
Study the past, if you would divine the future — Confucius
The Endodontic Implant Algorithm — provides highlights in the assessment and identification of determinant factors leading to endodontic failures, in order to help in the decision making process whether or not it is adequate to implement an new endodontic approach vs. extraction and replacement with dental implants — Confusion
Over the years, endodontics has diminished itself by enabling the presumption that it is comprised of a narrowly defined service mix; root canal therapy purportedly begins at the apex and ends at the orifice. Nothing could be further from the truth. It is the catalyst and precursor of a multivariate continuum, potentially the foundational pillar of all phases of any rehabilitation [Figs 1a, 1b, 1c]. Early diagnosis of teeth requiring endodontic treatment, prior to the development of periradicular disease, is critical for a successful treatment outcome (1). Esthetics, function, structure, biologics and morphology are the variables in the equation of optimal oral health. Interventional or interceptive endodontics, restorative endodontics, the re-engineering of failing therapy, transitional endodontics and surgical endodontics encompass a vast scope of therapeutic considerations prior to any decision/tipping point to replace a natural tooth. Everything we do as dentists is “transitional”, with the exception of extractions. No result is everlasting, none are permanent; thus our treatment plans must reflect this reality. Artifice versus a natural state is not a panacea for successful treatment outcomes [Fig 2a, 2b, 2c, 2d].
In 1992, funding from the Cochrane Collaboration was obtained for a UK Cochrane Center based in Oxford to facilitate the preparation of systematic reviews of randomized trials of health care (2). The Cochrane Systematic Review is a process that involves locating, appraising, and synthesizing evidence from scientific studies in order to provide informative empirical answers to scientific research questions. In 1952, the enterprising son of an inventor named Ron Popeil created infomercials using 30 to 120 second television spots to sell his inexpensive array of useful products, including the Pocket Fisherman and the Veg-O-Matic food slicer. The singular goal of an infomercial was to get the viewer to a phone immediately and have them place their order. No waiting weeks, months or even years for the lofty marketing goals of branding to pay off. Somewhere along the way, dentistry morphed the two concepts. Nowhere is this becoming more apparent than in the debate on the endodontic implant algorithm. “We have met the enemy… and he is us”…..The Pogo Papers.
Scientific doctrine is the cornerstone of Endodontic therapeutics. However, of late, anecdotal testimony has become the default setting for new paradigms to justify endodontic treatment modalities and an encomium to technologic advances. The strength of the arch of this or any specialty’s integrity and relevance must rely on a keystone of randomized clinical trials and evidence-based treatment outcomes. Expert opinions reflected through the looking glass of business models or global tours cannot replace stringently controlled clinical assessments distilled from exacting independent investigations. Science cannot be applied through a McLuhanistic rearview mirror of technology. The two must symbiotically occupy the same space regardless of whether that is antithetical to the Pauli Exclusion Principle, one of the most accepted laws of physics; no two objects can simultaneously occupy the same space.
In December 2004, Salehrabi and Rotstein (3) published an epidemiological study on endodontic treatment outcomes in a large patient population. The outcomes of initial endodontic treatment done by general practitioners and endodontists participating in the Delta Dental Insurance plan on 1,462,936 teeth of 1,126,288 patients from 50 states across the USA were assessed in an eight year timeline. 97% of teeth were retained in the oral cavity subsequent to nonsurgical endodontic treatment over this period. The combined incidence of untoward events such as retreatments, apical surgeries, and extractions was 3% and occurred primarily within 3 years from the completion of treatment. Analysis of the extracted teeth revealed that 85% had no full coronal coverage. A statistically significant difference was found between covered and uncovered teeth for all tooth groups tested which is consistent with the findings from numerous investigations (4, 5, 6).
The purpose of this publication is to evaluate current trends and perceptions pertaining to the standard of care in endodontics and provide an evidence based consensus on their relevance and application. Part II will address the algorithm by which sacrifice of natural structures for orthobiologic replacements can be validated and the engineering principles and designs that best mimic clinical dictates.
Three surveys have been conducted with the membership of the American Association of Endodontists since the late 1970’s. The first reflected what is now an anachronistic view of emergency procedures and the standard of care defining non-surgical therapy during that period (7); the second, done prior to the technologic advances of the last decade of the twentieth century, was hallmarked by a dramatic decrease in leaving pulpless teeth open in emergency situations and a significant decline in the use of culturing prior to obturation (8). The report indicated that the concept of “debridement and disinfection” versus “cleaning and shaping” was now the focus of the biologic therapeutic imperative and the need for expansive microbial strategies was recognized as being of paramount importance [Fig 3]. The primary patho-physiologic vectors of pulpal disease and the myriad complexity of the root canal system had always been understood; as the century closed, clinicians were provided with new tools and technology to expand the boundaries and limitations of endodontic treatment procedures [Figs 4a, 4b].
