
Brain abscesses originating from carious teeth represent a rare yet potentially severe condition. Dental caries, if left untreated, can lead to various complications, including the development of brain abscesses due to the proximity of dental structures to the central nervous system. This paper aims to elucidate the pathophysiology, clinical manifestations, diagnostic approaches, treatment modalities, and preventive strategies concerning brain abscesses arising from dental caries.
CASE REPORT
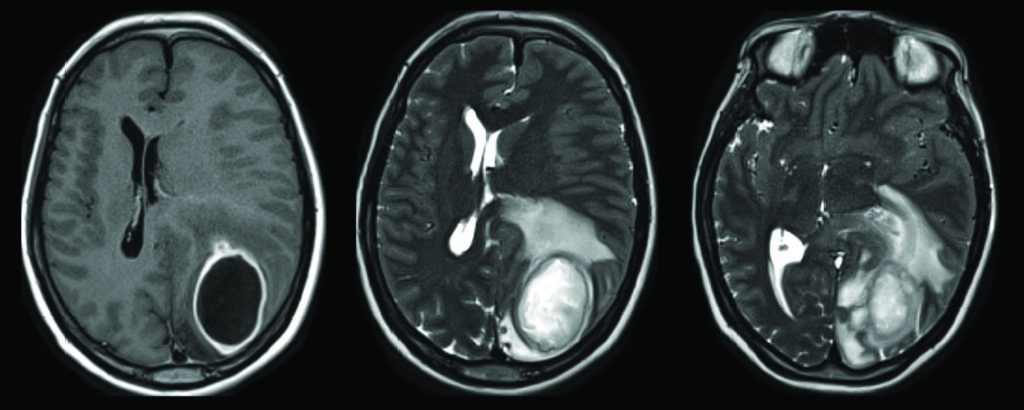
A 30-year-old woman, known as a previous IV drug abuser, presented to the emergency department with blurred vision, a headache and a decreased level of alertness, registering a Glasgow Coma Scale of 11. A computed tomography scan showed a left occipital lesion with extensive perifocal edema and compromise of the visual cortex (Fig. 1 A & B). Magnetic resonance imaging with contrast revealed an underlying parieto-occipital rim-enhancing, centrally necrotic lesion