
Patients seek out cosmetic dentists with an expectation of improving their smile. Sometimes patients have well thought out and easily articulated expectations related to their treatment goals. More often, they have a vague, idealized vision of “perfection” that they cannot define. Communication becomes a major factor in the success or failure of a case. It is critical for the dentist to understand the patient’s wishes and set reasonable expectations for the results of any proposed treatment. At this point, it becomes important to discuss treatment options, the benefits and risks of treatment, the financial investment required, long term maintenance of treatment, and proposed longevity of the result. This communication between the patient and the dentist is an important part of the practice of Responsible Esthetics. This time spent with the patient discussing options and defining treatment results is a mutual investment in success.
Responsible Esthetics is defined as “The practice of patient-engaged interdisciplinary dentistry focused on achieving lifelong optimal cosmetic and functional results while minimizing risk to healthy tissues.” While the goal of Responsible Esthetics is to provide a lifelong result, dentists must also take into consideration that restorative materials can wear out, and the replacement of failed restorations can be part of a lifelong plan. It is important for dentists to consider that just as life’s journey is full of growth and change, a patient’s dental needs and desires may also change with the passage of time.
Case study
Diagnosis
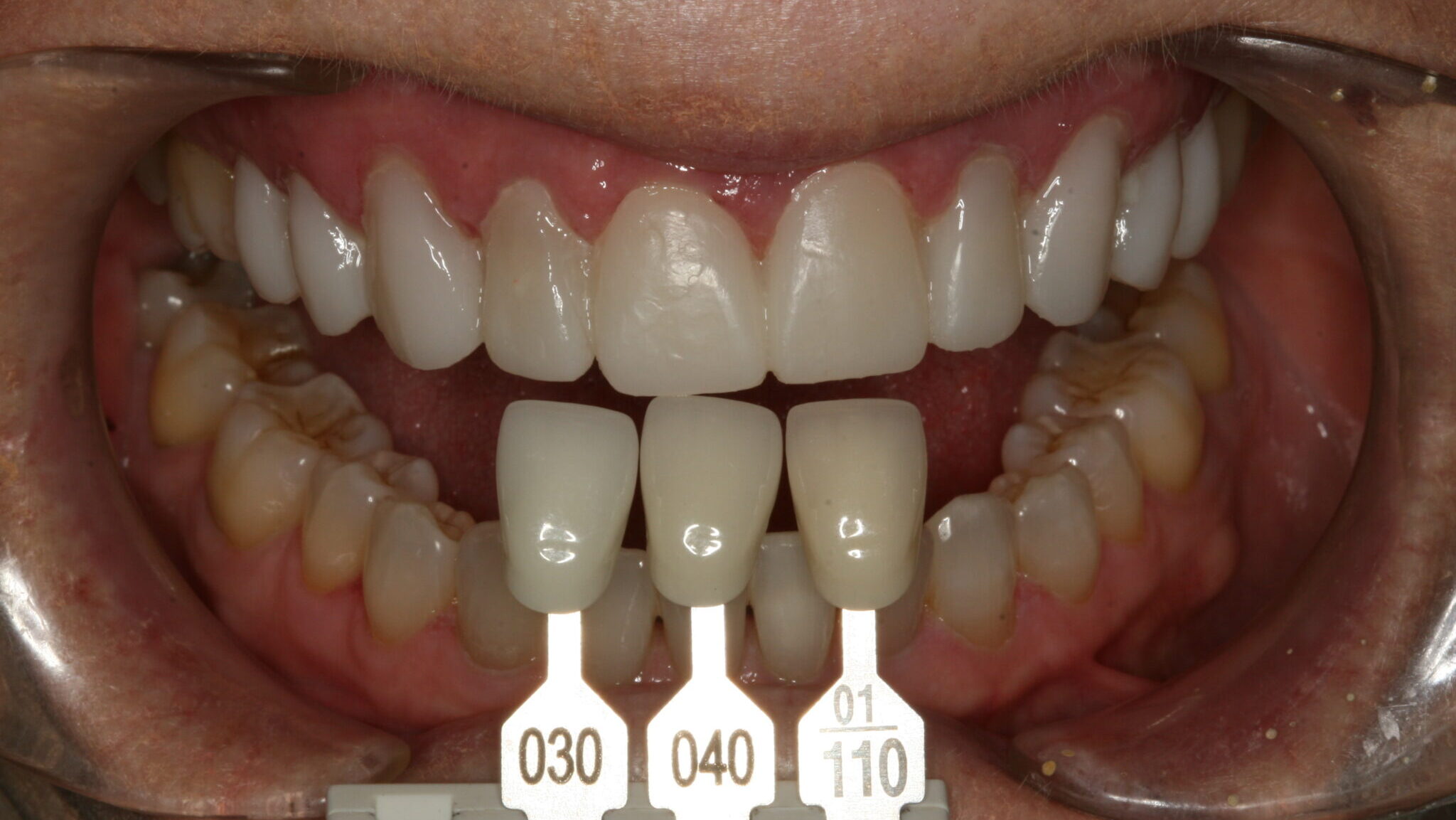
A 65-year-old female in good medical and dental health presented for restorative consultation stating she maintains annual dental cleanings. She stated that she wanted to improve her smile. The patient stated that she was not happy with the color or shape of her upper teeth. A series of diagnostic photographs were made (Fig. 1). Radiographic examination was performed including a full mouth series of periapical radiographs and a panoramic radiograph. Clinical examination revealed a Class I dental relationship with no significant occlusal interferences.1 Several posterior restorations were observed along with the presence of composite bonding to close a diastema between her maxillary central incisors. A periodontal evaluation revealed generalized health with several areas of gingival asymmetry.2 Evidence of generalized wear was found throughout the patient’s dentition; however, the patient exhibited no symptoms of any temporomandibular disorder and appeared asymptomatic during a TMJ evaluation. Alginate impressions were made of her upper and lower dentition along with a polyvinyl siloxane centric bite registration.
Fig. 1

