


Full coverage crowns and ceramic veneers are used to treat patients with structural damage to anterior teeth caused by caries, previous restorations or trauma. Additionally, ceramic veneers can be used as an esthetic treatment to correct the shape and color of anterior teeth. Currently, ceramic materials have become the material of choice for anterior crowns, largely replacing metal-based options. According to a 2016 survey, 54% of dentists preferred lithium disilicate as the restorative material for a single anterior crown, while 17% chose porcelain-fused-to-zirconia and 14% selected leucite.1 As ceramic materials are more translucent than the metal copings in porcelain-fused-to-metal crowns, the clinician must be cognizant of the underlying color of their tooth preparations when restoring anterior teeth with ceramic restorations. The tooth preparation may not be ideal in color from tooth discoloration (i.e. tetracycline staining, materials or tissue in endodontic access, etc.) or when a patient’s natural tooth shade is lower in value than their desired shade.
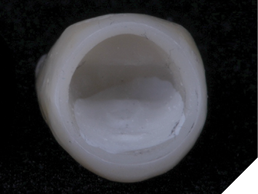
When preparing anterior teeth for crowns, several strategies can help manage the color of the underlying tooth preparation. First, selecting the appropriate restorative material can help mask undesirable tooth color. For example, porcelain-fused-to-zirconia crowns have a zirconia coping that is more effective at masking discolored preparations than lithium disilicate.2 For example, 0.5 mm of low-translucency zirconia offers similar opacity to 1.2 mm of lithium disilicate.3 Second, resin opaquers can be applied to the tooth preparation to alter its color. Opaquers are similar to flowable composites (Fig. 1), but they are significantly more opaque (Fig. 2). They are available in white, dentin and pink shades. Third, some laboratories have an opaque paint that they can apply in the inside of a ceramic restoration to increase its masking ability (Fig. 3). Opaque esthetic colorants can also be painted on the internal of pre-sintered zirconia which increases the internal opacity of the zirconia restoration once sintered. A fourth method to modify the color of a ceramic restoration is through internal or external bleaching of the abutment tooth, though internal bleaching is only appropriate for teeth that have undergone endodontic treatment. If external bleaching is performed before bonding restorations, patients should refrain from bleaching for at least two weeks prior to bonding.4 This precaution ensures that oxygen release from the bleaching agents does not inhibit the polymerization of adhesive resins. Finally, an opaque cement may be used to mask the color of the underlying tooth.2 Typically, the cement space for restorations is 100 microns (0.1 mm) or less. The use of an opaque cement in this thin space can be a method to allow slight modification of the shade of a ceramic restoration at the delivery appointment. The use of a cement is often a final opportunity to modify the shade of a restoration once it has already been fabricated.
Fig. 1
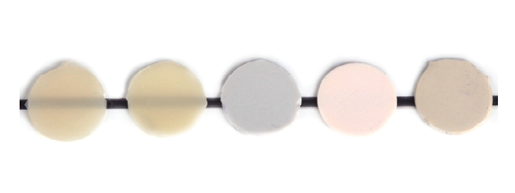
Fig. 2