measuring 4.5 x 3.3 cm with surrounding vasogenic edema causing mass effect on the left lateral ventricle and subsequent subfalcine herniation to the right (Fig. 2 A, B & C).
Fig. 1AB
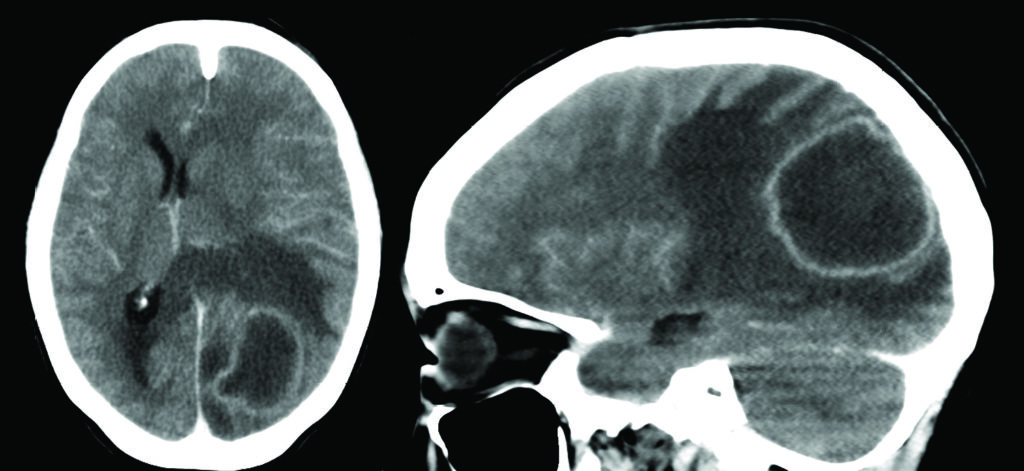
Fig. 2ABC
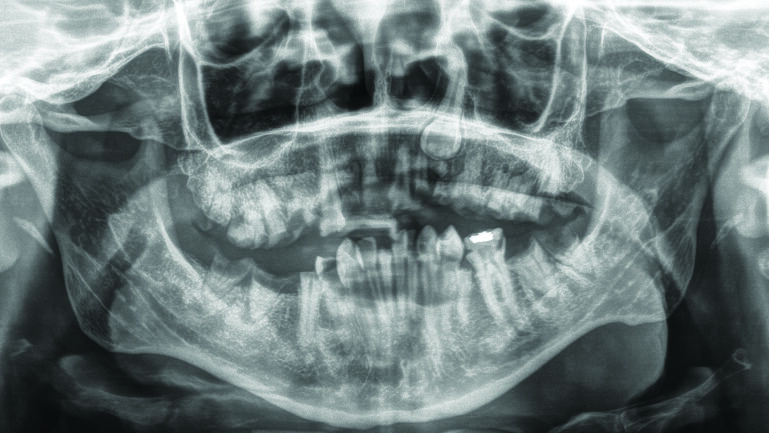
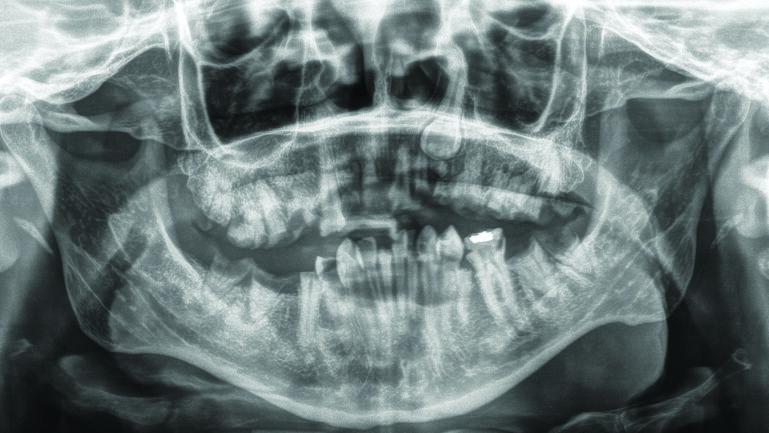
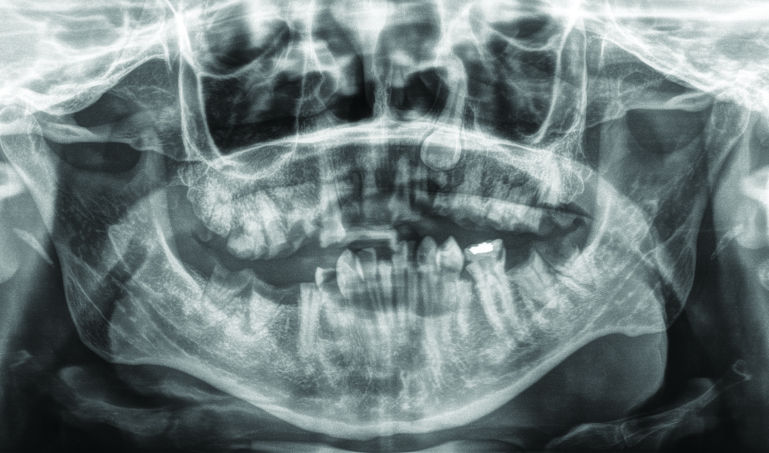
Surgical decompression revealed an intracerebral abscess and cultures of the purulent material were sent to aerobic, anaerobic, and fungal organisms. Anaerobic culture grew rare gram-positive cocci, Streptococcus constellatus, with the patient having a concomitant bacteremia. The panorex x-ray identified numerous carious teeth and retained roots with associated periapical lucencies in the, keeping with a chronic odontogenic infection, necessitating full mouth clearance of the patient’s teeth. (Fig. 3). Her cardiac echo remained unremarkable. The patient was treated with a prolonged course of antibiotics. Post-operatively she returned to her baseline.