Treatment plan
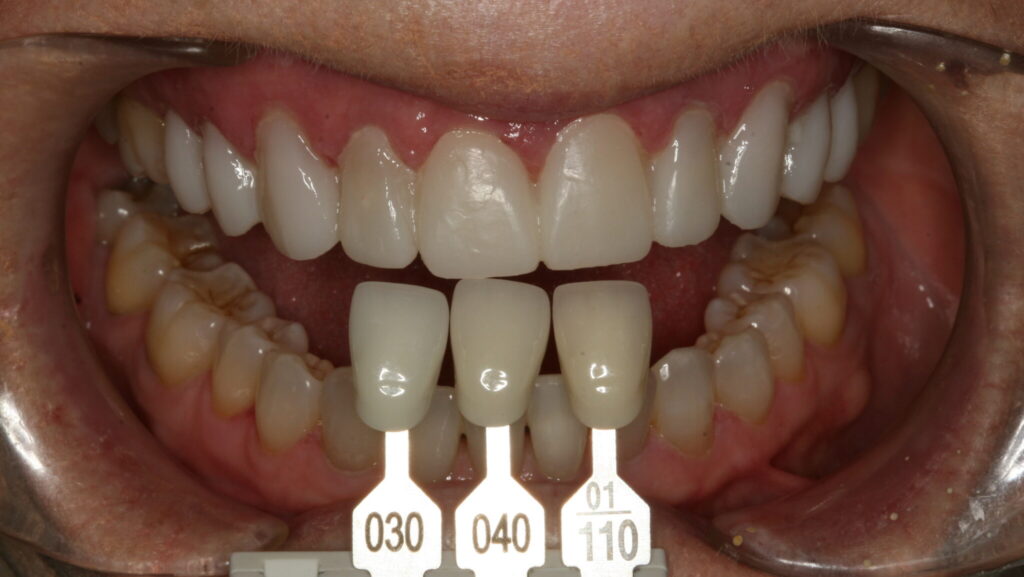
The patient was asked to return for a planning appointment.2 During that appointment, she expressed a desire to change the color and shape of her upper teeth (Fig. 2). She also stated that she felt any proposed treatment should be both conservative and cost effective. Several different methods for addressing her desires were discussed including whitening, orthodontics, composite bonding, and porcelain veneers. The benefits and risks of each treatment were discussed thoroughly. After she had the opportunity to ask questions about each procedure discussed, the patient again emphasized that a conservative result was her primary goal and elected to pursue composite bonding on her upper 10 teeth. Proper care for the future restorations was discussed including nightly wear of a hard protective occlusal guard, and the importance of optimal maintenance including regular cleanings and examinations was stressed.1
Fig. 2

