
Abstract
Facial differences and temporomandibular joint (TMJ) disorders often coexist. Some dentofacial deformities can be a common primary cause of TMJ pathology or develop as a secondary result of joint disease. Patients with these concurrent pathologies benefit from simultaneous surgical management of both issues, typically involving OGS and alloplastic total joint reconstruction (TJR). This article will demonstrate that the current evidence supports combined temporomandibular joint reconstruction and orthognathic surgery as a safe and effective treatment for patients with facial differences and late-stage TMJ disease. Benefits of C-TJR-OGS such as decreased treatment time, reduced pain, optimized occlusal function, and improved aesthetic balance will be explored along with clinical photographs highlighting patient outcomes.
Facial differences requiring surgical correction frequently coexist with temporomandibular joint (TMJ) disorders. Regardless of whether a patient’s temporomandibular joint pathology is a causative factor for their dentofacial deformity or develops secondary to a pre-existing deformity, patients with these concomitant conditions often benefit from combined surgical intervention. Orthognathic surgery (OGS) alone, which is aimed at correcting the facial deformity, may also alleviate pain and dysfunction of the joint. OGS will not, however, correct any inherent anatomic pathology of the joint. The need to treat coexisting dentofacial deformities and TMJ disease raises the clinical question of how to optimally address both conditions to achieve the best surgical outcomes. Surgical treatment for these patients typically includes alloplastic total joint reconstruction (TJR) and OGS, which are often undertaken concurrently.1 Performing combined TJR and OGS in these patients can significantly decrease treatment times and yield better outcomes with regards to form and function.2
Orthognathic surgery, commonly known as corrective jaw surgery, refers to a subset of orthopedic surgical procedures where bony osteotomies are performed to reposition the maxillomandibular complex. The goal of OGS is to achieve a functionally ideal occlusion, balanced facial aesthetics, and increased airway patency. The basic orthognathic surgical procedures, either performed in combination or separately, generally include the LeFort I maxillary osteotomy (LFI), bilateral sagittal split mandibular osteotomy (BSSO), and sliding genioplasty. By performing a combination of these procedures, movement of the maxillomandibular complex in virtually any direction is possible. Evolving technologies, including virtual or digital surgical planning, have revolutionized OGS workflows and led to orthognathic surgeons being able to predictably practice these procedures successfully for decades with excellent outcomes. These procedures can now be performed in an ambulatory outpatient or short stay setting with high satisfaction rates (90%).3
Healthy and biologically stable temporomandibular joints are necessary for favorable OGS outcomes, as associated temporomandibular joint pathology often leads to unsatisfactory results in function, aesthetics, pain, and occlusal stability if left untreated.1 The stability of the temporomandibular joints is dependent on the integrity, positioning, and overall health of the mandibular condyle, glenoid fossa, articular disk, and peri-articular soft tissues. Pathologic temporomandibular joint conditions such as adolescent internal condylar resorption (AICR), reactive arthritis, trauma, connective tissue or autoimmune diseases, ankylosis, congenital malformations of the joint complex, and other late-stage temporomandibular joint diseases can lead to markedly degenerated and non-salvageable temporomandibular joints. These conditions are also often associated with dentofacial deformities and malocclusion.
Alloplastic total joint replacement (TJR) has become an accepted and widely available procedure in the treatment of end-stage temporomandibular joint disease.1 Although conservative management remains the first line treatment for mild-to-moderate TMJ dysfunction, alloplastic TJR offers a safe and viable surgical solution for patients with severe joint deformity, fibrous or bony ankylosis, joint pathology or loss of function. Compared to historical methods of TMJ reconstruction, alloplastic TJR also offers several advantages such as improved access to treatment, reduced operative time, earlier recovery of mobilization, elimination of a second surgical donor site, and lower overall risk of morbidity. Surgical advancements in the last few decades have overcome early challenges including unsuitable material selection and poor prosthetic design. The modern-day alloplastic temporomandibular joint replacement prosthesis was developed in the late 1990s and has since become a mainstay in the management of late-stage TMJ dysfunction.4 Alloplastic TJR prostheses consist of a mandibular ramal component and a glenoid fossa component to reconstruct the natural articulating surfaces of the TMJ. The mandibular component reconstructs the condylar process and part of the mandibular ramus. It is typically made from titanium (Ti-6AL-4V) alloy and/or nickel-containing cobalt-chromium-molybdenum (Co-Cr-Mo) alloy. The glenoid fossa component is made of ultrahigh molecular weight polyethylene (UHMWPE) with or without an unalloyed titanium mesh backing. This combination of materials provides the blend of strength, durability, flexibility, and biocompatibility needed to recreate complex TMJ functions.1 An effective TMJ prosthesis can withstand occlusal loads, allow for full range of motion, and remain stably fixated in place.