Fig. 3
DISCUSSION
PATHOPHYSIOLOGY
The incidence of brain abscesses is 0.3–1.3 per 100,000 people annually, with only 2-5% having an odontogenic origin.1 The pathogenesis of brain abscesses from carious teeth follows a predictable progression. Dental caries, primarily caused by bacterial colonization and enamel demineralization, progress through the tooth structure if not managed adequately.2 As the caries penetrate deeper, they reach the dental pulp, creating an avenue for infection. Bacteria, predominantly Streptococci and anaerobic organisms such as Fusobacterium and Prevotella species proliferate within the pulpal tissue and spread into the surrounding structures, including the periodontium and alveolar bone.3 Almost all periodontal and endodontic dental infections contain anaerobic microbes; aerobic organisms account for less than 5% of odontogenic infections.4
If left untreated, these infections can extend beyond the local oral structures, producing localized abscesses and/or perforations in the bone. The proximity of the oral cavity to the maxillofacial region allows bacteria to infiltrate the bloodstream through the rich network of blood vessels, potentially leading to bacteremia. Once in the bloodstream, bacteria can disseminate to distant sites, including the brain, via hematogenous spread or direct extension through adjacent tissues, causing brain abscess formation.
Research has demonstrated that microorganisms may have reached the peripheral capillary system within a minute of dental procedures. Thus, in very mild mouth manipulations, bacteria can still transfer into the bloodstream.5 Brain abscesses may also result from other infections, such as acute otitis media, mastoiditis, upper respiratory infections, or localized trauma.6
CLINICAL MANIFESTATIONS
The clinical presentation of a brain abscess secondary to dental caries can vary widely and often depends on the size, location, and stage of development of the abscess. Patients may exhibit nonspecific symptoms initially, such as fever, headache, speech difficulties, and malaise.4 More specific neurological signs may manifest as the abscess progresses, including focal neurological deficits depending on location and overall CNS involvement. They may include variable degrees of paresis, speech disturbances, visual alterations, seizures, altered mental status, and signs of increased intracranial pressure, such as vomiting and papilledema.7
However, connecting these neurological symptoms to dental pathology might not always be straightforward, leading to diagnostic challenges and potential delays in appropriate management.
DIAGNOSTIC APPROACHES
Diagnosing a brain abscess originating from dental caries requires a multifaceted approach. The diagnostic process commences with a comprehensive medical history and clinical examination from a physician, with particular emphasis on dental health and any recent occurrences of oral infections or procedures. If the patient notes the presence of gingivitis, periodontitis, cavities, recent tooth extraction and implant placement or prior endodontic treatments, the clinician should be suspicious that the oral cavity may be the source of an abscess.4
Cranial imaging techniques, notably computed tomography (CT) with and without contrast, as well as magnetic resonance imaging (MRI), including T1, T2 flair, DWI/ADC and T1 sequences with gadolinium, are crucial for visualizing the abscess and determining its precise location. MRI is also useful to rule out other pathologies such as neoplastic lesions.4 The location of the abscess can vary widely. The frontal lobe was the most commonly affected lobe at 45.7%, but it can also occur in other areas such as the parietal lobe 19.6% and the temporal and occipital lobes with a similar percentage 13% and 10.9%, respectively.4
Supplementary investigations such as blood cultures, analysis of cerebrospinal fluid, cardiac echo and dental radiographs may be necessary to identify the causative organisms and confirm the dental origin of the infection. As brain and odontogenic infections are often polymicrobial, identifying the pathogens using bacterial culture is essential to obtaining a precise diagnosis.4 Most bacteria involved in brain abscesses of odontogenic origin are anaerobic in a ratio of 3:1 compared to aerobes. The most commonly isolated pathogenic species are from the Milleri family (S.anginosus, S. constellatus and S.intermedius). One review identified this family as the most prevalent in brain abscesses, followed by other pathogens, as Porfiromonas gingivalis.4 However, other less common microorganisms have also been identified in brain abscess cultures, such as Enterococcus faecalis, Actinomycetes, Morganella morgani and Eikenalla corrodens.1,10
TREATMENT MODALITIES
The management of brain abscesses from dental caries typically involves a multidisciplinary approach. The primary goal is to treat the source of infection, followed by clearance of secondary systemic antibiotic treatment. On average, less than half of affected patients recover completely, and a third maintain minor deficiencies (i.e. episodes of vertigo, loss of memory, etc.).8 Prompt and aggressive intervention is necessary to prevent further neurological complications. The combination of surgical drainage via open craniotomy or stereotactic aspiration, intravenous antibiotics for at least six weeks, and repeat cranial CT or MRI imaging is considered the gold standard of care for a brain abscess.1 Neurosurgical interventions are indicated for intracerebral abscesses in inaccessible areas measuring more than 2-2.5 cm to evacuate the purulent material, aiming to reduce bacterial load and intracranial pressure and establish adequate drainage.
