
When should I refer a child to an orthodontist? Many dentists refer to an orthodontist once a child exfoliated their primary teeth and have a substantial number of permanent teeth. There are, however, many circumstances where it is beneficial or even necessary to make an early referral. The American Association of Orthodontists recommend that a child have an orthodontic assessment between the ages of 7-8. Having an assessment at this seemingly young age allows for the orthodontist to help with the early detection and treatment of many orthodontic issues. Here is a list of 10 reasons for an early referral to an orthodontist.
1. Thumb or Finger Sucking Habit
Thumb sucking habits can be one of the most difficult habits to break in a small child. Many children with a thumb or finger sucking habit have been doing it since birth and do it typically when they are tired, upset, or just to comfort themselves. Aggressive and continuous sucking habits, including the use of a pacifier, can lead to a significant malocclusion. These habits are associated with anterior open bites, posterior crossbites, high palate, and a large overjet (Fig. 1). These habits should be stopped by the eruption of the first permanent tooth. A habit breaking appliance such as a thumb crib and a subsequent Rapid Palatal Expander (RPE) may be necessary to stop the habit and correct the malocclusion, respectively.
Fig.1

2. Space Maintenance or Regaining
When a child loses a tooth prematurely due to trauma or caries/infection, the result could be space loss. For example, if a first primary molar is lost prior to the eruption of the first primary molar in that quadrant, then a band and loop space maintainer should be placed to save the space form closing. Although any dentist could fabricate a space maintainer, many don’t feel comfortable doing so. In the case of space regaining, an active appliance is required to move the teeth into a more favorable position. These usually require an orthodontist, and an early referral is warranted.
3. Congenitally Missing Teeth
Congenitally missing teeth present challenges that require an orthodontic treatment plan early on to optimize the success of the treatment. The most commonly missing permanent teeth are the third molars, the maxillary lateral incisors, and the mandibular second molars. If a primary tooth is missing, then almost always the successive tooth is also missing. If upon intraoral examination or radiographic assessment it is determined that a permanent tooth is congenitally missing, then an early orthodontic referral is necessary. In many cases the permanent cuspid can move into the space of the missing lateral incisor. With some minor reshaping of the lateral incisor, one can achieve an excellent result. In other cases, permanent implants are required to replace the missing teeth. A comprehensive long-term treatment plan is required to get the child through orthodontic treatment and the subsequent placement of the implants once the individual stops growing.
4. Class III Occlusion
A Class III occlusion is one of the most challenging malocclusions for an orthodontist to treat (Fig. 2). Due to the uncertainty of mandibular growth in these cases, Class III occlusions must be watched very closely from a very young age. If not treated or detected early, these cases could result in jaw surgery to correct the malocclusion. One tool that orthodontists use to treat a Class III occlusion in a young patient is a RPE. By expanding the maxilla with a RPE, the mandible can oftentimes position itself in a more favorable position (Class I occlusion). As a rule, refer these cases early to the orthodontist so that they can optimize growth and help prevent eventual surgery.
Fig.2
5. Excessive Overjet (Trauma Risk)
The overwhelming majority of teeth that are traumatized in a fall or sporting accident are the maxillary anterior teeth. An excessive overjet often associated with a Class II occlusion (Fig. 3) puts the maxillary incisors at risk for fracture, lateral luxation, intrusion or avulsion. These injuries can be very serious and present the patient with life-long challenges. A risk assessment should be completed by the dentist to determine if an early referral to an orthodontist is warranted to help prevent dental trauma. If a child plays contact sports or is very active and they have a Class II occlusion with an excessive overjet, a custom fit sports guard should be fabricated and worn to prevent dental injuries. Phase 1 orthodontic treatment whereby in the mixed dentition, the maxillary incisors are moved back to decrease the overjet would be beneficial in these cases.