Major surgical advancements in the past twenty-five years have enabled combined temporomandibular joint and OGS (C-TJR-OGS) to be successfully performed in a single operation with accurate diagnosis and precise surgical planning.5 Some surgical centers describe that “approximately two-thirds of patients requiring TMJ TJR can benefit from concomitant OGS for improvement in function, airway and breathing capabilities, better aesthetic outcomes, and decreased or elimination of pain”.1 Like conventional OGS, C-TJR-OGS cases can be safely and accurately planned using computer-aided surgical simulation (CASS) technology.6 Conventional surgical planning for orthognathic cases was a lengthy and labor-intensive process requiring the use of dental models and articulators, thus introducing increased potential for error. CASS technology has allowed for precise visualization of planned osteotomies, increased efficiency, and the ability to accurately model orthognathic movements in three-dimensional space.7 It is important to note that like with any surgical intervention, realistic and well-informed patient expectations are essential for successful C-TJR-OGS cases. Careful pre-operative planning of orthognathic movements and placement of the alloplastic TMJ prostheses typically allow for a post-operative interincisal mouth opening of 30-35mm to be achieved. Patients can be counselled that a 60-70% reduction in preoperative pain levels and a functional diet 75% of normal are attainable post-operative goals with C-TJR-OGS.1 In appropriately selected patients, combined orthognathic surgical facial correction and alloplastic TMJ TJR offers a safe, predictable, efficient, and cost-effective treatment approach for end-stage temporomandibular joint disease in combination with dentofacial deformities.
The correction of combined dentofacial deformities with temporomandibular joint pathology often requires bimaxillary surgery to achieve a quality functional and aesthetic result. Orthognathic patients with concomitant TMJ pathologies are also often categorized as having a high occlusal plane angle facial morphology.5 These individuals have an increased occlusal plane angulation (>12 degrees), increased mandibular plane angulation, anterior vertical maxillary hyperplasia, posterior vertical maxillary hypoplasia, decreased vertical height of the posterior mandible, and a decreased projection of the chin. These patients also commonly have an anteroposterior maxillary and mandibular hypoplasia.1 Orthodontically, class II malocclusion is frequently seen in these individuals, and an anterior open bite may be accompanied by a pronounced curve of Spee in the maxillary arch.5 In particularly severe cases, these facial morphologies findings can lead to loss of incisal guidance and canine rise in the presence of working and non-working dental interferences in the molars. Along with dentofacial and orthodontic considerations, these patients often demonstrate moderate to severe sleep apnea symptoms because of posterior displacement of the tongue base and subsequent collapse of the oropharyngeal airway. These patients can also suffer from nasal airway obstruction secondary to turbinate hypertrophy and septal deviations. Active condylar resorption or degeneration can cause these facial changes and airway findings to become progressively worse over time.