Root canal infections are polymicrobic, characterized predominantly by both facultative and obligate anaerobic bacteria (9).The necrotic pulp becomes a reservoir of pathogens, toxic consequences and their resultant infection is isolated from the patient’s immune response. Eventually, the microflora and their by-products will produce a periradicular inflammatory response. With microbial invasion of the periradicular tissues, an abscess and cellulitis may develop. The resultant inflammatory response will initiate either a protective and/or immunopathogenic effect; additionally, it may destroy surrounding tissue resulting in the five classic signs and symptoms of inflammation; calor, dolor, rubor, tumor and penuria. Patient evaluation and the appropriate diagnosis/treatment of the source of an infection are of utmost importance.
Patients demonstrating signs and symptoms associated with severe endodontic infection (Table I) should have the root canal system filled with calcium hydroxide and the access sealed. In the event of copious drainage, the access can be left open for no longer than 24 hours, the tooth then isolated with rubber dam, the canals irrigated and dried and calcium hydroxide inserted into the root canal space and the access sealed (10). The antibiotic of choice for periradicular abscess remains Penicillin VK; however, recent studies have reported that amoxicillin in combination with clavulinate (1gm loading dose with 500mg q8h for 7 days) was a more effective therapeutic regimen (11).
Systemic antibiotic administration should be considered if there is a spreading infection that signals failure of local host responses in abating the dispersion of bacterial irritants, or if the patient’s medical history indicates conditions or diseases known to reduce the host defense mechanisms or expose the patient to higher systemic risks. Antibiotic treatment is gener
ally not recommended for healthy patients with irreversible pulpitis or localized endodontic infections (Table II). Numerous studies with well-defined diagnosis and inclusion criteria failed to demonstrate enhanced pain resolution beyond the placebo effect (12, 13).
The sophistication of endodontic equipment, materials and techniques has been steadily iterated and innovated since the second survey. The microscope first introduced to otolaryngology around 1950, then to neurosurgery in the 1960’s, is now standard of care for the voyage into the microcosmic world of the root canal system. Recursions in the micro-processing technologies of electronic foramenal locators begat unprecedented accuracy levels, improved digital radiographic sensors and software enhanced diagnostic acumen, and ultrasonic units with a variety of tips designed specifically for use when performing both nonsurgical and surgical endodontic procedures minimized damage to coronal and radicular tooth structure in the effort to locate the pathways of the pulp. The treatment outcome of non-surgical root canal therapy at this point in time is far more predictable than at any other period in our history.
Of all the technologic innovations embraced by endodontics, digital radiography should have generated the greatest impact; however, its value remains limited in diagnosis, treatment planning, intra-operative control and outcome assessment. Flat field sensors still require 3 to 4 parallax images of the area of interest to establish better perception of depth and spatial orientation of osseous or dental pathology. These three-dimensional information deficits, geometric distortion and the masking of areas of interest by overlying anatomy or anatomic noise are of strategic relevance to treatment planning in general and in endodontics specifically (14)[Figs. 5a, 5b].
Cone beam computed tomography (cbCT) produces up to 580 individual projection images with isotropic submillimeter spatial resolution enhanced by advanced image receptor sensors; it is ideally suited for dedicated dento-maxillofacial CT scanning. When combined with application-specific software tools, cone beam computed tomography can provide a complete solution for performing specific diagnostic and surgical tasks. The images can be resliced at any angle, producing a new set of reconstructed orthogonal images and studies have shown that the scans accurately reflect the volume of anatomic defects. The limited volume cbCT scanners best suited for endodontics require an effective radiation dose comparable to two or three conventional periapical radiographs and as such are set to revolutionize endodontics (15, 16) [Fig 6].
Three dimensional pre-surgical assessment of the approximation of root apices to the inferior dental canal, mental foramen and maxillary sinus are essential to treatment planning. The ability of cbCT to diagnose and manage dento-alveolar trauma using multiplanar views, the determination of the root canal anatomy and the number of canals, the detection of the true nature and exact location of resorptive lesions and the discovery of the existence of vertical and horizontal fractures outweigh concerns about the degree of ionizing radiation and the risks posed (17). Provided cbCT is used in situations where the information from conventional imaging systems is inadequate, the benefits are essential for optimization of the standard of care.
Patel reported that periapical disease can be detected sooner and more accurately using cbCT compared with traditional periapical views and that the true size, extent, nature and position of periapical and resorptive lesions can be accurately assessed (18). Using a new periapical index based on cone beam computed tomography for identification of apical periodontitis, periapical lesions were identified in 39.5% by radiography and 60.9% of cases by cbCT respectively (P < .01). Simon et al compared the differential diagnosis of large periapical lesions with traditional biopsy. The results suggested that cbCT might provide a faster method to differentially diagnose a solid from a fluid-filled lesion or cavity, without invasive surgery (19, 20). In spite of the presence of artifacts, the learning curve related to image manipulation and the cost, cone beam tomography will invariably be the accepted standard of diagnostic care and treatment planning in endodontics in the very near future.
An improperly designed access cavity will hamper facilitation of optimal root canal therapy. If the orientation, extension, angulations and depth are inaccurate, retention of the native anatomy of the root canal space becomes precarious. The requirements of access cavity design can be achieved by conceptual and technical regression of the existing configuration to that which one would logically expect to have seen prior to the insults of restoration, function and aging. If tertiary dentin were perceived of as “irritational dentin” or dystrophic calcification considered “decay”, the chamber outline could be used to blueprint an inlay configuration for the access design that literally replicates the “virgin” tooth (Fig 7).
