
Abstract
The management of patients with a collapsed bite presents both diagnostic and therapeutic challenges, particularly when vertical dimension of occlusion (VDO) must be reestablished. This paper outlines a phased, rationalized protocol based on the Turner–Missirilian classification, emphasizing ethical considerations, functional evaluation, and patient-centred care. Phase I utilizes a Mandibular Orthopedic Repositioning Appliance (Gelb appliance) to establish a comfortable and functional VDO, often yielding symptomatic relief in cases of arthrogenic temporomandibular joint disorder (TMD). Phase II involves stabilization using orthodontic, fixed, or removable prosthetic modalities. A key innovation described is the use of a custom-fabricated palatal jig, which facilitates accurate occlusal registration and eliminates the need for prolonged provisional restorations. A case report demonstrates successful application of this protocol, resulting in functional rehabilitation and resolution of TMD symptoms. This technique provides a predictable, efficient, and patient-friendly approach for restoring occlusion in complex cases involving loss of VDO.
The term collapsed bite encompasses various occlusal relationships, wherein similar occlusal schemes can have different functional consequences depending on the patient. In many cases where function remains unaffected and no symptoms of dysfunction are reported, observation with periodic follow-up is often sufficient, and treatment may not be necessary. However, it is a matter of professional ethics to inform the patient of the clinical findings and the potential for future complications.
When symptoms of dysfunction are present—such as muscle pain, temporomandibular joint disorder (TMD), or occlusal trauma with its implications for pulpal and periodontal health—treatment must be considered.
For assessment and diagnosis in such cases, we use the Turner–Missirilian classification system,1 which categorizes patients into three groups in which restorative treatment may be indicated:
Category I: Restorative treatment to increase and reestablish the lost vertical dimension of occlusion (VDO), often including prosthetic replacement of missing teeth.
Categories II and III: Restoration of severely worn or missing teeth, with increase of VDO considered only as a last resort.
Changes in VDO inevitably influence the condylar position within the fossa. Since this new position depends on the occlusion, new occlusal contacts must be established. It is advised that changes to the occlusion and condylar position (i.e., the new VDO) be implemented through a trial period using removable overdentures, followed by fixed provisional restorations. These trial periods, lasting several months, allow for functional evaluations and adjustments. Once the patient reports consistent comfort, definitive fixed restorations are fabricated based on the occlusal pattern established by the provisional restorations.
Other studies also recommend a similar approach for patients with collapsed bite, especially in cases requiring an increase in VDO.2-4
Clinical experience and challenges
In our clinical experience, adhering to this staged protocol has led to favorable outcomes. However, many patients find prolonged treatment periods challenging, especially when using removable transitional overdentures. These often interfere with speech and mastication, and are commonly the most objectionable part of the treatment.
In recent years, we have replaced removable overdentures with a Mandibular Orthopedic Repositioning Appliance (MORA), also known as the Gelb appliance.4,5,7 This is a removable, diagnostic appliance that repositions the mandible by engaging the mandibular molars and some premolars bilaterally, while leaving the cuspids and incisors uncovered. The two sides are connected via a sublingual bar. This design is phonetically neutral and generally better accepted by patients (Fig. 1).
Fig. 1
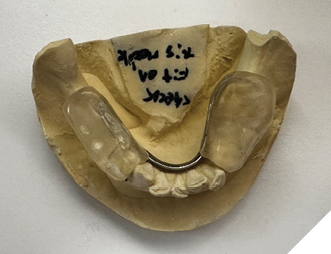
Patients are instructed to wear the appliance consistently, removing it only during meals. The increased VDO changes the length of the masticatory muscle fibers, which in turn reduces muscle activity. Additionally, shifting occlusal contact toward the molars brings the load closer to the fulcrum—the TMJ—thereby reducing stress on the system.