The current body of literature supports both OGS and alloplastic temporomandibular joint replacement, either separately or in combination, as safe and effective treatment protocol(s) with research studies showing high rates of patient satisfaction, reduction of pain, and improved function. A current long term survivability study at our center is demonstrating excellent TJR survivability with a low replacement rate (2.8%) using a single patient specific implant (Zimmer Biomet TM Jacksonville, Florida).14 In 2005, a study of 224 TMJ total joint reconstruction cases found that patients had significant improvement in pain after 3 years post-surgery, with average patient-reported pain scores decreasing from 8.5/10 to 2.8/10.1,8 Measurements of maximum interincisal opening (MIO) also improved from 20.1 mm to 29.3 mm at the 3-year mark.1,8 Lastly, 99% of patients stated that they would choose to undergo the surgery again and ranked highly on patient satisfaction rating scales. A prospective cohort study by Wolford et al. in 2015 reported equally positive objective and patient-reported outcomes following TMJ total joint reconstruction surgery, including improved quality of life at a median of 21 years in patients who previously suffered severe TMJ degeneration and function loss.9-10 Dela Coleta et al. evaluated the surgical stability of 47 female patients after combined OGS and alloplastic TJR. After a mean follow-up period of 40.6 months, this patient cohort demonstrated an average Menton advancement of 18.4 mm and average reduction in the occlusal plane angle of 14.9°. After a mean follow-up period of 40.6 months, results demonstrated relatively minor maxillary horizontal changes with very stable mandibular measurements.11 Pinto et al. evaluated the same 47 female patients as mentioned above with regards to pain-related and functional outcomes.12 These patients were divided into two groups based on the number of previous surgeries (Group 1 having undergone 0–1 previous surgeries and Group 2 having two or more previous surgeries). Significant improvements (37–52%) were observed for jaw function, TMJ pain, diet, headaches. Interincisal opening reportedly increased by an average of 14%. The Mount Sinai Centre for TMJ Surgery has reported on its successful use in the management of large deformities using extended TMJ TJR.14
In summary, advancements in the past three decades have established combined temporomandibular joint and OGS (C-TJR-OGS) as a safe and reliable approach to the treatment of patients who present with coexisting facial differences and TMJ disease. With appropriate diagnosis and the aid of precise surgical planning technologies, these concurrent pathologies can be addressed in a single operation thus minimizing treatment time and improving patient outcomes in occlusal function, pain scores, and aesthetic balance.
Case Presentation:
A 24-year-old female patient was referred by her orthodontist to the Cleft Lip, Palate and Craniofacial Clinic at Holland Bloorview Kids Rehabilitation Hospital for consultation and management regarding her dentofacial deformity and temporomandibular joint pathology (Fig. 1). Her congenital malformation was consistent with TMJ condylar agenesis secondary to an undiagnosed Pierre Robin Sequence. Her chief complaint on presentation was her lack of ability to chew due to her open bite, difficulty swallowing and moderate sleep apnea.
Fig. 1

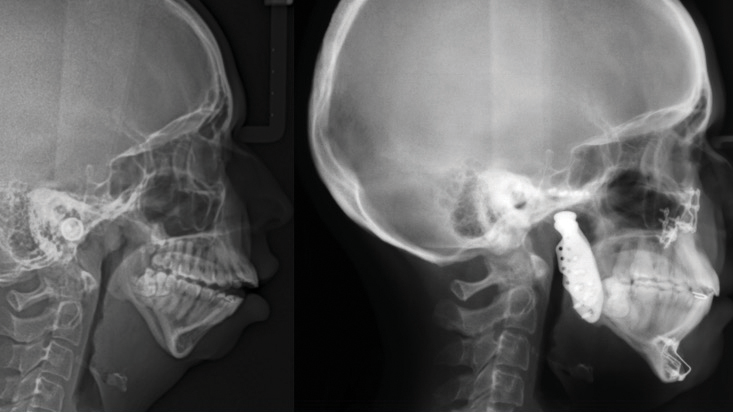
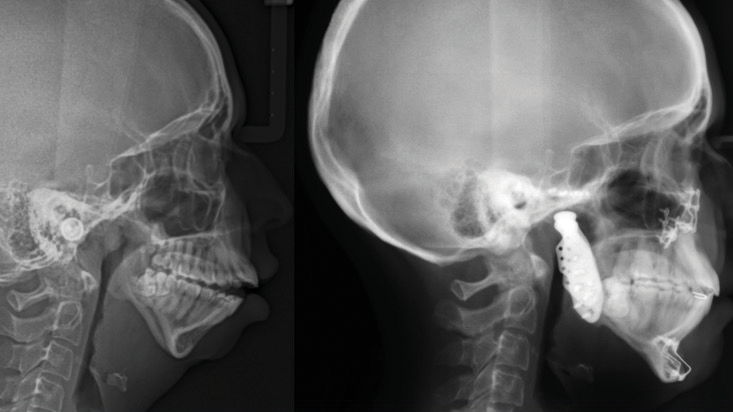
Her orthodontic history was significant for early adolescent treatment with 7 years of orthodontic therapy. She presented with a class II, division 2 skeletal malocclusion with 10mm overjet and a 5mm anterior open bite. Mild crowding was noted throughout the maxillary and mandibular arches. Orthognathic evaluation revealed a significant convex facial profile with severe mandibular retrognathia, microgenia, and posterior and anterior vertical maxillary excess. Posterior crossbite was noted on the left side with a notable transverse maxillary deficiency and deficient buccal corridors. Significant mentalis and peri-oral straining was noted on examination. Esthetic evaluation revealed a very short lower facial height, 5mm tooth exposure at rest, normal upper and short lower lip length, and incomplete vertical mental angle. Facial symmetry examination revealed that the patient’s mandible deviated to the left by about 3-4mm. Plain radiography (Fig. 2A&B) revealed the significant loss of condylar anatomy and minimal ramal height. Significant constriction of the airway is seen on the lateral cephalogram. Presurgical computed tomography revealed agenesis of the mandibular condylar process bilaterally, as well as severe morphologic deformity of the glenoid fossa and articular eminence bilaterally.