Fig.3

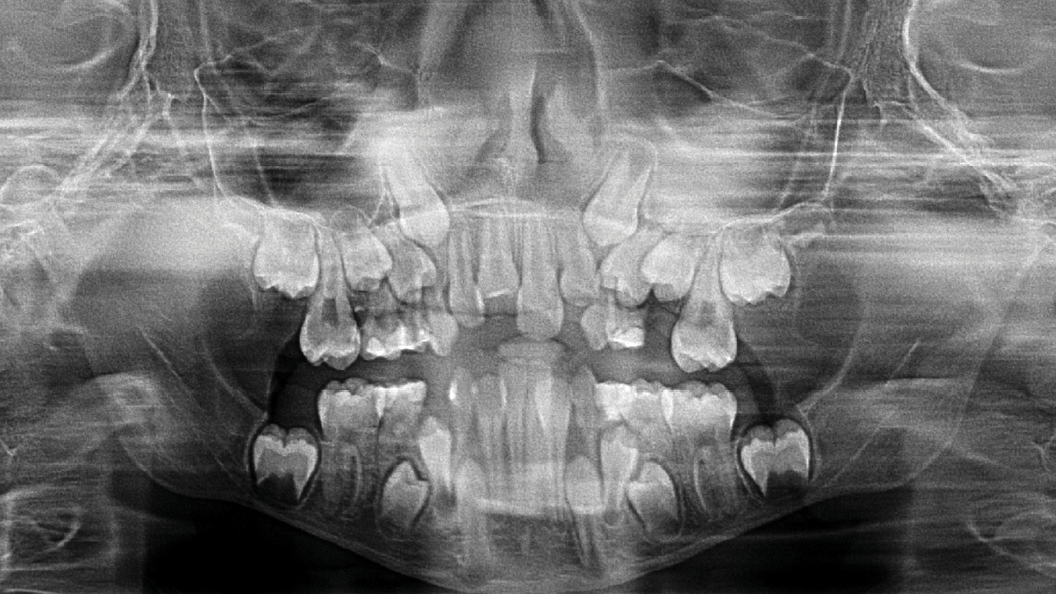
6. Ectopic Eruption
During development, teeth can erupt and position themselves where they shouldn’t. The ectopic eruption of permanent teeth can result in damage to the adjacent teeth and a significant malocclusion. During the dental examination and radiographic assessment of a developing and growing child, the dentist should be looking for signs that the teeth are not where they should be. In a crowded dentition, it is not uncommon to see the ectopic eruption of the maxillary first permanent molars or the maxillary permanent canines. The ectopic eruption of the permanent first molars are usually identified on bitewing radiographs. Due to the large size of the molar or the lack of arch length, the first molar gets impeded by the distal aspect of the second primary molar. Many of these cases will resolve themselves as the child grows. In the case of ectopically erupting maxillary canines, a panorex is necessary for diagnosis (Fig. 4). If the canines are positioned on an angle and have the potential to damage the roots of the lateral incisors, then an early referral to an orthodontist is warranted. In many cases the extraction of the maxillary primary canines will be recommended.
Fig. 4
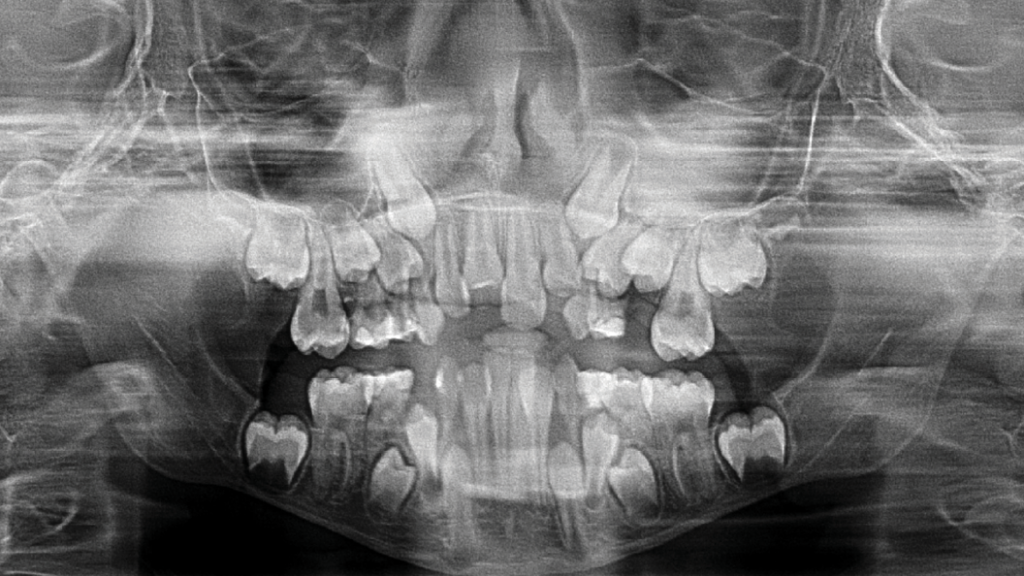
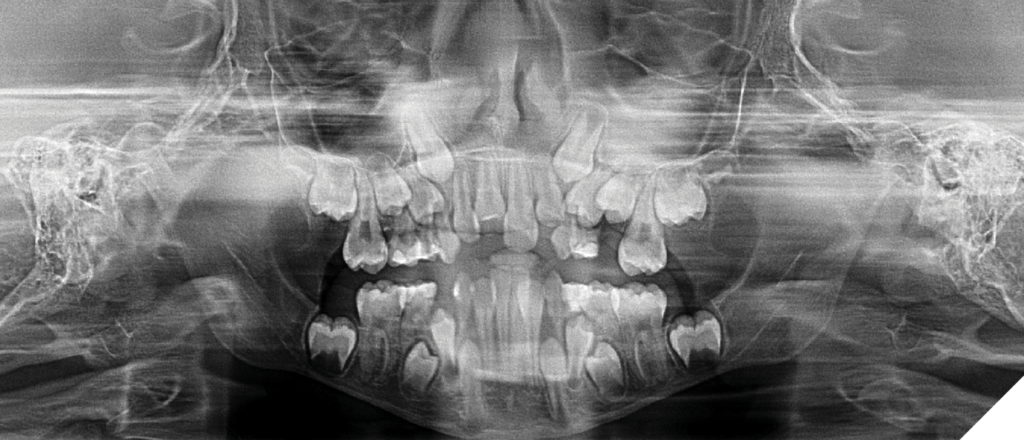
7. Posterior Crossbite
A posterior crossbite is an easy malocclusion to fix if treated early. Posterior crossbites can be the result of thumb sucking, mouth breathing, or simple inheritance. A unilateral or bilateral crossbite (Fig. 5) is often associated with a mandibular shift laterally. The palatal suture along the midline of the palate is not calcified in a growing child and, therefore, allows for expansion if manipulated. If left untreated this can lead to facial asymmetry and significant malocclusion. An appropriate time to treat these cases with a RPE is after the eruption of the first permanent molars. Expanding the maxillary arch with an RPE will treat the mandibular shift and increase the arch length resulting in decreased crowding. In many cases no further orthodontic treatment is required. An early referral to an orthodontist is required in these cases.