Fig. 3
For veneer preparations, some of the options mentioned above for masking discolored preparations are less applicable. While zirconia can be used for anterior veneers following a zirconia bonding protocol,5 many clinicians may lack the necessary armamentarium or experience for zirconia bonding. Therefore, using a zirconia veneer to block a discolored tooth preparation is not common. Most clinicians choose to restore veneers with glass ceramics, such as lithium disilicate, leucite or feldspathic porcelain. Lithium disilicate is available in different translucencies (i.e. low translucency, medium translucency, high translucency). A low translucency lithium disilicate can be selected for a discolored tooth preparation as this may help to mask a discolored preparation; however, the thickness of the ceramic restoration has a greater influence on its masking ability than its translucency.6 Resin opaquers are generally unsuitable for veneer preparations, as they can obscure the enamel surface, creating an additional bonding interface that may compromise bond strength. Therefore, veneer preparations typically rely on either pre-preparation bleaching, the use of an opaque cement shade or ensuring sufficient thickness of the restorative material to mask any discoloration.
The thickness of a veneer is determined by its fit within the space created by the tooth’s facial contours and the amount of tooth reduction provided. Understanding the adequate thickness of restorative materials to mask underlying tooth preparations is critical for planning the facial contours of anterior restorations and ensuring proper tooth reduction. Keeping a veneer preparation in enamel is important both for achieving enamel bonding as well as maintaining a high modulus (stiff) enamel substrate to match the high modulus of ceramic. On average, the enamel thickness of a maxillary central incisor is 1 mm in the middle and incisal thirds and 0.4 mm in the cervical third.7 Therefore, the clinician is limited in the amount of facial reduction that can be achieved for a veneer preparation. Additional restorative material thickness can be gained by bulking the facial contours of planned restorations. Excessive facial bulk of an anterior restoration impairs the esthetic outcome, gingival emergence profile, and phonetic function.
Knowledge of the translucency of materials like lithium disilicate helps predict the thickness required to achieve the desired shade. For example, 0.4 mm of a low translucency lithium disilicate and 0.6 mm of high translucency lithium disilicate were able to mask a discolored dentin specimen.8 However, these guidelines are approximations, and it is beneficial for the clinician, technician, and patient to verify the final color before fabricating the permanent restoration.
This article proposes a technique for verifying the final color of a prepared tooth using a bis-acryl try-in. For this method to be effective, the bis-acryl material must exhibit a similar translucency to the ceramic restoration being used. Lithium disilicate, a common glass ceramic material for veneers, is composed of lithium disilicate crystals embedded in a glass matrix, whereas bis-acryl provisional materials typically contain ceramic or glass fillers embedded in a resin matrix. To assess the suitability of bis-acryl try-ins for color prediction, a laboratory spectrophotometer was used to compare the translucency of various bis-acryl materials at different thicknesses with that of lithium disilicate.
Laboratory study
Low and medium translucency lithium disilicate blocks (IPS e.max CAD LT and MT, shade A2) were sectioned into 0.5, 0.7, 1.0, 1.3, and 1.5 mm thick tiles. The tiles were crystallized in a furnace according to the manufacturer’s instructions. An impression of a tile at each thickness was taken with a clear poly vinyl siloxane impression material in order to fabricate molds. Three different A2 shade bis-acryl provisional materials (Inspire, Clinicians Choice; Integrity, Dentsply Sirona; Luxatemp, DMG) were injected into the molds. The molds were covered with a glass slide and light cured for their manufacturers recommended curing time. All tiles were polished on both sides to 1200 grit SiC paper and final thicknesses were confirmed to be within 0.04 mm of intended thickness with digital calipers.