Fig. 2A
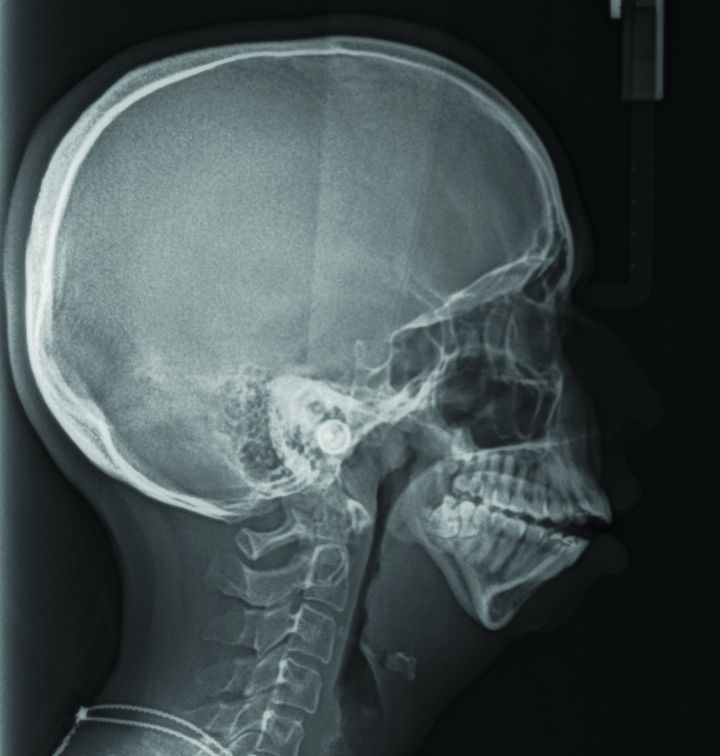
Fig. 2B
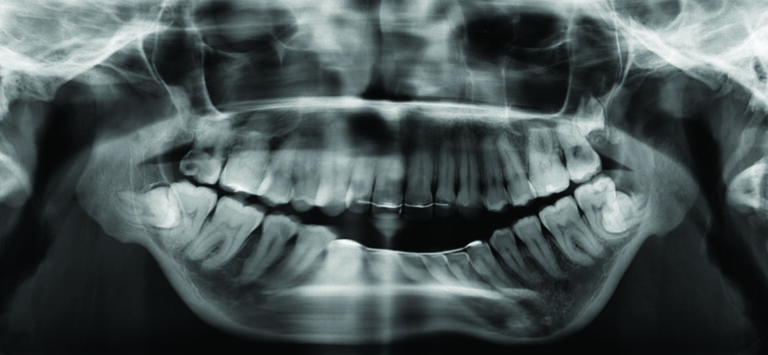
Following pre-operative orthodontic decompensation, (Fig. 3A&B, 4) the patient underwent the following surgical procedures:
Fig. 3A

Fig. 3B
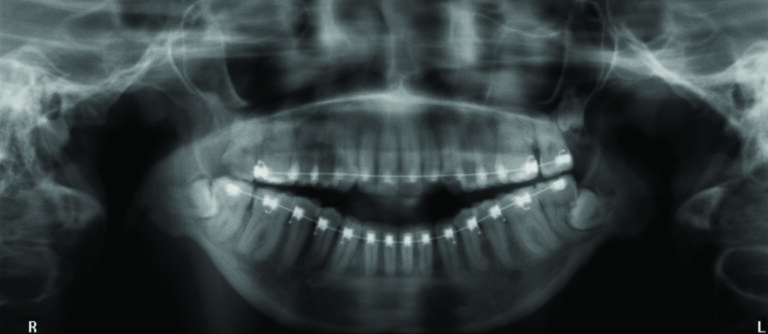
Fig. 4


1. Bilateral TMJ TJR with patient-fitted devices (Fig. 5)
Fig. 5
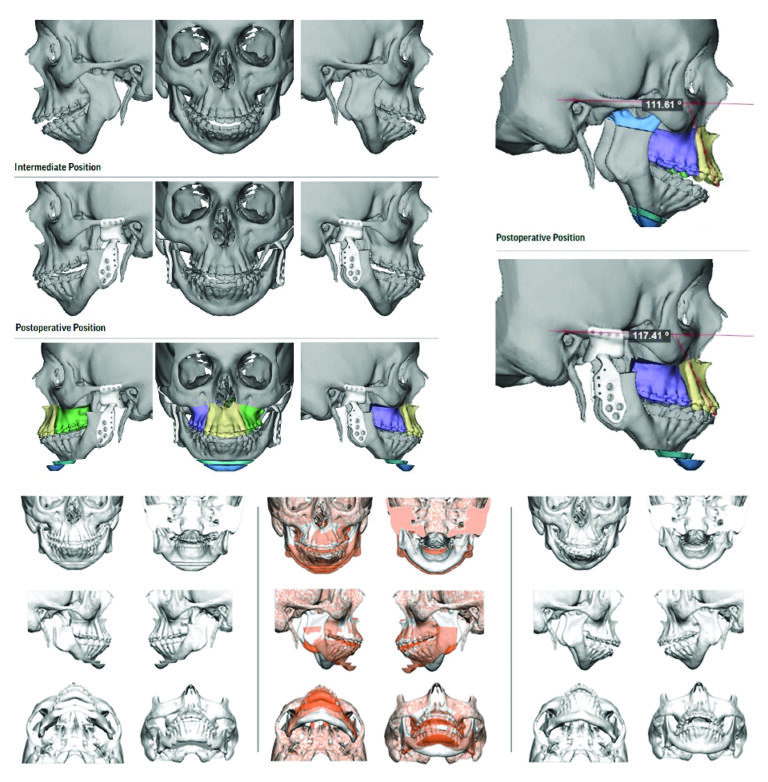
2. Segmental LeFort I maxillary osteotomy for expansion, impaction, advancement, and midline correction
3. Double step advancement genioplasty
4. Counterclockwise rotation of the maxillomandibular complex with advancement of the pogonion by 29mm