Description of treatment
The patient was able to view and approve a diagnostic wax-up of proposed treatment results prior to commencement of treatment. As the treatment planned was primarily additive, with the exception of, gingival recontouring on teeth #6, 10, and 11, only topical anesthetic was used. Tissue sculpting was performed with a Gemini Diode laser (Ultradent Corp; West Jordan, UT) to even gingival levels on teeth #6, 10, and 11.
Light tooth preparation was completed with a 703.8F diamond bur (Premier Dental; Plymouth Meeting, PA) in a high-speed handpiece under copious water spray. Due to the diastemata and positioning of the patient’s teeth, minimal tooth reduction of the patient’s enamel was required. Each tooth was acid etched for 15 seconds with 35% UltraEtch phosphoric acid gel etchant (Ultradent Corp; West Jordan, UT) followed by rinsing with a copious air and water spray.3,4 All teeth were lightly dried, but not dessicated.3,4 Two coats of All Bond Universal bonding agent (Bisco; Schaumberg, IL) were applied to each tooth and agitated for 20 seconds prior to air thinning to evaporate solvents. Each tooth was cured for 20 seconds with a Bluephase LED curing light (Ivoclar Vivadent; Amherst, NY). Incisal edges were built up with hybrid milky-white occlusal composite (Cosmedent Inc.; Chicago, IL). Body shades of BZero and B1 microfilled composite (Cosmedent Inc.; Chicago, IL) were used to build up the teeth and develop primary anatomy. Each increment was cured for 20 seconds following placement and shaping. Characterization was added with Honey Yellow, Gray, and White tints (Cosmedent Inc.; Chicago, IL) (Fig. 3). Each tooth was cured an additional 20 seconds prior to adding a final layer of microfilled Incisal Light composite (Cosmedent Inc.; Chicago, IL) (Fig. 4). A final 20 second cure was performed on each tooth.
Fig. 3

Fig. 4

Gross contouring was performed using a coarse abrasive Mini FlexiDisc (Cosmedent Inc; Chicago, IL). Interproximal areas were contoured with Epitex finishing strips (GC America Inc; Alsip; IL). Labial texture was accentuated with a coarse flame diamond (Brasseler USA Dental; Savannah, GA) using a light touch while moving back and forth in a mesial to distal direction. Final polish was performed with a Medium Grit FlexiCup (Cosmedent Inc; Chicago, IL) and DiaComp Feather Lite polishers (Brasseler USA Dental; Savannah, GA) (Fig. 5). The patient’s teeth were inspected for any excess restorative material. Post-operative home care instructions were given and the patient was scheduled for a follow-up appointment in two weeks for a final check for function and esthetic evaluation (Figs. 6 & 7).
Fig. 5

Fig. 6

Fig. 7

Continued care
The patient maintained regular 6-month recare appointments for 14 years. She was extremely pleased with her bonding results. She was diligent with her home care and wore her bite guard nightly. During that period of time, she experienced a few minimal chips of her composite bonding which were easily repaired. At approximately 13 years following placement of her composite bonding, the patient started to become aware of some marginal staining and breakdown of her composite bonding (Fig. 8). This initiated a second treatment planning discussion with the dentist to explore future plans.
Fig. 8