Removal of the existing restoration in its entirety and/or preliminary preparation of the coronal tooth structure for the subsequent full coverage restoration will identify decay, fractures, unsupported tooth structure and expose the anatomy of the underlying root trunk periphery which assists in discovery of the spatial orientation and morphology of the roots. The pulp chamber ceiling and pulp stones can be peeled away with a football diamond bur to grossly identify the primary orifices. Micro-etching (Danville Materials, San Ramon CA) the floor of the chamber, perhaps the most underused of all access tools, is invaluable in the exposure of fusion lines and grooves in order to identify accessory orifices. Troughing with ultrasonic tips of any design is used solely to trace fusion lines, not effect gross removal. The use of ultrasonics to “jackhammer” pulp stones is simply too risky as one approaches the floor of the chamber, particularly if there are no water ports on the tips. Orifice lengthening and widening enables straight line glide path to the apical third. The strategic objective is not to impede the file, stainless steel or nickel-titanium rotary along the axial walls with minimal dentin removal [Figs 8a, 8b].
It is equally as important to produce a high quality coronal restoration at the time of sealing the root canal system (21, 22). Despite research supporting the effectiveness of coronal barriers and the need for their immediate placement as a component of the completion phase of root canal treatment, a universally accepted protocol does not exist. Schwartz and Fransman have described a clinical strategy for coronal sealing of the endodontic access preparation that lists the following considerations in the protocol; use bonded materials [4th generation (three step) resin adhesive systems are preferred because they provide a better bond than the adhesives that require fewer steps], the “etch and rinse” adhesives are preferred to “self etching” adhesive systems if a eugenol containing sealer or temporary material is used, “self etching” adhesives should not be used with self-cure or dual-cure restorative composites, when restoring access cavities, the best esthetics and highest initial strength are obtained with an incremental fill technique with composite resin, a more efficient technique which provides acceptable esthetics is to bulk fill with a glass ionomer material to within 2 to 3 mm of the cavo-surface margin, followed by two increments of light-cure composite and if retention of a crown or bridge abutment is a concern after root canal treatment, post placement increases retention to greater than the original state (23) [Fig 9].
The complex anatomy of the root canal space presents a daunting challenge to the
clinician who must debride and disinfect the corridors of sepsis with absoluteness to achieve a successful treatment outcome [Fig 10]. In addition, the absence of a cell-mediated defense (phagocytosis, a functional host response) in necrotic teeth means the microorganisms residual in tubuli, cul de sacs and arborizations are mainly affected by the redox potential (reduction potential reflects the oxidation-reduction state of the environment — aerobic microflora can only be active at a positive Eh, whereas strict anaerobes can only be active at negative Eh values) and availability of nutrients in the various parts of the root canal (24). While our knowledge of persistent bacteria, disinfecting agents and the chemical milieu of the necrotic root canal has greatly increased, there is no doubt that more innovative basic and clinical research is needed to optimize the use of existing methods and materials and develop new ones in order to prevent and/or treat apical periodontitis.
Varying degrees of sterility of the root canal space are achieved by mechanistic removal, the chemical reactivity and fluid dynamics of irrigants and their introduction to the canal space; however, the protocols used today cannot predictably provide sterile canals. As none of the elements of endodontic therapy (host defense system, systemic antibiotic therapy, instrumentation and irrigation, inter-appointment medicaments, permanent root filling, and coronal restoration) can alone guarantee complete disinfection, it is of utmost importance to aim at the highest possible quality at every phase of the treatment. In the classic study by Sjogren et al, 55 single-rooted teeth with apical periodontitis were instrumented and irrigated with sodium hypochlorite and root filled. Periapical healing was followed-up for 5 years. Complete periapical healing occurred in 94% of cases that yielded a negative culture. Where the samples were positive prior to root filling, the success rate of treatment was just 68%- a statistically significant difference. These findings emphasize the importance of completely eliminating bacteria from the root canal system prior to obturation. This objective cannot be reliably achieved in a one-visit treatment of necrotic pulps because it is not possible to eradicate all infection from the root canal without the support of an inter-appointment antimicrobial dressing (25).
NaOCl is the most widely used irrigating solution. It is a potent antimicrobial agent and lubricant which effectively dissolves pulpal remnants and organic components of dentin thus preventing packing infected hard and soft tissue into the apical confines. Hypochlorous acid (HClO) is the active moiety responsible for bacterial inactivation. NaOCl is used in concentrations varying from 0.5%to 5.25%; the in vitro and in vivo studies differ significantly in terms of the effectiveness of the range of concentrations as the in vitro experiments provide direct access to microbes, higher volumes are used and the chemical milieu complexity of the natural canal space are absent than in the in vivo experimentation. A study by Siqueira et al (26) showed no difference (in vitro) between 1%, 2.5% and 5% NaOCl solutions in reducing the number of bacteria during instrumentation. What has been shown is that the tissue dissolving effects are directly related to the concentration used (27).