At 3 years post-surgery, this patient has maintained a stable skeletal and occlusal relationship, improved facial balance, and improved airway (Figs. 6A&B,7).
Fig. 6A

Fig. 6B
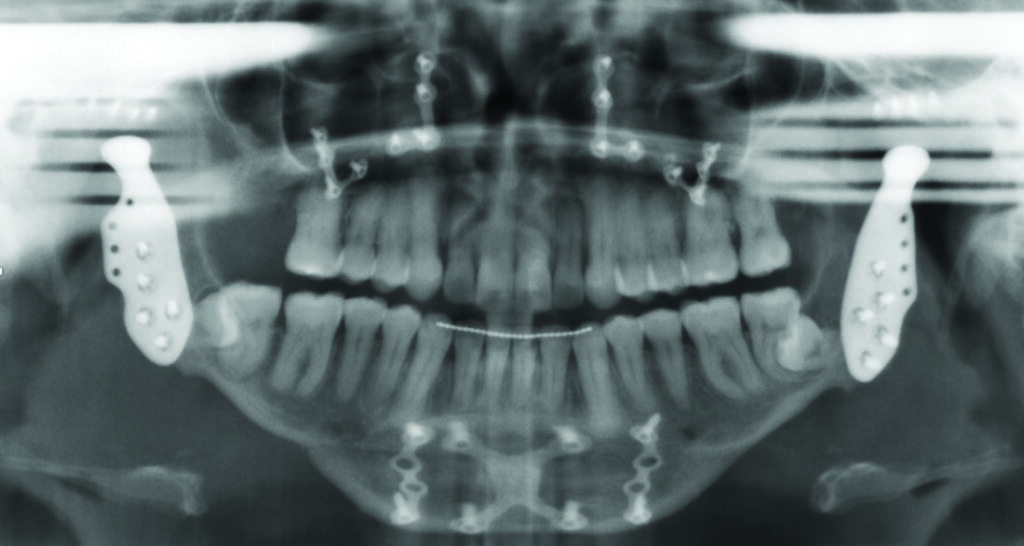
Fig. 7

When evaluating the pre-operative and post-operative results (Figs. 8,9), the obvious change in facial difference, the idealized occlusion, and the improved range of motion obtained by this surgical result, demonstrate that this treatment modality (C-TJR-OGS) contributed to a restored and improved function for this patient with regards to her quality of life, airway and overall subjective satisfaction.