The translucency of each tile was measured with a laboratory spectrophotometer (CM-700d, Konica Minolta). A spectrophotometer is a device which measures the color of an object by shining light on a specimen, measuring the wavelengths of light reflected back to a sensor, and converting those wavelengths to a 3-axis color coordinate system (L=lightness/darkness, a=red/green, b=yellow/blue). Color differences can be calculated using a mathematical formula which measures the distance between two colors in the color coordinate system. A commonly used color difference formula is known as ∆E2000. Spectrophotometers can measure translucency by measuring the color difference of a tile when it is placed against a light and dark background. The color difference of an object on a light and dark background is known as its Translucency Parameter (TP). If the color difference is large (TP is high), the tile is translucent.
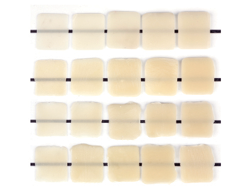
The previously prepared lithium disilicate and bis-acryl tiles were placed against white and then black calibrated backgrounds and their color was measured with the spectrophotometer. The color difference was used to calculate TP. The TPs of the bis-acryl materials relative to the medium translucency lithium disilicate is presented in Figure 4 and the low translucency lithium disilicate is presented in Figure 5. The tiles were photographed against a black line (Fig. 6).
Fig. 4
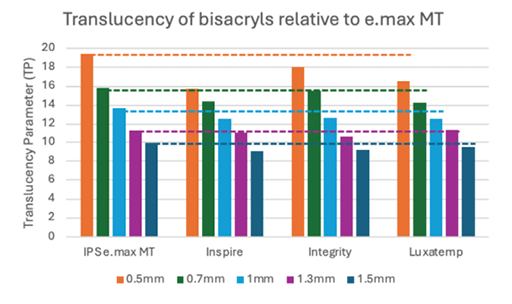
Fig. 5
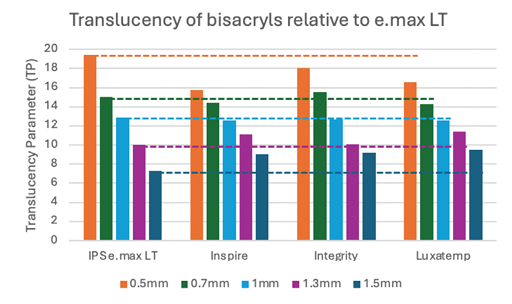
Fig. 6
The results of this study indicate that most of the bis-acryl materials were slightly more opaque than medium translucency lithium disilicate at all thicknesses and the low translucency lithium disilicate at 0.5 mm thickness. The bis-acryls best represented low translucency lithium disilicate at 0.7 to 1.3 mm thickness. Clinically, these results suggest that the bis-acryl try-in would work best at thicknesses of 0.7 mm and thicker. At 0.5 mm thickness, bis-acryl may overexaggerate the amount of masking that will be performed by lithium disilicate.
Case example
A patient presented for an esthetic treatment of her anterior teeth due to her concern with the color and shape of her teeth. Ceramic veneers were treatment planned for teeth #6-11 and ceramic crowns for teeth #4, 5, 12, and 13 to replace existing restorations and improve color and shape of teeth. The patient’s original shade was C3, and she desired a brighter but natural smile. Shade A1 was selected. After preparation of her teeth, the discoloration of her dentin created a dark tooth preparation (Fig. 7). Preparations of the teeth had been performed through a bis-acryl mock-up of the final contours of the teeth. Reduction was determined to be between 0.3 to 0.5 mm as determined by a depth reduction bur. A bis-acryl try-in was inserted to determine if the bis-acryl could sufficiently mask the discoloration of her teeth, understanding that the try-ins may overexaggerate the amount of masking that will be performed by lithium disilicate. Figure 8 demonstrates an acceptable shade of the restorations. Therefore, the final restorations were fabricated out of a low translucency lithium disilicate material. Incisal characterization was achieved with a cut back and layering of porcelain. A tooth-shade resin cement was used to bond the veneers as no additional modification in translucency was required. The final restorations achieved the desired shade of the restorations (Fig. 9). Another case of using a bis-acryl try in to mask discolored tooth preparations is presented in Figures 10-12.
Fig. 7

