society and will be presenting at an upcoming ODA ASM.