 Fig. 8
Fig. 8
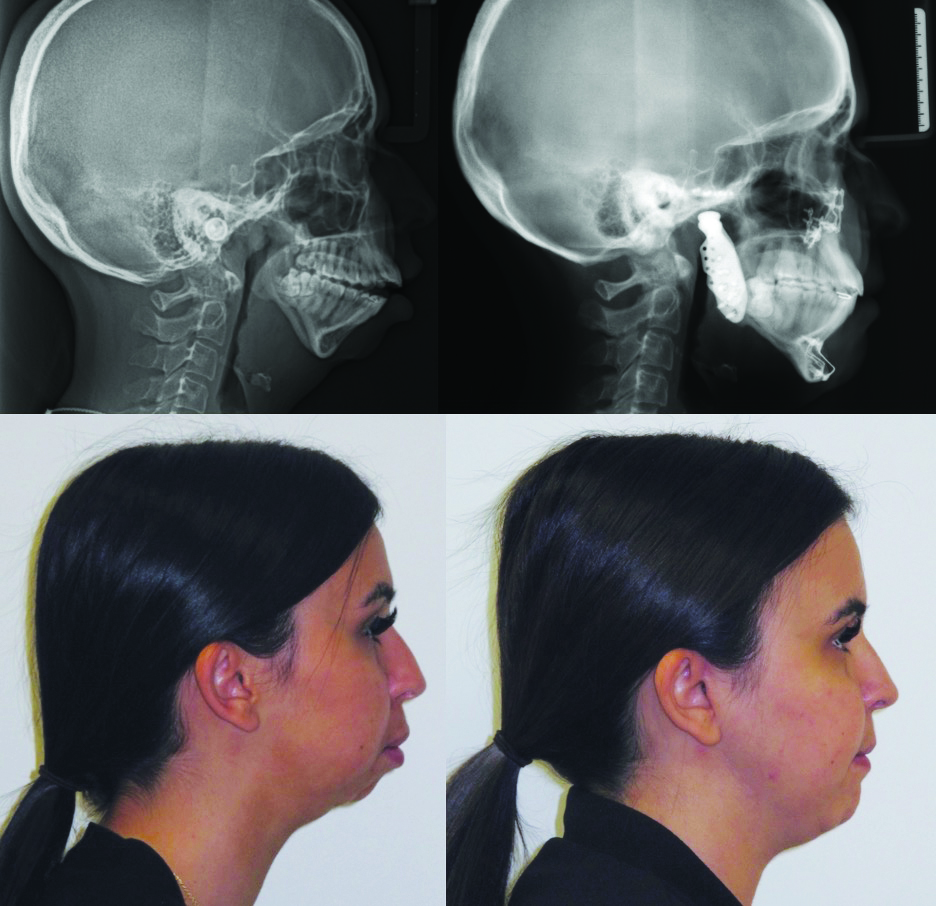
Fig. 9

Oral Health welcomes this original article.
Acknowledgement: Dr. Nick Karaiskos (Orthodontist, Ottawa, ON)
References
- Mercuri LG. Temporomandibular Joint Total Joint Replacement – TMJ TJR: A Comprehensive Reference for Researchers, Materials Scientists, and Surgeons. 1st ed. Cham: Springer International Publishing AG; 2015.