Perhaps the most misunderstood aspect of NaOCl irrigation is the need for the quantities of irrigation required due to the morphologic and anatomic variations in the volumetric size of the root canal anatomy. Siqueira showed that regular exchange and the use of large amounts of irrigant should maintain the antibacterial effectiveness of the NaOCl solution, compensating for the effects of concentration (28). Numerous devices have appeared in the endodontic armamentarium to address this situation; EndoVac (Discus Dental) — a negative pressure differential device designed to deliver high volumes of irrigation solution while using apical negative pressure through the office high volume evacuation system, Negative Pressure Safety Irrigator (Vista Dental, Racine WI) — device is similar to EndoVac, Rinsendo (Air Techniques, Corona CA) uses pressure suction technology; 65 ml of irrigant are automatically drawn from the attached syringe and aspirated into the canal [pressure created is lower than manual irrigation], VIbringe (Bisco Canada, Richmond BC) — sonic flow technology facilitates enhanced irrigation through the myriad complexities of the root canal system [Fig 11].
NaOCl cannot dissolve inorganic dentin particles and thus prevent smear layer formation during instrumentation (29). Chelators such as EDTA and citric acid are recommended as adjuvants in root canal therapy. It is probable that biofilms are detached with the use of chelators; however, they have little if any antibacterial activity. Several studies have shown that citric acid in concentrations ranging as high as 50% was more effective at solubilization of inorganic smear layer components and powdered dentin than EDTA. In addition, citric acid has demonstrated antibacterial effectiveness.
Technology and innovation will not negate the need for optimal preparation (debridement and disinfection) to eliminate microbial content and its impact on a necrotic root canal system. We as a discipline need to be better; however, by the same token, endodontics has shown its commitment to endless reinvention. In time, that will restructure the role of natural teeth in foundational dentistry, currently diminished by the market forces of implant driven dentistry. Orthobiologic replacement is not a panacea as random clinical trials increasingly show; the severity of peri-implantitis lesions demonstrates significant variability and as such no treatment modality has shown superiority. The pendulum will continue to swing as the endodontic implant algorithm becomes increasingly multivariate.
Steven Covey is known for his book The Seven Habits of Highly Effective People. The habit most applicable to endodontics is the second one; Begin with the End in Mind. The implication of this vision in regard to idealizing the final shape of the root canal system to ensure that the obturation represents a totality is profound. The root canal is negative space and as such recovery of its original unaffected form is the sine qua non of obturation or more descriptively — microstructural replication.
Perhaps the most significant example of negative space recovery is Michelangelo’s statuary for the funerary of Pope Julius II. Four unfinished sculptures speak eloquently to this process: the figure was outlined on the front of the marble block and then Michelangelo worked steadily inwards from this side, in his own words ‘liberating the figure imprisoned in the marble’. This is an exacting description of debridement and instrumentation of the root canal space prior to root filling after a myriad of pathologic vectors have destroyed the dental pulp, and altered the morphology/topography of the system [Fig 12].
Incomplete filling of the debrided and sculpted root canal space is one of the major causes of endodontic failure (30). Until recently, in vitro testing (dye leakage, fluid transport, bacterial penetration, glucose leakage) was used to evaluate the sealing efficacy of endodontic filling materials and techniques by assessing the degree of penetration/absorbance of these tracers (31, 32, 33). Unfortunately, leakage studies are limited static models that do not simulate the conditions found in the oral cavity (temperature changes, dietary influences, salivary flow). Given the historic dominance of in vitro testing, the clinician must be cautious when extrapolating study findings to the clinical situation, regardless of manufacturer’s claims (34). This reliance on invalid testing protocols diminishes the “mono-block” assertions applied to the new generation of adhesive obturating materials proposed as the “replacement material” for gutta-percha
(35).
Gutta-percha was introduced to dentistry by Edwin Truman in 1847(36). The concept of thermo-labile vertical condensation of gutta-percha was originally described by Dr. J. R. Blaney in 1927(37). The defining article on obturation remains Dr. Schilder’s classic on filling the root canal space in three dimensions published some forty years later (38). Logically, one cannot physically fill the root canal in two dimensions; however, one can fill the root canal space badly, in three dimensions. This does not critique Dr. Schilder’s exposition, but it does demonstrate that words can easily be misconstrued and alter perspective once they become, as Kipling said, ‘the most powerful drug of mankind’. Ironically, Schilder’s article came seven years prior to his treatise on cleaning and shaping the root canal system which even to this day remains the iconic standard for the technical imperatives associated with instrumentation.
The Washington Study by Ingle indicated that 58% of treatment failures were due to incomplete obturation (39). The corollary is obvious; teeth that are poorly obturated are invariably poorly debrided and disinfected. Procedural errors such as loss of working length, canal/apical transportation, perforations, loss of coronal seal and vertical root fractures have been shown to adversely affect the integrity of the apical seal (40, 41). The Toronto study evaluating success and failure of endodontic treatment at 4 to 6 years after completion of treatment showed that teeth treated with a flared canal preparation and vertical condensation of thermolabile gutta-percha had a higher success rate when compared with step-back canal preparation and lateral compaction. Highlighting the vertical condensation of warm gutta-percha obturation technique as a factor influencing success and failure simply confirmed a perspective evident to most endodontists from years of clinical empiricism.