This shift benefits the joints, particularly in cases where TMD is of arthrogenic origin rather than myogenic.5,7 After 2–4 months of wearing the Gelb appliance, the mandible typically settles into a new relation with the cranium, with the condyles assuming a new position within the fossae.4,6 Symptom relief is associated with a more optimal and comfortable condylar position, leading to muscular relaxation. Achieving functional equilibrium of the bone and muscle components of the stomatognathic system represents Phase I of treatment.
Phase II focuses on stabilizing the jaw position by reproducing the VDO established with the Gelb appliance—via orthodontics, removable partial overdentures, fixed restorations, or a combination thereof.1–4,6,14 Without this second phase, relapse is likely.6,7
Adjusting VDO and introducing the palatal jig
In most cases, the Gelb appliance significantly increases the VDO. Its position and size are determined using a Lucia jig or leaf gauge, with the bite registered in the patient’s habitual centric position.8 It’s important to clarify that although the Lucia jig is a muscle deprogramming appliance originally designed to record centric relation (CR),9 we use it to control and maintain a tension-free increase in VDO.
As a result, the appliance typically creates an open bite in the anterior region. Following the protocol, temporary acrylic provisional restorations are then inserted and periodically adjusted. However, prolonged use of cemented acrylic provisionals can lead to damage of the prepared teeth, and simultaneously recording the occlusion for definitive restorations becomes difficult unless a fully adjustable articulator is used.
To address this, we developed a modified protocol. Patients return regularly for Gelb appliance adjustments, with gradual reductions in VDO until light contact is established between maxillary and mandibular incisors, while maintaining strong bilateral contacts in the premolar and molar regions. Patients are monitored for TMJ or muscular symptoms, and in our experience, none have been reported.
This treatment VDO—higher than the pre-treatment VDO but lower than the initial VDO with the Gelb appliance—becomes the basis for definitive restoration.
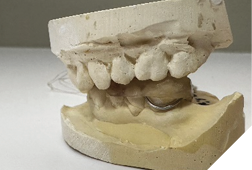
Next, a palatal jig is fabricated using fast-setting acrylic resin (Duralay) on the maxillary cast. It engages the palatal and lingual surfaces of the maxillary incisors and cuspids and is secured with dental floss embedded in the resin to prevent swallowing (Fig. 2).
Fig. 2
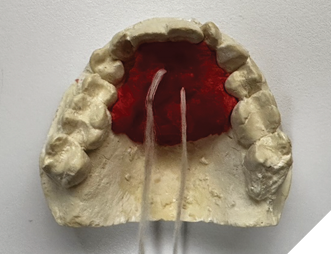
Once inserted and adjusted to establish simultaneous occlusal contacts in conjunction with the Gelb appliance, the palatal jig acts as a vertical stop for mandibular closure at the treatment VDO. With incisal edges and occlusal surfaces exposed, reliable occlusal registration becomes possible.
Final steps and outcomes
With the palatal jig securing the VDO, teeth can be prepared, occlusion registered, and final restorations fabricated and inserted simultaneously at the treatment VDO. We aim for an occlusal scheme based on cuspid guidance, which has been well tolerated by our patients. Others have reported that both cuspid guidance and group function—limited distally to the mesiobuccal cusp of the first molar10–13—reduce EMG activity of the masticatory muscles.
Following permanent insertion, a follow-up appointment is scheduled for occlusal contact assessment—occlusal adjustments are nearly always required. Based on case specifics, the need for an anti-bruxism appliance is evaluated.
In a prior article,14 we presented two cases using the palatal jig: one treated with bilateral fixed bridges and another with a removable denture.
We now present a third case, combining single crowns, composite restorations, and a removable partial denture.
A 72-year-old Caucasian female presented with long-standing TMJ discomfort and missing teeth. She was diagnosed with partial mandibular edentulism (missing 37, 45, 46, 47), generalized attrition, and arthrogenic TMD due to posterior bite collapse. Her periodontal condition was stable.
After informed consent, Phase I began with delivery of a Gelb appliance (Fig. 3ABC), which was adjusted periodically until achieving the treatment VDO. Phase II involved stabilization at this VDO. Teeth 36, 35, 43, and 44 were prepared simultaneously, and impressions (Henry Schein VP MIX) and bite registration (Kopy ultra-fast VPS) were taken using the palatal jig.
Fig. 3A