Treatment plan #2
The patient, now 79 years old, recalled her planning appointment approximately 14 years earlier. She and the dentist discussed her previous restorative experience, and her desires for her smile going forward. The patient was pleased with the general shape of her teeth with the exception of some worn areas. Her chief complaints were generalized staining and breakdown at the margins of her composite bonding and tissue changes at the gingival margins of #8 and 9 (Fig. 9). This time, however, the patient’s desires had changed. While she had been happy with her bonding, she now desired a longer lasting, more durable restorative option. Furthermore, she stated she was not opposed to tooth preparation and was comfortable to make a more significant financial investment in her smile if the result could be as beautiful as her bonding and more durable. Given this information, the patient and the dentist discussed the benefits and risks of retreating her upper 10 teeth with new composite bonding or porcelain veneers. The patient elected to pursue porcelain veneers on her upper 10 teeth.
Fig. 9

Description of treatment #2
Under color corrected lighting, digital photographs were made from multiple document the patient’s current condition and communicate her desires to the ceramist (Fig. 10). Profound anesthesia of #4-13 was obtained through the use of topical benzocaine and lidocaine HCl 2% and 1:100,000 epinepherine injection (Septodont; Lancaster, PA). The patient’s lips were adequately and comfortably retracted for the entire procedure using an Optragate lip retractor (Ivoclar Vivadent; Amherst, NY).
Fig. 10

Initial tooth preparation was completed with a 2000.10 Two Striper super-coarse grit diamond bur (Premier Dental; Plymouth Meeting, PA) in a high-speed handpiece under copious water spray (Fig. 4). Due to the previous additive bonding, minimal tooth reduction of the patient’s enamel was required. A well-defined cervical margin was established with a 703.8F diamond bur (Premier Dental; Plymouth Meeting, PA) to provide a positive veneer stop with a smooth, cleansable, precise porcelain to tooth interface while allowing for development of proper emergence profile.3,4 Photographs of the preparations were made and a preparation shade of st9 (Ivoclar Vivadent; Amherst, NY) was recorded. Expa-syl gingival retraction paste (Acteon Group; Mèrignac, France) was expressed around all gingival margins to provide hemostasis and adequate tissue reflection. After 3 minutes the paste was rinsed away with a copious, forceful water spray. The preparations were dried and a master polyvinyl impression was made with Honigum Pro Light and Heavy impression material (DMG America; Englewood, NJ) (Fig. 5). A Futar D (Kettenbach; Eschenburg, Germany) stick bite of the prepared teeth in centric occlusion was made and photographed.
The patient’s teeth were cleaned with Consepsis chlorhexidine (Ultradent Corp; West Jordan UT). Bisacrylic provisionals were fabricated from BL Luxatemp Ultra (DMG America; Englewood, NJ). The provisionals were trimmed and then seated with TempoCem ID (DMG America; Englewood, NJ). Excess material was removed with a #12 scalpel blade, a 15 second curing time per tooth was completed, and the provisionals were smoothed and finished with abrasive discs (Cosmedent Inc.; Chicago, IL) and a rubber cup polisher (Cosmedent Inc.; Chicago, IL). Occlusion was verified and checked, and the patient was appointed for a post-operative check twenty-four hours later (Fig. 11).
Fig. 11
Cementation
On return from the ceramist, the porcelain restorations were inspected on the dies for marginal fit and on solid models for proper interproximal contacts. Profound anesthesia of #4-13 was obtained through the use of topical benzocaine and lidocaine HCl 2% and 1:100,000 epinepherine injection (Septodont; Lancaster, PA). An Optragate lip retractor (Ivoclar Vivadent; Amherst, NY) was placed to assist in isolation. The provisional veneers were removed, and the preparations were cleaned to remove any residual resin temporary material or debris. The veneers were then tried into the patient’s mouth and evaluated for fit and esthetics.
Upon removal from the patient’s mouth, the veneers were treated with Ivoclean cleaning paste (Ivoclar Vivadent; Amherst, NY) to remove any possible contamination. They were rinsed, dried, and Monobond silane coupling agent (Ivoclar Vivadent; Amherst, NY) was applied to the intaglio of the veneers.5 They were air dried, and a thin coating of All Bond Universal bonding agent (Bisco; Schaumberg, IL) was applied to the inside of the veneers. Vitique Clear Veneer Cement (DMG America; Englewood, NJ) was then applied to the veneers and they were immediately placed into a ResinKeeper light-safe box (Cosmedent Inc.; Chicago, IL) to prevent polymerization of the resin.3,4
The preparations were acid etched for 15 seconds with 35% UltraEtch phosphoric acid gel etchant (Ultradent Corp; West Jordan, UT) followed by rinsing with a copious air and water spray.3,4 All preparations were lightly dried, but not dessicated.3,4 Two coats of All Bond Universal bonding agent (Bisco; Schaumberg, IL) were applied to each preparation and agitated for 20 seconds prior to air thinning to evaporate solvents. The veneers were then removed from the light-safe box and seated on their respective preparations. They were tacked into place for 5 seconds each with the curing light.6 Excess was removed gently with a scaler, floss was passed through the contacts, and the veneers were then cured fully for an additional 30 seconds each.6 DeOx oxygen inhibiting gel (Ultradent Corp; West Jordan, UT) was expressed around all margins and the restorations were cured an additional 10 seconds to finalize polymerization.3,4,5 The patient’s occlusion was checked and smooth, proper contacts were verified with dental floss. Post-operative home care instructions were given, and the patient was scheduled for a follow-up appointment (Figs. 12-13).
Fig. 12