There is a never ending array of obturation materials, delivery systems and sealers appearing in the marketplace. Each is hallmarked by proprietary modifications and each is heralded as the most significant iteration in obturation since the previous one; today, we practice with a sad truism — marketing is inexorably directing science. However, gutta-percha in combination with a myriad of sealers and solvents remains the primary endodontic obturating material. The dominant systems remain carrier based obturation (Thermafil — Tulsa Dental Specialties, Tulsa OK), Continuous Wave Compaction Technique (Elements Obturation — Sybron Endo, Orange CA and Thermoplastic Injection (Obtura III Max — Obtura Spartan, Earth City MO).
Resilon (RealSeal — SybronEndo Corp., Orange, CA), a high performance industrial polyurethane was developed as an alternative to gutta-percha. There are scattered studies that show Resilon exhibits less microbial leakage (42) and higher bond strength to root canal dentin (43), reduced periapical inflammation (44) and enhanced fracture resistance of endodontically treated teeth when compared with gutta-percha (45) [Fig 13]. Other studies have reported undesirable properties associated with Resilon including low push-out bond strength (46) and low cohesive strength plus stiffness (47). In addition, Resilon could not achieve a complete hermetic apical seal (48). These results indicate that a more appropriate material for root canal obturation still needs to be developed. There is still no obturation method or material that produces a leakproof seal. A material that is bio-inductive and promotes regeneration, a “smart” nano-material that can adapt to the ever-changing microenvironment of the canal system is essential, but todate, remains elusive.
All polymers demonstrate melt temperature and flow rate. Both gutta-percha and Resilon demonstrate demonstrate a viscoelastic gradient that manifests as a dynamic rheological birefringence in the molded state. Dependent upon the molecular weight of the source material (without the opacifiers, waxes and modifiers), gravimetric measurements the time-temperature-transformation diagram of any molding compound can be constructed. In the thermoplastic world of today, this has engendered an increase in the weight of the mass of obturating material and an improvement in the bacterial seal. This applies to carrier based obturation techniques, Continuous Wave Compaction Technique and Obtura III obturation without cone placement.
The steps required for debridement and disinfection of the root canal space are sequential and interdependent. Aberration of any node in the process impacts upon the others leading to iatrogenic damage and potentially, treatment outcome failure. The most common distortion of native anatomy is ledging; canal curvature exceeding 20o was shown to produce ledging of mandibular molars in a cohort of undergraduate students 56% of the time (49). Dentin chips pushed apically by instrumentation incorporated with fragments of pulp tissue will compact into the apical third and the foramenal area causing blockage, altering the working length due to the loss of patency [Figs 14a, 14b].
Apical patency is a technique in which the minor apical diameter of the canal is maintained free of debris by recapitulation with a small file through the apical foramen (50). The most predictable method is to regularly use a designated patency file throughout the cleaning and shaping procedure in conjunction with copious irrigation. A #.08 K-file passively moved through the apical terminus without widening it is most effective; it will refresh the NaOCl at the terminus as the action of the file going to the point of patiency produces a fluid dynamic. Regrettably, loss of working length remains a common adverse event during endodontic therapy, especially among less experienced clinicians. Its major cause is the formation of an apical dentin plug. Therefore, establishing apical patency is recommended even during treatment of canals with vital pulps (51).
Historically, numerous techniques have been advocated for canal preparation (balanced force, anti-curvature, double-flare, modified double-flare); however, step-back (52) and crown-down (53) are the most universally accepted. Experience has shown that a crown-down preparation will cause fewer procedural errors (apical transportation, elbow formation, ledging, strip perforation, instrument fracture). The preliminary removal of coronal dentin (pre-enlargement — treating the apex last) minimizes blockage and enables an increasing volume of irrigant penetration thereby sustaining working length throughout the procedure (54).
The balanced force shaping philosophy is integral to the crown-down approach. Its premise is that instruments are guided by the canal structure when rotational/anti-rotational motion (watch-winding) is used. Changing the direction of rotation controls the probability that instruments will become overstressed and thus ensures that the cutting of structure occurs most efficiently (55). Endodontists have long appreciated what the science reported, that the balanced-force hand instrumentation technique produced a cleaner apical portion of the canal than other techniques [Fig 15] (56, 57). As will be discussed shortly, this author remains committed to hand filing in order to refine apical third shaping and creating an enhanced apical control zone taper.
Two distinct phases are required for the preparation of canals with nickel titanium (NiTi) rotary files. It is essential, that no matter the protocol used, a reservoir of NaOCl must be maintained and replenished repeatedly in the strategically extended access preparation. The coronal portion of the canal space is explored with small sized K-files to establish a glide path for the rotaries to follow. The taper of NiTi files, regardless of manufacturer induces a crown-down effect in the straight portion of the canal. After the coronal and middle third segments are opened and repeatedly irrigated with NaOCl, a sequence of small K-files can progress apically, ultim
ately defining patency, confirming the topography of the accessible canal space and its degree of curvature.
A second “wave” with the NiTi rotaries is then used to effect deep shape approximating the working length and depending upon the configuration of the apical third, to enlarge the terminus to the gauged apical size and initiate the taper of the apical control zone (58). This is a basic concept. It is inherent in all templated protocols that each tooth is different and modifications to the process are always necessary as a function of the tooth morphology and type being treated.