Fig. 3B

Fig. 3C
Temporary crowns (Maxitemp HP) compatible with the Gelb appliance were placed. Ten days later, single zirconia crowns (Argen YZ; Shaw Lab, Kingston, Ontario) were permanently cemented using 3M Ketac Cem. Teeth 34 and 33 were built up with composite (Activa, Pulpdent) to restore occlusal contact at the treatment VDO (Fig. 4).
Fig. 4

Finally, a cast lower partial denture (Shaw Lab, Kingston, Ontario) was fabricated (Fig. 5ABC). The occlusal design followed anterior/cuspid guidance (Fig. 6). After insertion and minor adjustments, the patient reported comfort and complete resolution of joint symptoms.
Fig. 5A

Fig. 5B

Fig. 5C

Fig. 6A

Fig. 6B

Conclusion
We believe this technique represents a significant advancement in the treatment of complex cases involving altered or increased VDO. The use of a palatal jig offers a safe, predictable method for maintaining and registering the treatment VDO, eliminating the need for prolonged use of acrylic provisionals. It also serves as a reference during removable partial denture fabrication, contributing to overall clinical efficiency and patient satisfaction. 
Oral Health welcomes this original article.
References
- Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984;52(4):467–74.
- Patel MB, Bencharit S. A treatment protocol for restoring occlusal vertical dimension using an overlay removable partial denture as an alternative to extensive fixed restorations: A clinical report. Open Dent J. 2009;3:213–8.
- Carlsson GE, Magnusson T. Management of temporomandibular disorders in the general dental practice. Chicago: Quintessence Publishing; 2004. p. 128–9.
- Gelb H, Bernstein I. Clinical evaluation of two hundred patients with temporomandibular joint syndrome. J Prosthet Dent. 1983;49(2):234–43.
- Gelb H. An orthopedic approach to occlusal imbalance and temporomandibular joint dysfunction. Dent Clin North Am. 1979;23(2):333–49.
- Gelb H. Evaluation of static centric relation in the temporomandibular joint dysfunction syndrome. Dent Clin North Am. 1975;19(3):617–29.
- Greene CS, Menchel HF. The use of oral appliances in the management of temporomandibular disorders. Oral Maxillofac Surg Clin North Am. 2018;30(3):265–77.
- Fukushima S. A controversy with respect to occlusion. Jpn Dent Sci Rev. 2016;52(3):49–53.
- Lucia VO. A technique for recording centric relation. J Prosthet Dent. 1964;14(3):492–505.
- Williamson EH, Lundquist DO. Anterior guidance: Its effect on electromyographic activity of the temporal and masseter muscles. J Prosthet Dent. 1983;49(6):816–23.
- Shupe RJ, Mohamed SE, Christensen LV, Finger IM, Weinberg R. Effects of occlusal guidance on jaw muscle activity. J Prosthet Dent. 1984;51(6):811–8.
- Manns A, Chan C, Miralles R. Influence of group function and canine guidance on electromyographic activity of elevator muscles. J Prosthet Dent. 1987;57(4):494–501.
- Landulpho AB, Silva E, Silva FA, Vitti M. Electromyographic evaluation of masseter and anterior temporalis muscles in patients with temporomandibular disorders following interocclusal appliance treatment. J Oral Rehabil. 2004;31(2):95–8.
- Topouzov V, Lee J. Multidisciplinary approaches to restoring vertical dimension of occlusion: Two clinical case studies of collapsed bite and symptoms of TMJ pain dysfunction syndrome. Oral Health. 2025;115(2):32–8.
About the authors

Dr. Venelin Topouzov is a general dentist in private practice in Cornwall, Ontario.

Dr. Justin Lee is a general dentist in private practice in Cornwall, Ontario.