Fig. 8

Fig. 9

Fig. 10

Fig. 11

Fig. 12

Conclusions
Several methods exist to mask a discolored crown preparation including the use of a porcelain fused to zirconia restoration, resin opaquers on the tooth preparation, opaque paints on the internal surface of the crown, bleaching of the tooth preparation, and an opaque cement. For veneer preparations, options to block a discolored preparation include bleaching of the tooth preparation, the use of an opaque cement, or providing sufficient thickness of the restorative material. This study presents a technique for using a bis-acryl try-in to predict the masking ability of lithium disilicate at different translucencies and thicknesses. This technique works reasonably well at restorations thicknesses between 0.5 -1.5 mm. 
Oral Health welcomes this original article.
References
- Makhija SK, Lawson NC, Gilbert GH, Litaker MS, McClelland JA, Louis DR, Gordan VV, Pihlstrom DJ, Meyerowitz C, Mungia R, McCracken MS; National Dental PBRN Collaborative Group. Dentist material selection for single-unit crowns: Findings from the National Dental Practice-Based Research Network. J Dent. 2016 Dec;55:40-47. doi: 10.1016/j.jdent.2016.09.010. Epub 2016 Sep 28. PMID: 27693778; PMCID: PMC5125852.
- Bacchi A, Boccardi S, Alessandretti R, Pereira GKR. Substrate masking ability of bilayer and monolithic ceramics used for complete crowns and the effect of association with an opaque resin-based luting agent. J Prosthodont Res. 2019 Jul;63(3):321-326. doi: 10.1016/j.jpor.2019.01.005. Epub 2019 Feb 10. PMID: 30755361.
- Nizami B, Bloom H, Lawson NC, Le R, Goldstein RE. Prevention and Management of Discolored Tooth Preparations. Oral Health. 2023
- de Almeida AA, Lima DM, Pereira AF, Sousa SF, Alves CM. Influence of delay between dental bleaching with 35% hydrogen peroxide and orthodontic brackets on the bond strength at the enamel/adhesive interface. J Clin Exp Dent. 2019 May 1;11(5):e447-e451. doi: 10.4317/jced.55719. PMID: 31275517; PMCID: PMC6599696.
- Sulaiman TA, Suliman AA, Abdulmajeed AA, Zhang Y. Zirconia restoration types, properties, tooth preparation design, and bonding. A narrative review. J Esthet Restor Dent. 2024 Jan;36(1):78-84. doi: 10.1111/jerd.13151. Epub 2023 Oct 15. PMID: 37840220; PMCID: PMC10842315.
- Ayata M, Kilic K, Al-Haj Husain N, Özcan M. Effect of Thickness and Translucency on Color Change and Masking Ability of Ceramic Materials used for Laminate Veneers. Eur J Prosthodont Restor Dent. 2023 Nov 30;31(4):383-390. doi: 10.1922/EJPRD_2501Ayata08. PMID: 37194571.
- Ferrari M, Patroni S, Balleri P. Measurement of enamel thickness in relation to reduction for etched laminate veneers. Int J Periodontics Restorative Dent. 1992;12(5):407-13. PMID: 1343012.
- Pala K, Reinshagen EM, Attin T, Hüsler J, Jung RE, Ioannidis A. Masking capacity of minimally invasive lithium disilicate restorations on discolored teeth-The impact of ceramic thickness, the material’s translucency, and the cement color. J Esthet Restor Dent. 2024 Jan;36(1):107-115. doi: 10.1111/jerd.13146. Epub 2023 Nov 7. PMID: 37933738.
About the authors

Silvia Rojas Rueda, DDS, is a pediatric dentist and dental biomaterials researcher currently pursuing a master’s degree at the University of Alabama at Birmingham. With extensive experience in both clinical practice and research, her work focuses on biomaterials, restorative dentistry, and digital workflows.

Mohammed Hammamy is a first year resident in the UAB Biomaterials residency program.

Dr. Adamo Notarantonio is a graduate of the State University of New York at Stony Brook School of Dental Medicine (2002), where he received honors in both removable and fixed prosthodontics. His memberships to professional organizations include the American Academy of Restorative Dentistry, the American Academy of Cosmetic Dentistry, the American Equilibration Society, the International Congress of Oral Implantologists, the Academy of General Dentistry, and the American Dental Association.

Dr. Amanda Seay operates a full-time private practice specializing in comprehensive restorative dentistry in Charleston, South Carolina. Dr. Seay is an esteemed member of various professional organizations, including the American Academy of Restorative Dentistry, American Academy of Esthetic Dentistry, American Society of Dental Aesthetics, and she holds the distinguished title of Fellow Accredited Member in the American Academy of Cosmetic Dentistry.

Nate Lawson, DMD, PhD is an associate professor and the director of the Division of Biomaterials at the UAB School of Dentistry.