The apical control zone is defined as a matrix like region created at the terminus of the apical third of the root canal space. The zone demonstrates an exaggerated taper from the spatial position determined by an electronic foramenal locator to be the minor apical diameter. Whether this is linear or a point determination is a function of histopathology. The enhanced taper at the terminus creates a resistance form against the condensation pressures of obturation and acts to prevent excessive extrusion of filling material during thermo-labile vertical compaction.
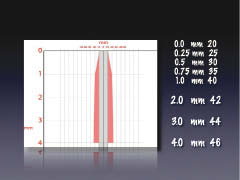
All NiTi systems are modeled upon a single or multiple taper ratio per millimeter of file length. Fig 16a demonstrates the metrics of the F1, F2, F3 finishing files of the ProTaper Universal system (author’s preference). These files demonstrate a common taper in the last 4 mm of the file which in the vast majority of situations corresponds to the length of the apical third of the root canal space. As shown, the .07 taper of the F1 (.20 tip), the .08 taper of the F2 (.25 tip) and the .09 taper of the F3 (.30 tip) produce the corresponding diametral dimension indicated each millimeter back from the apical terminus if the crown down protocol built into this multiple taper file system is adhered to. If the shape of the internal micro-morphology of the root complex were epidemiologically similar, then “imprinting” of the canal preparation would be logical. Unfortunately, such is not the case (59).
Fig 16b shows how the use of hand files in the apical third can alter the preliminary shape created by the NiTi files. Hand files have a .02 taper (along the shaft of the file, the diameter increases by .02 mm per mm of length — .20 file with 16 mm of flutes would be measure .52 mm at the coronal end of the flutes). In the example shown, a #20 file is positioned at the minor apical diameter. Careful positioning of a series of file within the last mm can produce a .2 mm or 20% taper with no undue disruption of the native anatomy. Schilder’s precept for shaping was to keep the apical foramen as small as practically possible. Whatever file approximates the minor apical diameter, in conjunction with hand filing, the apical control zone created will enhance the apical seal as the rheologic vectors of compaction and condensation have a greater lateral volume of displacement at the terminus.
If the biologic parameters that mandate endodontic success are adhered to, in almost all cases, treatment outcomes will be successful. The endodontic implant algorithm processes the array of contributing factors leading to endodontic failure, in order to determine whether to implement a re-engineered endodontic approach or to extract and replace the natural tooth with an osseo-integrated implant. It finds the greatest common divisor among the degree of coronal breakdown of the involved or adjacent teeth, the quality and quantity of the bone support and tissue condition, the engineering demands to be born by the tooth or teeth in question and assesses the occlusal scheme and the patient’s aesthetic and functional expectations of treatment.
The reasons for tooth extraction may include, but are not limited to, crown to root ratio, remaining root length, periodontal attachment levels, furcation status, periodontal health of teeth adjacent to the proposed fixture site and non-restorable carious destruction. In addition, the clinician must consider questionable teeth in need of endodontic treatment, teeth requiring root amputations, hemi-sections or advanced periodontal procedures with a questionable prognosis and pulpless teeth fractured at the gingival margin with roots shorter than 13 mm. These teeth will require endodontic treatment, crown lengthening, post/cores and crowns; however, their longevity is very much in doubt with these parameters (60).
Practitioners are ethically obligated to inform patients of all reasonable treatment options. It is the patient’s attitude, values and expectations that are integral to the risk assessment algorithm. Poor motivation to retain a tooth mandates extraction, not clinical intervention whereas high motivation advocates non-surgical intervention or surgery. The process of planning, presentation and acceptance of dental treatment plans is always dominated by the duality of emotion and pragmatism associated with cost. Where it becomes specious is the side by side dollar comparison of restoring a natural tooth or placement of a fixed bridge et al in contrast to orthobiologic replacement of a debilitated tooth.
Far too often the comparison of purported treatment outcome percentages are based upon corporate affiliation and/or fiduciary bias, or are simply too narrow a parameter to suggest comparable alternatives. With the treatment options available to an experienced endodontist, only a very few structurally sound teeth need be removed.
Benjamin Disraeli said: “Expediency is a law of nature. The camel is a wonderful animal, but the desert made the camel.” The endodontic implant algorithm begs the question, “Does science drive the market, or does the market drive science”. “All truths are easy to understand once they are discovered; the point is to discover them.” — Galileo. Time and forbearance will bear witness to the discovery of the salient and relevant truths that guide the endodontic implant algorithm. oh
Dr. Serota has practiced dentistry in Mississauga, Ontario since 1973. His practice is focused on endododontic and implant solutions. A graduate of the University of Toronto and the Harvard School of Dental Medicine, he is the founder of the oldest online endodontic community, ROOTS.
Oral Health welcomes this original article.
Part II: Untying the Gordian Knot: Back to the Egg will address non-surgical and/or surgical resolution of failing primary treatment outcomes with apical periodontitis and orthobiologic replacement mimicry of the natural dentition using progressive thread design fixtures with precise cone connections.