- Wolford L. Concomitant TMJ and OGS: does it really work? International journal of oral and maxillofacial surgery. 2015;44:e18–e18.
- Keefe SH, Keefe MG, Hui B, Pogrel MA. Patient motivation and satisfaction from OGS—a case series. Oral surgery, oral medicine, oral pathology and oral radiology. 2023;135(2):e15–24.
- Quinn PD, Granquist EJ. Atlas of Temporomandibular Joint Surgery. United States: John Wiley & Sons, Incorporated; 2015.
- Wolford LM, Cassano DS, Goncalves JR. Common TMJ disorders: orthodontic and surgical management. In: McNamara JA, Kapila SD, editors. Temporomandibular disorders and orofacial pain: separating controversy from consensus, Craniofacial growth series, vol. 46. Ann Arbor: The University of Michigan; 2009. p. 159–98.
- Peterson’s Principles of Oral and Maxillofacial Surgery. 4th ed. 2022. Cham: Springer International Publishing
- Emmerling MR, Shah B, Ginzburg M. Virtual Surgical Planning in OGS. Current surgery reports (Philadelphia, PA). 2024;12(3):26–35.
- Giannakopoulos HE, Sinn DP, Quinn PD. Biomet Microfixation Temporomandibular Joint Replacement System: A 3-Year Follow-Up Study of Patients Treated During 1995 to 2005. Journal of oral and maxillofacial surgery. 2012;70(4):787–94.
- Wolford LM, Mercuri LG, Schneiderman ED, Movahed R, Allen W. Twenty-Year Follow-up Study on a Patient-Fitted Temporomandibular Joint Prosthesis: The Techmedica/TMJ Concepts Device. Journal of oral and maxillofacial surgery. 2015;73(5):952–60.
- Mercuri LG. Alloplastic temporomandibular joint replacement – past, present, and future: “Learn from the past, prepare for the future, live in the present.” Thomas S. Monson. British journal of oral & maxillofacial surgery. 2024;62(1):91–6.
- Coleta KED, Wolford LM, Goncalves JR, Santos-Pinto A, Pinto LP, Cassano DS. Maxillo- mandibular counter-clockwise rotation and mandibular advancement with TMJ concepts1 total joint prostheses: part I skeletal and dental stability. Int J Oral Maxillofac Surg. 2008;38:126–38.
- Pinto LP, Wolford LM, Buschang PH, Bernardi FH, Goncalves JR, Cassano DS. Maxillo- mandibular counter-clockwise rotation and mandibular advancement with TMJ concepts total joint prostheses: part III pain and dysfunction outcomes. Int J Oral Maxillofac Surg. 2009;38:326–31.
- Bouzid A, Caminiti MF, Tenenbaum H, Psutka DJ. Survivability and Outcomes of Total Temporomandibular Joint Replacement using a single Patient Specific Prosthesis. University of Toronto, Research Day Feb 14th, 2024
- Briceno WX, Milkovich J, El-Rabbany M, Caminiti MF, Psutka DJ. Reconstruction of Large Defects Using Extended Temporomandibular Joint Patient-Matched Prostheses. J Oral Maxillofac Surg. 2022 Jun;80(6):1018-1032.
About the Authors

Ryan J. McCoy, Oral and Maxillofacial Surgeon, Clinical Fellow in Advanced Temporomandibular Joint and OGS, University of Toronto, Toronto, Ontario, Canada.

David J. Psutka, Assistant Professor, Division of Oral and Maxillofacial Surgery, Faculty of Dentistry, University of Toronto; Senior Consulting Oral and Maxillofacial Surgeon, Co-Founder of the Mount Sinai Hospital Center for Excellence in TMJ Reconstructive Surgery; Co-Chair, Fellowship Program in Advanced Temporomandibular Joint and OGS, University of Toronto.

Marco F. Caminiti, Associate Professor, Head and Program Director, Oral and Maxillofacial Surgery, University of Toronto; Co-Chair, Fellowship Program in Advanced Temporomandibular Joint and OGS, University of Toronto; Head of Oral and Maxillofacial Surgery, Humber River Hospital; Surgical Director; Cleft Lip, Palate and Craniofacial Clinic, Holland Bloorview Kids Rehabilitation Hospital.