Fig. 5

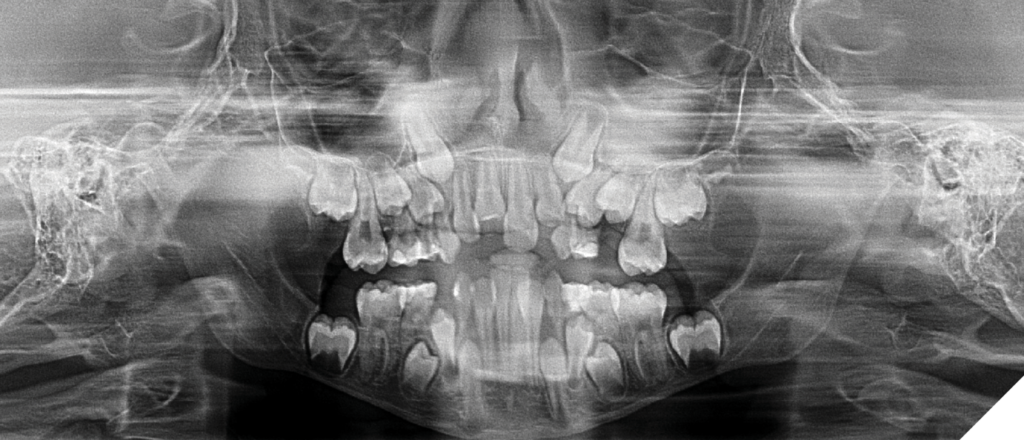
8. Excessive Crowding
In the cases where there just is not enough space for the teeth to fit then an early referral to an orthodontist can be helpful. The lack of arch length required for the teeth may require serial extractions to help facilitate their eruption (Fig. 5). A treatment plan formulated by an orthodontist will help guide the treatment of these cases.
9. Craniofacial Anomalies
Craniofacial anomalies can introduce significant challenges for both the patient and the dentist. These cases can be very complex and an early referral to an orthodontist is required. Patients with craniofacial abnormalities can have missing teeth, large or small sized teeth, serious jaw discrepancies, and clefted lip and/or palate, just to name a few. These patients are often treated with a team of dental and medical professionals and their success is dependent on the comprehensive and attentive teamwork of these professionals. Some cases such as Amelogenesis Imperfecta or Dentinogenesis Imperfecta may only affect teeth, where others such as Cleft Lip and Palate can involve many parts of the face. Many of these patients have significant cognitive impairment and require the care of a pediatric dentist as well. A skilled orthodontist is an essential part of the team that treats these patients, and an early referral must be made.
In conclusion, the early referral of patients to an orthodontist can be beneficial to the overall ease of treatment and the result of the orthodontic treatment. The early detection of dental issues by the dentist is necessary. A dentist’s true understanding of growth and development will help their young patients immensely.
—
References
- Christopherson, E.A., Briskie, D. and Inglehart, M.R. (2009), Objective, Subjective, and Self-Assessment of Preadolescent Orthodontic Treatment Need – A Function of Age, Gender, and Ethnic/Racial Background?. Journal of Public Health Dentistry, 69: 9-17
- Proffit WR, Fields HW Jr., Moray LJ.Prevalence of malocclusion and orth-odontic treatment need in the UnitedStates: estimates from the NHANES IIIsurvey. Int J Adult Orthodon OrthognathSurg. 1998;13:97-106.
- Tausche E, Luck O, Harzer W. Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need.Eur J Orthod. 2004;26:237-44.
- Inglehart MR, Bagramian RA, editors.Oral health-related quality of life.Chicago (IL): Quintessence PublishingCompany; 2002.
- Inglehart MR, Bagramian RA. Oral health-related quality of life – introduction and overview. In: Inglehart MR, Bagramian RA, editors. Oral health and quality of life. Chicago (IL): Quintessence Publish-ing Company; 2002.

Dr. Farkouh is a pediatric dentist working in private practice in Toronto, Canada. He is on staff in the Department of Dentistry at The Hospital for Sick Children in Toronto, Canada. He is the Pediatric Dental Editor for Oral Health Journal.