1. Farzaneh M, Abitbol S, Lawrence H, Friedman S. Treatment Outcome in Endodontics-The Toronto Study. Phase II: Initial Treatment. J Endod 2004 May;30(5):302-309
2. Bero L, Rennie D. The Cochrane Collaboration. Preparing, maintaining, and disseminating systematic reviews of the effects of health care. JAMA 1995 Dec;274(24): 1935-1938
3. Salehrabi R, Rotstein I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod 2004 Dec;30(12):846-50
4. Cagidiaco MC, Garca-Godoy F, et al. Placement of fiber prefabricated or custom made posts affects the 3-year survival of endodontically treated premolars. Am J Dent 2008 Jun;21(3):179-84
5. Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration of endodontically treated teeth: a systematic review of the literature, Part II (Evaluation of fatigue behavior, interfaces, and in vivo studies). Quintessence Int 2008 Feb;39(2):117-29
6. Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of endodontically treated teeth. J Prosthet Dent 2002 Mar;87(3):256-63
7. Dorn SO, Moodnik RM, Feldman MJ, Borden BG. Treatment of the endodontic emergencies: A report on a questionnaire. Part I. J Endod 1977;3:94 -100
8. Gat
ewood RS, Himel VT, Dorn SO. Treatment of the endodontic emergency: A decade later. J Endod 1990;16:284 -91
9. Siqueira, J F. Endodontic infections: Concepts, paradigms, and perspectives. OS, OM, OP, OR & Endo Sept 2002;94(3):281-293
10. Siqueira JF Jr, Guimares-Pinto T, Ras IN. Effects of chemomechanical preparation with 2.5% sodium hypochlorite and intracanal medication with calcium hydroxide on cultivable bacteria in infected root canals. J Endod. 2007 Jul;33(7):800-5
11. Baumgartner JC, Hutter JW, Siqueira JF. Endodontic Microbiology and Treatment of Infections. In: Cohen S, Hargreaves KM, editors. Pathways of the Pulp. Ninth ed. St. Louis: Mosby; 2006
12. Baumgartner JC, Xia T. Antibiotic susceptibility of bacteria associated with endodontic abscesses. J Endod 2003;29(1):44-47
13. Khemaleelakul S, Baumgartner JC, Pruksakorn S. Identification of bacteria in acute endodontic infections and their antimicrobial susceptibility. Oral Surg Oral Med Oral Pathol 2002;94(6):746-55
14. Grondahl H-G, Huumonen S. Radiographic manifestation of periapical inflammatory lesions. Endodontic Topics 2004;8:55-67
15. Scarfe WC, Farman AG, Sukovic P. Clinical applications of cone-beam computed tomography in dental practice. JCDA 2006;72:75-80
16. Pinksy HM et al. Accuracy of three-dimensional measurements using cone-beam CT. Dentomaxillofacial Radiology 2006;35:410-6
17. Iwai et al. Estimation of effective dose from limited cone beam x-ray CT examination. Dental Radiology (Japanese) 2001;50:251-9
18. Patel S, Dawood A, Whaites E, Pitt Ford T. The potential applications of cone beam computed tomography in the management of endodontic problems. Int EndoJournal 2007;40:818-30
19. Estrela C. Accuracy of Cone Beam Computed Tomography and Panoramic and Periapical Radiography for Detection of Apical Periodontitis. J Endo 2008;34(3):273-279
20. Simon JHS, Enciso R, Malfaz JM, Rogers R, Bailey-Perry M, Patel A. Differential diagnosis of large periapical lesions using cone-beam computed tomography measurements and biopsy. J Endod 2006;32:833-7
21. Iqbal MK, Johansson AA, Akeel RF, Bergenholtz A, Omar R. A retrospective analysis of factors associated with the periapical status of restored, endodontically treated teeth. Int J Prosthodont 2003;16:31- 8
22. Siqueira JF Jr, Rocas IN, Favieri A, Abad EC, Castro AJ, Gahyva SM. Bacterial leakage in coronally unsealed root canals obturated with 3 different techniques. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;90:647-50
23. Schwartz RS, Fransman R. Adhesive Dentistry and Endodontics: Materials, Clinical Strategies and Procedures for Restoration of Access Cavities: A Review. J Endod March 2005;(31)3:151-165
24. Zehnder M, Kosicki D, et al. Tissue-dissolving capacity and antibacterial effect of buffered and unbuffered hypochlorite solutions. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology & Endodontics;(94):756-762
25. Sjogren U, Figdor D, Persson S, Sundqvist G. Influence of Infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endo Journal Sept 1997;(30)5:297-306
26. Siqueira JF, Ras IN, et al. Chemomechanical Reduction of the Bacterial Population in the Root Canal after Instrumentation and Irrigation with 1%, 2.5%, and 5.25% Sodium Hypochlorite. J EndodonJune 2000;(26)6:331-334
27. Torabinejad M, Cho Y, Khademi AA, Bakland LK, Shabahang S. The effect of various concentrations of sodium hypochlorite on the ability of MTAD to remove the smear layer. J Endod 2003;(29):233-239