Antibiotics, selected based on the likely causative pathogens and susceptibility patterns, are administered empirically and subsequently tailored according to culture and sensitivity results. A combination of IV vancomycin, ceftriaxone, and metronidazole are most used.1 Supportive care and rehabilitation may also be necessary to address neurological deficits and aid in the patient’s recovery.
Dental care must be provided as soon as the patient’s health permits following the diagnosis of dental etiology. Most often, this involves a tooth extraction. Due to the risk of further bacterial dispersion, a multidisciplinary medical team must choose the ideal time to initiate this treatment.4
PREVENTIVE STRATEGIES
Preventing brain abscesses originating from dental caries primarily revolves around maintaining optimal oral hygiene and seeking timely dental care. Emphasizing the importance of regular dental check-ups, prompt treatment of dental caries, and adherence to oral hygiene practices such as brushing, flossing, and mouth rinses can significantly reduce the risk of oral infections progressing to systemic complications.9,11
Educating both healthcare professionals and the general public about the potential consequences of untreated dental disease on systemic health is paramount in preventing such serious complications.
Brain abscesses arising from dental caries represent a rare but critical condition that requires timely recognition and management. Understanding the pathophysiology, clinical manifestations, diagnostic approaches, treatment modalities, and preventive strategies are crucial steps in mitigating the risk and burden of this potentially life-threatening complication. Collaboration between dental and medical professionals, coupled with patient education and awareness, plays a pivotal role in preventing the progression of dental infections to more severe systemic complications, including brain abscesses. Moving forward, continued efforts in public health education, reinforcement of preventive dentistry, and interdisciplinary collaboration are essential to anticipate the risk of such devastating complications, especially in remote areas with limited access to dental care. 
Oral Health welcomes this original article.
References
- Hsu G, et al. Do brain abscesses have a higher incidence of odontogenic origin than previously thought? Oral Surg Oral Med Oral Pathol Oral Radiol. 2020;130(1):10-7.
- Rathee M, Sapra A. Dental Caries. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.; 2024.
- Radaic A, Kapila YL. The oralome and its dysbiosis: New insights into oral microbiome-host interactions. Comput Struct Biotechnol J. 2021;19:1335-60.
- Burgos-Larraín LF, et al. Brain complications from odontogenic infections: A systematic review. J Stomatol Oral Maxillofac Surg. 2022;123(6):e794-e800.
- Corson MA, Postlethwaite KP, Seymour RA. Are dental infections a cause of brain abscess? Case report and review of the literature. Oral Dis. 2001;7(1):61-5
- Muzumdar D, Jhawar S, Goel A. Brain abscess: an overview. Int J Surg. 2011;9(2):136-44.
- Dorsett M, Liang SY. Diagnosis and Treatment of Central Nervous System Infections in the Emergency Department. Emerg Med Clin North Am. 2016;34(4):917-42.
- Kichenbrand C, et al. Brain abscesses and intracranial empyema due to dental pathogens: Case series. Int J Surg Case Rep. 2020;69:35-8.
- Veiga N, et al. of Primary Clinical Prevention of Dental Caries in the Adult Patient: An Integrative Review. Healthcare (Basel). 2023;11(11).
- Maraby-Salgado, et al. Brain Abscess and Dental Infections. A review. Romanian Neurosurgery. 2018;32(2)283-289.
- Brady P, et al. Intra cranial abscess secondary to dental infection. Journal of The Irish Dental Association, 60 (1):35-37, 2014.
About the Authors

Ms. Pynn is a 1st year medical student at Northern Ontario School of Medicine, previously completing a Bachelors of Science (Honours) at Queen’s University. Emily has been involved in research that explores the inequalities of underprivileged populations.

Dr. Lohkamp is a neurosurgeon at Thunder Bay Regional Health Sciences Center and an Assistant Professor at the Northern Ontario School of Medicine.

Dr. Bharathidasan is a staff anesthesiologist, Assistant Professor in the Department of Anesthesia at the Thunder Bay Regional Health Sciences Centre. He sub-specializes in Neuro anesthesia, Perioperative anesthesia and has special interest in Point of Care Ultrasound.

Dr. Pynn is Oral Health’s editorial board member for oral and maxillofacial surgery. He is an Assistant Professor, North Ontario School of Medicine, Lakehead University, and Chief of Dentistry, Thun-der Bay Regional Health Sciences Center.