Fig. 13

Conclusion
Both composite bonding and porcelain veneers can be employed to provide beautiful, natural, and long-lasting functional cosmetic results. The needs and desires of patients can change over time and will play a large role in dictating appropriate treatment decisions. Successful treatment is defined through careful planning, great communication, and meticulous use of contemporary dental techniques and materials (Fig. 13). 
Oral Health welcomes this original article.
Acknowledgements: The author would like to express sincere appreciation to Wayne B. Payne, MDT, AAACD and Tyler Payne for their technical expertise and beautiful porcelain work.
References
- Dawson, Peter E. Evaluation, Diagnosis, and Treatment of Occlusal Problems. The C.V. Mosby Co.: St Louis, MO; 1989.
- American Academy of Cosmetic Dentistry. Diagnosis and Treatment Evaluation in Cosmetic Dentistry: A Guide to Accreditation Criteria. Madison (WI): The Academy; 2001.
- Magne, Pascal. Bonded Porcelain Restorations in the Anterior Dentition A Biomimetic Approach. Quintessence Books: Chicago, IL; 2002.
- Gurel, Galip. The Science and Art of Porcelain Laminate Veneers. Quintessence Books: Chicago, IL; 2003.
- Touati B, Quintas AF. Aesthetic and Adhesive Cementation for Contemporary Porcelain Crowns. Practical Procedures in Aesthetic Dentistry. 13(8): 611-620, 2001.
- Miller, Michael B. Reality: The Techniques: Volume I. Reality Publishing Co.: Houston, TX; 2003.
About the author

Dr. Rowe maintains a private practice dedicated to excellence in general, cosmetic, and complex restorative dentistry located in Jonesboro, Arkansas. He is an Accredited Member of the American Academy of Cosmetic Dentistry, past member and Chairman of the American Board of Cosmetic Dentistry, and has served as the AACD’s Chairman of Accreditation. He also serves as an Accreditation Examiner for the American Academy of Cosmetic Dentistry. He is a graduate of the University of Tennessee College of Dentistry, and is a formally trained artist having graduated from Washington and Lee University with a Bachelor of Arts degree in Studio Art. Dr. Rowe enjoys sharing his passion for cosmetic dentistry materials and techniques, lecturing nationally and internationally.