28. Siqueira JF Jr, Rocas IN, Santos SR, Lima KC, Magalhaes FA, de Uzeda M. Efficacy of instrumentation techniques and irrigation regimens in reducing the bacterial population within root canals. J Endod 2002;28:181-184
29. Niu W, Yoshioka T, Kobayashi C, Suda H. A scanning electron microscopic study of dentinal erosion by final irrigation with EDTA and NaOCl solutions. Int Endod J 2002;35:934-939
30. Lin LM, Rosenberg PA, Lin J. Do procedural errors cause endodontic treatment failure? JADA 2005;(136) 2:187-193
31. De-Deus G et al. Dye extraction results on bacterial leakproof root fillings. J Endo Sept 2008;(34)9:1093-5
32. Barthel CR, Moshonov J, Shuping G, Orstavik D. Bacterial leakage versus dye leakage in obturated root canals. Int Endod J 1999;32:370 -5
33. Kersten HW, Moorer WR. Particles and molecules in endodontic leakage. Int Endod J 1989;22:118-24
34. Oliver CM, Abbott PV. Correlation between clinical success and apical dye penetration. Int Endod J 2001;34:637-44
35. Paqu F, Sirtes G. Apical sealing ability of Resilon/Epiphany versus gutta-percha/AHPlus: immediate and 16-months leakage. Int Endod J. 2007 Sep;40(9):722-9
36. Cruse WP, Bellizzi R. A historic review of endodontics 1689-1963, Part I. J Endod,1980; 6:495-499
37. Blaney JR. The biologic aspect of root canal therapy. Dental Items of Interest 1927;49:681-708
38. Schilder H. Filling root canals in three dimensions. Dental Clinics of North America 1967;723-44
39. Ingle H: Endodontics, ed 5, Hamilton, London, 2002 BC Decker
40. Wu MK, Fan B, Wesselink PF. Leakage along apical root fillings in curved root canals. I. Effects of apical transportation on seal of root fillings J Endodon 2000;(26):210
41. Siqueira JF Jr. Aetiology of the endodontic failure: why well-treated teeth can fail. Int Endod J 2001;34:1-10
42. Roggendorf et al. Bacterial leakage in filled root canals using four root canal sealers. IEJ Dec 2007;40(2): Abstract R3.86
43. Roedl et al. Bond strength to root canal dentine following different irrigation protocols using a new testing method. IEJ Dec 2007;(40)12:Abstract R3.66
44. Raina R et al. Evaluation of the Quality of the Apical Seal in Resilon/Epiphany and Gutta-Percha/AH Plus-filled Root Canals by Using a Fluid Filtration Approach J Endod;(33)8:944-47
45. Teixeira FB, et al. Fracture resistance of roots endodontically treated with a new resin filling material. JADA 2004;(135)5:646-652
46. Sly MM, Moore BK, Platt JA, Brown CE. Push-out bond strength of a new endodontic obturation system (Resilon/Epiphany). J Endod. 2007 Feb;33(2):160-2
47. Williams C, Loushine R et al. A Comparison of Cohesive Strength and Stiffness of Resilon and Gutta-Percha. J Endod 2006;(32)6:553-5
48. Tay F, Loushine R et al. Ultrastructural Evaluation of the Apical Seal in Roots Filled with a Polycaprolactone-Based Root Canal Filling Material. J Endod 2005;(31)7:514-19
49. Kapalas A, Lambrianidis T. Factors associated with root canal ledging during instrumentation. Endod Dent Traumatol 2000;16:220-231
50. Souza, RA. Clinical and radiographic evaluation of the relation between the apical limit of root canal filling and success in Endodontics. Part 1 Braz Endod J 1998;3:43-48
51. AL-Omari MAO, Dummer PM. Canal blockage and debris extrusion with eight preparation techniques. J Endod 1995;21:154-158
52. McKendry DJ. Comparison of balanced forces, endosonic, and step-back filing instrumentation techniques: quantification of extruded apical debris. J Endod Jan 1990;16(1):24-7
53. Mullaney TP. Instrumentation of finely curved canals. Dent Clin North Am 1979;23:575-92
54. Morgan LF, Montgomery S. An evaluation of the crown-down pressureless technique. J Endod 1984;10:491-8
55. M. Al-Omari, P. Dummer. Canal blockage and debris extrusion with eight preparation techniques. J Endod 2006;21(3):154-158
56. P. Hankins, M. ElDeeb/ An evaluation of the canal master, balanced-force, and step-back techniques. J Endod 1996;22(3):123-130
57. Siqueira J, Arajo M, Garcia P, Fraga R, Dantas C. Histological evaluation of the effectiveness of five instrumentation techniques for cleaning the apical third of root canals. J Endod 1997;23(8): 499-502
58. Serota KS et al. Predictable endodontic success: The apical control zone. Dentistry Today May 2003;(22)5:90-7
59. Peters OA, Pete
rs C, et al. ProTaper rotary root canal preparation: effects of canal anatomy on final shape analysed by micro CT. Int Endo J February 2003;(36)2:86-92
60. Becker W. Immediate implant placement: Diagnosis, treatment planning and treatment steps for successful outcomes. J Calif Dent Assoc 2002;33:303-310
@ARTICLECATEGORY:594;